 NITO100/ISTOCK/GETTY IMAGES PLUS
NITO100/ISTOCK/GETTY IMAGES PLUS
Supporting the Transgender Community
By reducing healthcare disparities, providing nonjudgmental care, and addressing areas of high risk, oral health professionals can play a unique role in encouraging oral and systemic health in this patient population.
This course was published in the September 2020 issue and expires September 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Recognize determinants of health for the transgender community.
- Apply dental hygiene management to provide patient-centered care for the transgender patient.
- Identify risk factors for systemic conditions for trans men and women.
- Identify pharmacological interventions for transgender people.
Transgender individuals identify their gender, expression, and behavior differently than their biological sex established at birth.1–3 An estimated 1.4 million Americans identified as transgender in 2014 according to the Williams Institute at the University of California, Los Angeles School of Law.4 The number of people in the transgender community has doubled since 2011, and it is suspected this number may be even higher. Transgender people are often underreported due to familial, social, and psychological stressors related to public acceptance. Research has estimated about one in every 250 adults identify with the transgender community, with the majority being young adults.4,5 Dental hygienists need to understand the complexity of social determinants of health and the impact of hormone replacement therapy during transitioning on oral and systemic health to provide patient-centered care.
DETERMINANTS OF HEALTH
This marginalized community encounters a complex layer of stigmas resulting in inequalities, including rejection of human rights.2 Fewer than 18 states prohibit gender identity discrimination regarding employment, housing, education, and public accommodations (eg, restaurants, retail stores, hotels, theaters, medical offices, and pharmacies).6 The structural differences experienced by this community result in an increase of barriers to oral and general healthcare. In addition, without legal protection, this community is at higher risk for unemployment, contributing to poverty and homelessness. As a result, some people in the transgender community turn to sex work.7 Additionally, transgender individuals may face harassment, violence, and gender crimes.2,6 Currently, there is no tracking system in the United States to document transgender homicide; however internationally, an estimated one murder of a transgender individual occurs every 3 days.8 These factors increase the vulnerability of this community on an individual level, resulting in adverse health outcomes.2
MENTAL HEALTH AND WELL-BEING
The discrimination, social stigma, and harassment faced by transgender individuals increase the risk for mental health disorders and addiction problems.5,9–12 Stress among people in the transgender community can vary, depending on the transition process, ability to cope, and support systems.9 Within the transgender population, 41% reported experiencing discrimination, verbal abuse, and violence, which raise the risk for anxiety and depression.9,13 Transgender individuals taking hormone replacement therapy (HRT) report positive effects on quality of life, with reduced anxiety and depression, as HRT changes the physical body characteristics to align with psychological gender.2,14
The risk of chemical dependency among transgender youth is 2.5 times to 4 times higher than their peers due to trans-related discrimination and mental health disorders. Individuals who were sexually assaulted or verbally threatened within the past year reported greater heavy episodic drinking than those who identified themselves as cisgender (gender corresponds with birth sex).10,11,15
Additionally, suicide and suicidal behaviors are more prevalent within the transgender community. Environmental factors that contribute to suicidal behaviors include lack of family support, harassment, victimization, and gender violence.16,17 Interventions to increase social inclusion and reduce transphobic experiences may help to decrease the prevalence of suicidal behaviors, mental health disorders, chemical dependencies, and adverse health outcomes among the transgender community.17
DENTAL HYGIENE MANAGEMENT
The dental hygiene standard of care is no different for a transgender person than a cisgender person.18 However, determinants of health, use of HRT during the transition process, risk of oral-systemic conditions, and potential pharmacological interventions need to be considered when developing the dental hygiene care plan. Current dental hygiene risk management assessment models should be used to prevent oral and systemic diseases and promote general health and well-being.
Some transgender people undergo HRT during the transition process, and may choose gender-affirmation surgery to achieve their desired gender identity. However, gender affirmation surgery is not a prerequisite for transitioning. HRT is the primary medical intervention pursued to alter physical characteristics to match gender identity. HRT is a cross-sex hormone therapy consisting of sex hormones and various hormonal medications administered during the transition process.1 Dental hygienists need to be knowledgeable of the different HRTs when providing individualized patient-centered care.
