 MAY LIM / ISTOCK / GETTY IMAGES PLUS
MAY LIM / ISTOCK / GETTY IMAGES PLUS
Strategies to Support Dental Prostheses
Proper care will help maintain the longevity and service life of dental prostheses, while also supporting patient health.
This course was published in the May 2022 issue and expires May 2025. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the different types of fixed or removable prostheses.
- Discuss the appropriate cleaning methods for each type of prothesis.
- List the oral and medical concerns that should be considered with all patients who wear dentures.
Maintaining healthy soft tissue, gingiva, and bone structure following the implementation of a fixed or removable prosthesis is paramount to the therapy’s long-term success. Toward this goal, clinicians can help patients maintain their dental prostheses by educating them about the many factors affecting oral health and appliance longevity. In providing such information, oral health professionals must consider each patient’s oral health, general health, and comorbidities. Fungal infections, for example, are not uncommon in denture wearers.1
Many chemicals and tools are indicated for the care of an intraoral prosthesis, and clinicians should help guide patients, as some of these products are contraindicated for use with specific prostheses, or for patients presenting with certain medical comorbidities.
In addition, dentures are fabricated using multiple materials. Understanding which product works best for the denture being placed is paramount to achieving optimal long-term outcomes. This article will address appropriate care for various appliances.
Conventional Dentures
Because the need to treat edentulism is commensurate with an aging population, the demand for complete dentures is expected to continue.2 Maintaining complete denture cleanliness is crucial to minimize the amount of harmful oral microflora that will adhere to dentures. Several measures are needed to ensure denture maintenance throughout the life of the prosthesis;3 for example, when the patient is not wearing the denture, it should be placed in water to avoid distortion.1 There are multiple ways described in the literature to clean dentures, including:
- Brushing4
- Soaking in either commercial tablets or sodium hypochlorite (NaOCL) for 10 minutes, before being moved to water5
- Ultrasonic cleaning6
- Microwave disinfection7
According to the American College of Prosthodontists’ guidelines, denture adhesives may be used for severely compromised ridges after the fit has been fabricated to the limitations of the remaining tissues. While adhesives should not be used to compensate for poorly made or ill-fitting dentures, the use of denture adhesives may improve masticatory function. These products are available in gels, powders, and pads.
Applying gel adhesives should be done by adding three to four pea-size dots on the intaglio surface. Powder adhesives are used by lightly coating the intaglio surface after wetting the denture. Pad adhesives should be trimmed and placed within the confines of the intaglio surface. Excess amounts of all three types of adhesives should be removed.3
Following denture delivery, the patient should be examined after 1 day to 3 days to evaluate and make appropriate adjustments to the occlusion and tissue-bearing areas. The patient is encouraged to maintain constant communication with the oral health professional if further adjustments are necessary. A yearly recare visit should be scheduled to examine the dentures, attachments, and oral tissues.8
Implant-Retained Dentures
Implant-retained overdentures differ from conventional dentures by virtue of the implant component that aids retention. Yet they are also similar, as the prosthesis is tissue supported and should be fully extended, as would a conventional denture. Maintaining implant-retained overdentures entails caring for the attachments and inserts, as well as the denture itself.
Many attachment systems are available, and three of the most common are Locator attachments, O-ring attachments, and Hader bars. Studies have looked at how different denture cleaners affect the retention of these components, and what that could mean in a clinical setting. A study by Ayyildiz et al9 compared retention loss values in blue, pink, and clear Locator attachment inserts after immersion in three commonly used denture cleaners at 1 month, 3 months, and 12 months. The authors concluded that retention decreased in all three groups, with NaOCL having the greatest negative effect.