Transwomen are prescribed estrogens or antiandrogens as feminizing hormone therapy. Estrogen is a hormone responsible for female secondary sex traits such as breast growth, pubic and underarm hair, and the initiation of menstrual cycles.19 The expected outcomes after 18 months to 24 months of estrogen therapy include breast growth, decrease in body and facial hair growth, decreased testicular size and erectile function, and an increase of body fat.1,19,20 Antiandrogens are sex hormone antagonists to prevent biological effects in the body, and are often prescribed for transgender girls or adolescents to prevent testosterone production.19
Transmen are prescribed steroid hormones or androgens (testosterone, dihydrotestosterone, and androstenedione). Testosterone is responsible for physical traits of men, such as muscle mass, deepened voice, and facial and body hair. In transmen, testosterone is responsible for the suppression of the menstrual cycle and decreased production of estrogen from the ovaries. After cross-sex hormone therapy is initiated, physical outcomes can appear within several weeks to months. Physical changes may include oily skin/acne, cessation of menstrual cycle, voice deepening, facial/body hair, body fat distribution, clitoral enlargement, vaginal atrophy, increased muscle mass, and scalpel hair loss.21
Transwomen on long-term estrogen replacement have a higher risk profile compared to transmen.19 Negative systemic effects from estrogen therapy include cardiovascular and cerebrovascular disease, venous thrombosis, pulmonary embolism, seizures, and breast cancer.19,22–25 Studies have shown the risk of cardiac events, venous thrombosis, and pulmonary embolism is highest in the first year of estrogen therapy.19 Individuals undergoing HRT have a two-fold to five-fold increased risk of venous thrombosis and seizures compared to nonusers.17 Side effects to antiandrogen therapy are sexual dysfunction, infertility, and osteoporosis. Although breast cancer rates in transwomen are comparable to the general population, the risk is heightened by prolonged duration of estrogen therapy.19
Transmen face a higher risk of metabolic disease due to an increase in abdominal fat caused by the use of steroid hormones or androgens. Some may also undergo unexplained menses and experience increased risks of polycystic ovarian disease due to high levels of androgens and endometrial cancer.19 The impact of testosterone on cardiovascular health and hypertension is conflicting; however transmen with underlying risk factors may be prone to these systemic diseases.19,22,23 Sleep apnea in transmen may become worse with testosterone therapy, thus increasing risk factors for cardiovascular disease.19,26 Additionally, testosterone increases hemoglobin by 5% to 7%, therefore posing a greater risk for polycythemia in this patient group. Complications associated with polycythemia include stroke, myocardial infarction, and deep vein thrombosis.26 Additionally, studies have indicated a correlation between testosterone and psychiatric effects, including mania and aggression.19
Osteoporosis/osteopenia is a risk factor for people in the transgender community due to the effects of sex hormones on bone mineral density. Both transwomen and transmen should take daily supplements of vitamin D and calcium in addition to regular weight-bearing exercises to maintain muscle mass. Although there is conflicting evidence regarding the effect of testosterone on bone mineral density, transmen are at elevated risk for osteoporosis/osteopenia due to decreased estrogen.20 As such, this patient group should undergo frequent bone mineral density screenings.27 Furthermore, people in this community may have altered liver function and increased liver enzymes from either estrogen or testosterone therapy.19
As transgender individuals may be at increased risk for cardiovascular and metabolic disease and cardiovascular disase and diabetes are associated with periodontal disease risk, this patient population should be assessed regularly for any changes in periodontal status.28–31 Dental hygienists may implement dietary counseling to reduce cardiovascular, cerebrovascular, and metabolic disease risk.18
ADDITIONAL RISK FACTORS
Dental hygienists should be mindful of the complex determinants of health that impact this community. Transgender people may have an increased risk of dental caries as a result of reduced salivary flow from HRT, sex hormones, prescribed medications, or depression-related lack of daily self-care. Caries risk assessment and management should be incorporated into the treatment plan with recommendations for oral hygiene instruction, fluoride use, dental dietary counseling, and 3-month to 6-month recare intervals.18
Transgender patients with xerostomia may benefit from over-the-counter or prescription medications to alleviate dry mouth symptoms and promote caries prevention. Reduced salivary flow increases the risk for periodontal inflammation due to the plaque buildup around oral soft and hard tissues. Due to complex risk factors, early intervention may be suggested to prevent periodontal and caries disease progression.