Likewise, the same findings were noted in studies by Nguyen et al10 and You et al.11 The Nguyen et al10 study reported that the studied mouthrinse increased the retentive values of pink Locator attachments, whereas other commercial cleaners did not statistically affect retention. In 2016, Kürkcüoğlu et al12 reported Locator attachment inserts (blue, pink, and clear) were affected differently when soaked in commercial solutions. Blue inserts were significantly negatively affected by cleaners containing sodium bicarbonate (NaHCO3) and NaOCL, while clear attachments were only affected by cleaners containing NaHCO3.12 Water temperature was found to impact the retention loss of Locator attachment inserts. A 2017 study found that immersing Locator attachment inserts in water at 140° F resulted in significantly increased retention loss compared to 68.0°F and 98.6°F water.13
Similarly, O-rings were found to be affected when immersed in denture cleaners. Studies conducted by Felipucci et al14 and Derafshi et al15 concluded that O-ring attachments suffered retention loss when placed in denture cleaners compared to water. It was also reported that NaOCL caused the most retention loss.14,15
Studying Hader clips, Varghese et al16 reported that yellow Hader clips did not suffer significant retention loss when immersed in commercial denture cleaners, as compared to water. In fact, the clips had increased retention values when immersed in NaOCL. However, the authors did not recommend the use of NaOCL, as this increase in retention may be the result of the Hader clips becoming more rigid.
Implant-Supported Fixed Complete Dentures
Full-arch fixed implant prostheses should be evaluated every 2 months to 6 months. Radiographic assessment should be conducted every 1 year to 2 years—or sooner if signs of peri-implantitis or peri-implant mucositis are present.17,18 During the maintenance visit, the patient’s history should be updated and a clinical exam performed to assess the prosthesis and peri-implant tissue. Probing depths and bleeding on probing around the implants should be documented and compared to the baseline probing depths recorded during prosthesis placement.18,19 Full-arch fixed implant prostheses need not be removed unless there is evidence of disease, a prosthetic complication, or a component misfit on the radiograph. If the prosthesis is removed, new screws should be used to reinsert the prosthesis.20 In addition, clinicians should educate patients and caregivers on how to clean under fixed appliances. Prostheses are maintained by brushing and additional oral hygiene tools, such as any combination of the following:
- Floss
- Water flossers
- Interdental brushes17
- Occlusal devices
While numerous over-the-counter products are available to care for various prostheses, a thorough understanding of the chemical components is essential to the long-term sustainability of the denture and oral supporting structures. This again speaks to the need for patient education from the dental team.
Care for Conventional Dentures
Many edentulous patients use conventional dentures. An investigation by Sharma et al21 noted the importance of patient education and proper oral hygiene for denture wearers. A patient presenting with a denture that has not been properly cared for may suggest a lack of patient education and/or a lack of interest on the clinician’s part to have the prosthesis last for many years.21–24 At the same time, a patient may have the knowledge, yet lack the physical or mental ability to clean the prosthesis.25 Harikrishnan et al26 and Peracini et al27 conducted studies with similar outcomes that assessed awareness of denture care results with five cleaning methods. They reported that patients used water, toothpaste, and/or a toothbrush combination to clean their dentures on a daily basis by:26,27
- Brushing with water
- Brushing with soap
- Brushing with toothpaste
- Soaking in mouthrinse
- Brushing and soaking in mouthrinse28
Consumer products used to soak a denture typically list sodium bicarbonate as the key ingredient. In addition, products commonly used to brush a denture are formulated to provide effective cleaning, yet without abrasive levels sufficient to damage the appliance.
Proper brushing will reduce bacterial and fungal growth on the denture and oral tissues. Oral candidiasis is found in 60% of healthy denture wearers, so educating patients about the type of brush to use for denture care is important.24,29 There is a difference in the coarseness of the bristles between a manual toothbrush and denture brush. The coarseness/hardness of the bristles of a regular toothbrush will increase the risk of developing roughness in the acrylic prosthesis and, subsequently, raise the incidence of bacterial growth on the denture.27,29,30 Along these same lines, brushing with vinegar, bleach, or baking soda may roughen dentures. The design of an end-tufted toothbrush will ensure easier cleansability of any attachments on the denture and implants (if present).
When a denture-wearing patient presents with candidiasis, both the oral cavity and denture should be treated to eliminate the fungal infection. In this scenario, the recommended treatment for candidiasis is 7 days to 10 days.31 Once the oral health professional has reviewed the patient’s medical history, the choice is made as to which drug is indicated to treat the oral fungus. The drug options are outlined in Table 1.
Educating patients about the importance of soaking the denture and not brushing the denture when Candida is present is also indicated. Dentures that are not treated raise the risk of patients developing mucosal lesions, inflamed mucosal tissues, and pneumonia.32 If the dentures have soft liners, they should be soaked in an enzyme plus neutral peroxide denture cleaning solution to minimize surface degradation.33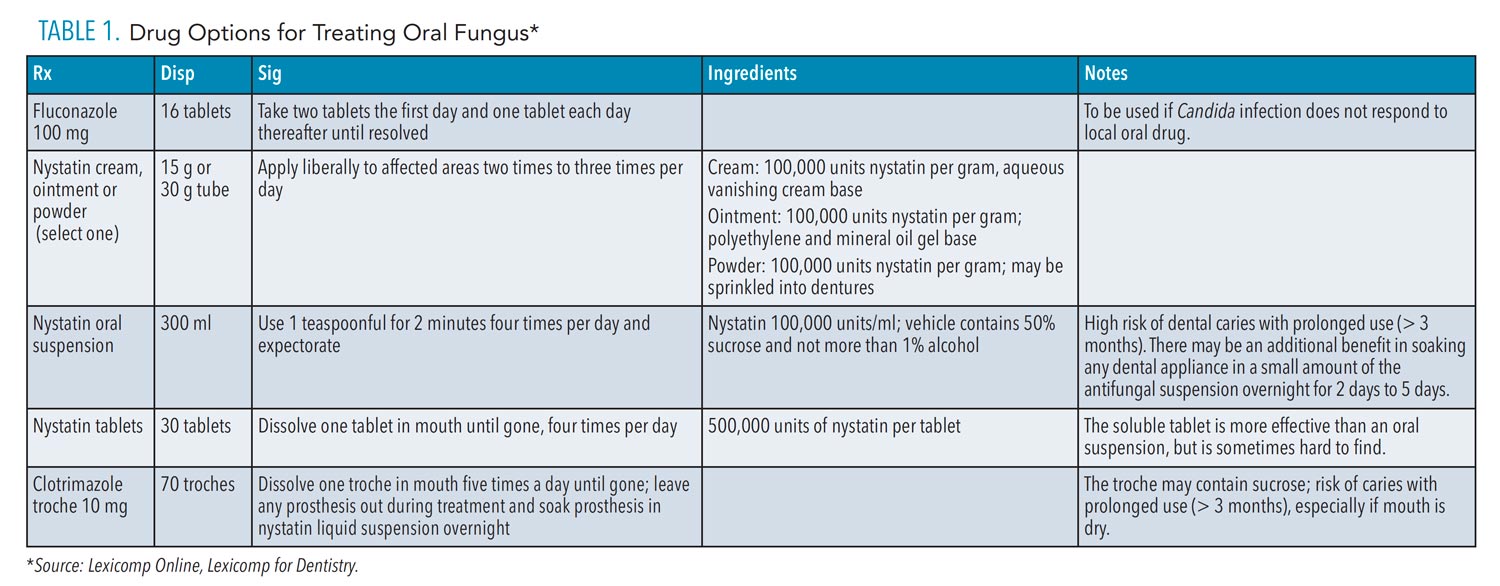
Medical Considerations
Oral and medical concerns that should be considered with all patients who wear dentures include:
Allergies. Completing a through medical history will help decrease the possibility of adverse events. One of the ingredients in denture cleaners is persulfate. Patients who are allergic to sulfur should evaluate each denture product they are considering to ensure this ingredient is not incorporated.
Toxicity. Denture cleaners can be toxic if swallowed. Stressing the importance of thorough rinsing after cleaning will help patients avoid toxicity issues. In addition, patients should be cautioned about using too much zinc-containing dental adhesive, as adverse events have been reported.
Breakage. Instructing the patient about proper denture cleaning technique can help minimize problems with broken dentures. Placing water or a towel in the sink will act as a cushion if the prosthesis is dropped, as it may become slippery during the cleaning process.
Inhalation Pneumonia. Linuma et al34 conducted an investigation with 524 subjects who wore their dentures while sleeping. The study revealed these patients contracted inhalation pneumonia at a rate two times the norm.