Evidence indicates the transgender community is at increased risk for human immunodeficiency virus (HIV) and other sexually transmitted diseases, such as human papillomavirus (HPV).5,7,12 In 2015, the rate of new diagnoses for HIV among transgender individual was three times higher than the national average.11 Additionally, transgender women are at risk for HPV, which causes oral and pharyngeal cancers.5,12 Dental hygienists may want to recommend the HPV vaccination to this population.32,33 Additionally, completing a comprehensive oral cancer screening at each visit is key to identify early lesions.33
PROVIDER ACCEPTANCE
Transgender individuals may encounter discrimination and hostility from healthcare providers when disclosing their status upon medical history review.13 In addition, this community has reported “trans broken arm syndrome” during patient-provider experiences. This term is used to describe healthcare providers associating medical issues solely based on being transgender.34 To prevent trans broken arm syndrome during patient care, dental hygienists need to be competent and ethical providers who demonstrate respect and inclusive patient-centered care for the transgender community. In a dental setting, providing a nonjudgmental, supportive, and safe environment may enhance provider acceptance by developing trust during patient care.
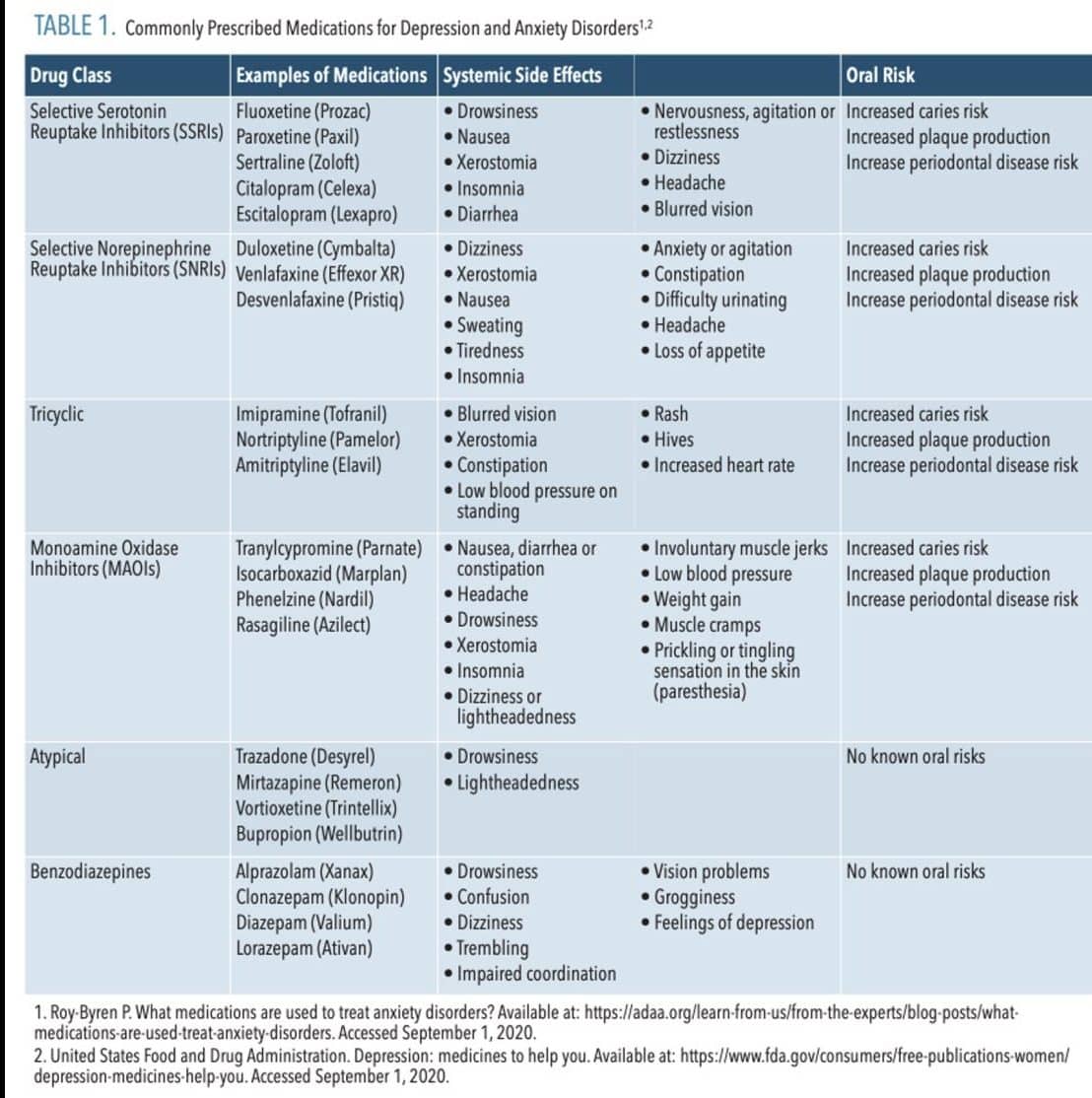
PHARMACOLOGICAL CONSIDERATIONS
Transgender people may also be prescribed medications in addition to HRT to treat symptoms related to mental health disorders and/or chemical dependencies. The increased incidence of depression and anxiety among the transgender community is usually managed by prescribing antidepressants and/or antianxiety medications.