Chronic Obstructive Pulmonary Disease (COPD). Patients who do not exhibit good denture oral hygiene are at increased risk for COPD. In addition, the same was noted with patients presenting with nicotine stomatitis.35
Conclusion
Caring for a dental prosthesis is an ongoing process for the patient and oral healthcare team. Educating the patient about proper maintenance protocols related to the prosthesis and attachments will support the health of the oral tissues, as well as appliance longevity.
Considering that Locators are the most common attachment used when designing an implant-retained denture, clinicians should provide information specific to this type of device to help patients maintain oral health and maximize the service life of the prosthesis. Implant-supported, fixed full-arch prostheses need not be removed unless the patient presents with just cause. If a patient presents with candidiasis, a full medical history should be reviewed and treatment customized in a manner that treats not only the oral tissues, but the prothesis as well.
Ultimately, ensuring oral health and long-term prosthesis function requires a team effort that includes the dentist, dental hygienist, and an educated patient.
References
- Felton D, Cooper L, Duqum I, et al. Evidence‐based guidelines for the care and maintenance of complete dentures: A publication of the American College of ProsthodontistsJ J Prosthodont. 2011;20(Suppl 1):S1–S12.
- Douglass CW, Shih A, Ostry L. Will there be a need for complete dentures in the United States in 2020? J Prosthet Dent. 2002;87:5–8.
- Felton D. Edentulism and comorbid factors. J Prosthodont. 2009;18:88–96.
- Da Silva F, Kimpara E, Mancini M, et al. Effectiveness of six different disinfectants on removing five microbial species and effects on the topographic characteristics of acrylic resin. J Prosthodont. 2008;17:627–633.
- Sheen SR, Harrison A. Assessment of plaque prevention on dentures using an experimental cleanser. J Prosthet Dent. 2000;84:594–601.
- Ribeiro DG, Pavarina AC, Dovigo LN, Spolidorio DMP, Giampaolo ET, Vergani CE. Denture disinfection by microwave irradiation: a randomized clinical study. J Dent. 2009;37:666–672.
- Panzeri H, Lara EHG, Paranhos HFO, et al. In vitro and clinical evaluation of specific dentifrices for complete denture hygiene. Gerodontology. 2009;26:26–33.
- Zarb GA, Hobkirk J, Eckert S, Jacob R. Prosthodontic Treatment for Edentulous Patients: Complete Dentures and Implant-supported Prostheses. St. Louis: Elsevier Mosby; 2013.
- Ayyıldız S, Sahin C, Emir F, Ersu B. Effect of denture cleansing solutions on the retention of locator attachments over time. J Prosthodont. 2020;29:237–242.
- Nguyen CT, Masri R, Driscoll CF, Romberg E. The effect of denture cleansing solutions on the retention of pink locator attachments: an in vitro study. J Prosthodont. 2010:19:226–230.
- You W, Masri R, Romberg E, Driscoll CF, You T. The effect of denture cleansing solutions on the retention of pink locator attachments after multiple pulls: An in vitro study. J Prosthodont. 2011;20:464–469.
- Kürkcüoğlu I, Ozkir SE, Koroglu A, Sahin O, Yilmaz B. Effect of denture cleansing solutions on different retentive attachments. J Prosthet Dent. 2016;115:606–610.
- Chiu LPY, Di Vitale N, Petridis H, McDonald A. The effect of different water temperatures on retention loss and material degradation of locator attachments. J Prosthodont. 2017;26:537–544.
- Felipucci DNB, Curylofo PA, Crizostomo LC, et al. Effect of cleanser solutions on the retention force of O’ring attachment: An in vitro study. Braz Dent J. 2020;31:657–663.
- Derafshi R, Mohaghegh M, Saki M, Safari A, Haghighi MR. The effects of denture cleansing solutions on the detention of attachments of implant supported overdentures. J Dent (Shiraz). 2015;16(Suppl 1):68–72.
- Varghese RMF, Masri R, Driscoll CF, Romberg E. The effect of denture cleansing solutions on the retention of yellow Hader clips: an in vitro study. J Prosthodont. 2007;16:165–171.