Social history may include tobacco (smoke, smokeless, or vape), prescription medications or substance/alcohol abuse resulting in a higher risk profile for oral-systemic conditions.18 Dental hygienists delivering motivational interviewing strategies to support positive behavior change during patient care may reduce these social habits.35 In addition, social history may include gender violence, physical and emotional abuse, and psychiatric conditions.5,9,11,12,18 Dental hygienists should be prepared to provide referrals to a physician, social worker, and/or a therapist/counselor.
CONCLUSION
Dental hygienists can play a unique role in supporting the transgender community and are instrumental in the prevention of oral-systemic diseases. Dental hygienists have the opportunity to initiate change by reducing determinants of health, increasing healthcare equality, and providing nonjudgmental patient-centered care and referrals for trans people. The lack of longitudinal evidence on the impact of long-term sex hormone therapy on mental health, well-being, and systemic health supports the need for continued training and education for dental hygienists to provide quality care for this patient group.
![]() REFERENCES
REFERENCES
- Unger CA. Hormone therapy for transgender patients. Transl Androl Urol. 2016;5:877–884.
- White Hughto JM, Reisner SL, Pachankis JE. Transgender stigma and health: a critical review of stigma determinants, mechanisms, and interventions. Soc Sci Med. 2015;147:222–231.
- Eden K, Wylie K, Watson E. Gender dysphoria: recognition and assessment. Adv Psychiatr Treat. 2012;18:2–11.
- Flores AR, Herman JL, Gates GJ, Brown TNT. How many Adults Identify as Transgender in the United States? The University of California, Los Angeles: The Williams Institute; 2016:13.
- Meerwijk EL, Sevelius JM. Transgender population size in the United States: a meta-regression of population-based probability samples. Am J Public Health. 2017;107:e1–e8
- Human Rights Campaign Foundation. 2018 State Equity Index: A Review of State Legislation Affecting the Lesbian, Gay, Bisexual, Transgender, and Queer Community and aLook Ahead in 2019. Available at: https://assets2.hrc.org/files/assets/resources/SEI-2018-Report.pdf. Accessed August 25, 2020.
- Nemoto T1, Bödeker B. Social support, exposure to violence and transphobia, and correlates of depression among male-to-female transgender women with a history of sex work. Am J Public Health. 2011;101:1980–1988.
- Stotzer RL. Data sources hinder our understanding of transgender murders. Am J Public Health. 2017;107:1362–1363.
- Yang MF, Manning D, van den Berg JJ, Operario D. Stigmatization and mental health in a diverse sample of transgender women. LGBT Health. 2015;2:306–312.
- Day JK, Fish JN, Perez-Brumer A, Hatzenbuehler ML, Russell ST. Transgender youth substance use disparities: results from a population-based sample. J Adolesc Health. 2017;61:729–735.
- Johns MM, Lowry R, Andrzejewski J, et al. Transgender identity and experiences of violence victimization, substance use, suicide risk, and sexual risk behaviors among high school students—19 states and large urban school districts, 2017. MMWR Morb Mortal Wkly Rep. 2019;68:67–71.
- Sharma A, Kahle E, Todd K, Peitzmeier S, Stephenson R. Variations in testing for HIV and other sexually transmitted infections across gender identity among transgender youth. Transgend Health. 2019;4:46–57.
- Bradford J, Reisner SL, Honnold JA, Xavier J. Experiences of transgender-related discrimination and implications for health: results from the Virginia transgender health initiative study. Am J Public Health. 2013;103:1820–1829.
- Rowniak S, Bolt L, Sharifi C. The effect of cross-sex hormones on the quality of life, depression and anxiety of transgender individuals: a quantitative systematic review. JBI Database System Rev Implement Rep. 2019 Apr 23. Epub ahead of print.