- Armitage G, Pinelopi X. Post‐treatment supportive care for the natural dentition and dental implants. Periodontol 2000. 2016;71:164–184.
- Caton JG, Armitage G, Berglundh T, et al. A new classification scheme for periodontal and peri-implant diseases and conditions — Introduction and key changes from the 1999 classification. J Clin Periodontol. 2018;45(Suppl 20):S1–S8.
- Monje A, Aranda L, Diaz KT, et al. Impact of maintenance therapy for the prevention of peri-implant diseases: a systematic review and meta-analysis. J Dent Res. 2016;95:372–379.
- Bidra AS, Daubert DM, Garcia LT, et al. Clinical practice guidelines for recall and maintenance of patients with tooth-borne and implant-borne dental restorations. J Am Dent Assoc. 2016;147:67–74.
- Sharma N, Shukla J, Sharma D, Mehta D, Kakde L, Bais K. Perceived status and care practices among complete denture wearers. J Pharm Bioallied Sci. 2020;12(Suppl 1):S336–S339.
- Jaiswal AK, Pachava S, Sanikommu S, Rawlani SS, Pydi S, Ghanta B. Dental pain and self-care: a cross-sectional study of people with low socio-economic status residing in rural India. Int Dent J. 2015;65:256–260.
- Bommireddy VS, Koka KM, Pachava S, Sanikommu S, Ravoori S, Chandu VC. Dental service utilization: patterns and barriers among rural elderly in Guntur district, Andhra Pradesh. J Clin Diagn Res. 2016;10:ZC43–ZC47.
- Cinquanta L, Varoni EM, Barbieri C, Sardella A. Patient attitude and habits regarding removable denture home hygiene and correlation with prosthesis cleanliness: A cross-sectional study of elderly Italians. J Prosthet Dent. 2021;125:772.e1–772.e7.
- Shay K. Denture hygiene: a review and update. J Contemp Dent Pract. 2000;1:28–41.
- Harikrishnan R, Ganapathy D, Ramanathan V. A survey on assessing the denture hygiene awareness among elderly patients. Drug Invent Today. 2019;12:2356–2360.
- Peracini A, de Andrade IM, Paranhos HFO, da Silva CHL, de Souza RF. Behaviors and hygiene habits of complete denture wearers. Braz Dent J. 2010;21:247–252.
- Riani E, Octarina O. The effect of mouthwash containing alcohol on flexural strength of polymethylmethacrylate and thermoplastic nylon. J Indo Dent Assoc. 2020;3:17–23.
- Samaranayake YH, Cheung BPK, Parahitiyawa N, et al. Synergistic activity of lysozyme and antifungal agents against Candida albicans biofilms on denture acrylic surfaces. Arch Oral Biol. 2009;54:115–126.
- Wiatrak K, Morawiec T, RóJ R, et al. Evaluation of effectiveness of a toothpaste containing tea tree oil and ethanolic extract of propolis on the improvement of oral health in patients using removable partial dentures. Molecules. 2021;26:4071.
- U.S. Centers for Disease Control and Prevention. Candida infections of the mouth, throat, and esophagus. Available at: cdc.gov/fungal/diseases/candidiasis/thrush/index.html. Accessed April 22, 2022.
- Frazer C, Frazer R, Byron R. Prevent infections with good denture care. Nursing. 2009;39:50–53.
- Saito T, Wada T, Kubo K, Ueda T, Sakurai K. Effect of mechanical and chemical cleaning on surface roughness of silicone soft relining material. J Prosthodont Res. 2020;64:373–379.
- Linuma T, Arai Y, Abe T, et al. Denture wearing during sleep doubles the risk of pneumonia in the very elderly. J Den Res. 2015;94(Suppl 3):28S–36S.
- Przybyłowska D, Rubinsztajn R, Chazan R, Swoboda-Kopeć E, Kostrzewa-Janicka J, Mierzwińska-Nastalska E. The prevalence of oral inflammation among denture wearing patients with chronic obstructive pulmonary disease. Adv Exp Med Biol. 2015;858:87–91.
From Dimensions of Dental Hygiene. May 2022;20(5):36-39.