- Coulter RWS, Blosner JR, Bukowski LA, Herrick AL, Siconolfi DE, Stall RD. Differences in alcohol use and alcohol-related problems between transgender- and nontransgender-identified young adults. Drug Alcohol Depend. 2015;154:251–259.
- Wolford-Clevenger C, Cannon CJ, Flores LY, Smith PN, Stuart GL. Suicidal risk among people: a prevalent problem in critical need of empirical and theoretical research. Violence Gend. 2017;4:69–72.
- Bauer GR, Scheim AI, Pyne J, Travers R, Hammond R. Intervenable factors associated with suicide risk in transgender persons: a respondent driven sampling study in Ontario, Canada. BMC Public Health. 2015;15:525.
- American Dental Hygienists’ Association. Standards for Clinical Dental Hygiene Practice. Available at: adha.org/resources-docs/2016-Revised-Standards-for-Clinical-Dental-Hygiene-Practice.pdf. Accessed August 25, 2020.
- Bourns A. Guidelines and Protocols for Hormone Therapy and Primary Health Care for Trans Clients. Toronto, Ontario: Sherbourne Health Centre; 2009:72.
- Mayo Clinic. Feminizing Hormone Therapy. Available at: .mayoclinic.org/tests-procedures/mtf-hormone-therapy/about/pac-20385096. Accessed August 25, 2020.
- Mayo Clinic. Masculinizing Hormone therapy. Available at: mayoclinic.org/tests-procedures/ftm-hormone-therapy/about/pac-20385099. Accessed August 25, 2020.
- Streed CG, Harfouch O, Marvel F, Blumenthal RS, Martin SS, Mukherjee M. Cardiovascular disease among transgender adults receiving hormone therapy: a narrative review. Ann Intern Med. 2017;167:256–267.
- Getahun D, Nash R, Flanders WD, et al. Cross-sex hormones and acute cardiovascular events in transgender persons: a cohort study. Ann Intern Med. 2018;169:205–213.
- Henderson VW, Lobo RA. Hormone therapy and the risk of stroke: perspectives ten years after the Women’s Health Initiative trials. Climacteric. 2012;15:229–234.
- Khan J, Schmidt RL, Spittal MJ, Goldstein Z, Smock KJ, Greene DN. Venous thrombotic risk in transgender women undergoing estrogen therapy: a systematic review and meta-analysis. Clin Chem. 2019;65:57–66.
- Floras JS. Sleep apnea and cardiovascular disease: an enigmatic risk factor. Circ Res. 2018;122:1741–1764.
- Centre of Excellence for Transgender Health. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People. San Francisco: University of California San Francisco; 2016:199.
- Teles R, Wang CY. Mechanisms involved in the association between periodontal diseases and cardiovascular disease. Oral Dis. 2011;17:450–461.
- Aoyama N, Suzuki JI, Kobayashi N, et al. Increased oral porphyromonas gingivalis prevalence in cardiovascular patients with uncontrolled diabetes mellitus. Int Heart J. 2018;59:802–807.
- Sanz M, Ceriello A, Buysschaert M, et al. Scientific evidence on the links between periodontal diseases and diabetes: consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the international Diabetes Federation and the European Federation of Periodontology. J Clin Periodontol. 2018;45:138–149.
- Cavero-Redondo I, Peleteiro B, Álvarez-Bueno C, Rodriguez-Artalejo F, Martínez-Vizcaíno V. Glycated haemoglobin A1c as a risk factor of cardiovascular outcomes and all-cause mortality in diabetic and non-diabetic populations: a systematic review and meta-analysis. BMJ Open. 2017;7:e015949.
- Walker KK, Jackson RD, Sommariva S, Neelamegam M, Desch J. USA dental health providers’ role in HPV vaccine communication and HPV-OPC protection: a systematic review. Hum Vaccin Immunother. 2019;8:1–7.
- Stull CL, Lunos S. Knowledge, attitudes and practices regarding human papilloma virus communication and vaccine advocacy among Minnesota dentists and dental hygienists. J Dent Hyg. 2019;93:33–42.
- Knutson D, Koch JM, Mitchell TA, Martyr MA. “Trans broken arm:” health care stories from transgender people in rural areas. J Res Women Gend. 2016;7:30–46.
- Arnett MC, Gwozdek A. Motivational interviewing for the clinical dental hygienist. Dimensions of Dental Hygiene. 2017;5(15):54–57.
From Dimensions of Dental Hygiene. September 2020;18(8):40-43.

{kind=link}