Strategies for the Safe Use of CBCT
Cone-beam computed tomography is an effective tool in orthodontics, but it must be used judiciously to protect patients from unnecessary radiation exposure.
Cone-beam computed tomography (CBCT) provides the ability to capture images of three-dimensional dental and skeletal relationships, which is especially helpful in the practice of orthodontics. The use of CBCT, however, increases patient exposure to radiation when compared to traditional radiography. As such, CBCT should be used judiciously to protect patients from undue exposure.
As with all radiographic procedures in dentistry, the need for CBCT should be determined after a review of the patient’s health, availability of previous radiographs, and the completion of a thorough clinical examination. Current recommendations from the American Dental Association (ADA) Council on Scientific Affairs state that CBCT imaging should be performed, “Only when the dental practitioner expects that the diagnostic yield will benefit patient care, enhance patient safety, or improve clinical outcomes significantly.”1 The ADA Council also asserts that CBCT is an adjunct to traditional dental radiography.1 Regarding the appropriateness of CBCT imaging in orthodontics, the ADA Council asserts, “Dentists should use professional judgment in the prescription and performance of CBCT examinations by consulting recommendations from available CBCT guidelines and by considering the specific clinical situation and needs of the individual patient.”1
CLINICAL GUIDELINES
The American Academy of Oral and Maxillofacial Radiology (AAOMR) recently summarized the potential benefits and risks of maxillofacial CBCT use in orthodontic diagnosis, treatment, and outcomes.2 The organization provided clinical guidelines developed by a panel of board-certified orthodontists and oral and maxillofacial radiologists based on analysis of the available published evidence. Specific recommendations are grouped under four general principles.
1. Image appropriately according to clinical condition
Appropriate CBCT imaging should include patient-centered considerations, such as history, clinical examination, and presenting clinical condition. To assist clinicians with their decision making, specific imaging selection guidelines based on the stage of treatment on initial presentation, potential treatment complexity, and the presence of modifying factors have been proposed.2 For various clinical scenarios, an index of the strength of the current available evidence and recommendations on the most appropriate field of view are provided in Figure 1.
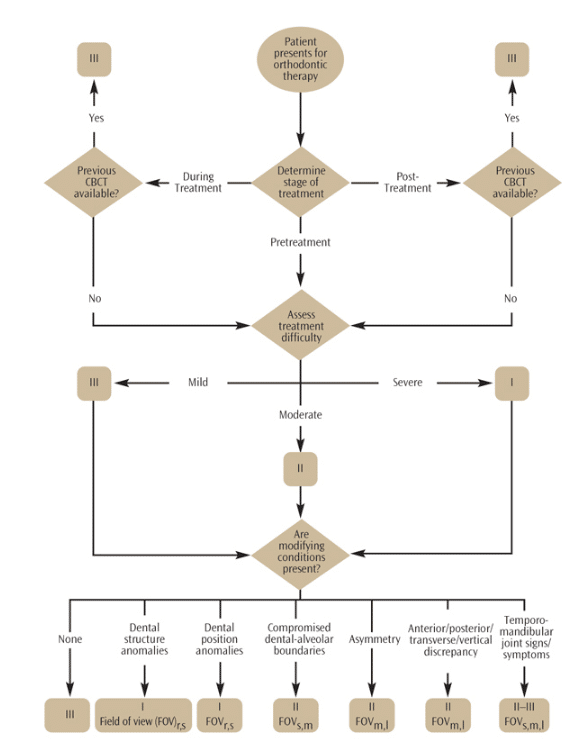
FIGURE 1. The recommendations for appropriate selection of cone-beam computed tomography (CBCT) imaging in orthodontics suggest that determining the phase of treatment is the first decision to be made.2 If the patient is currently undergoing treatment or is post-treatment and a previous CBCT scan is available, taking another is not indicated (III). If unavailable, the potential treatment difficulty should be determined. Mild difficulty includes patients with dental malocclusions, with or without minimal anterior-posterior, vertical, or transverse skeletal discrepancies. For these patients, CBCT is likely not indicated (III). Moderate difficulty includes patients with dental and skeletal discrepancies who are treated orthodontically and/or orthopedically, including bimaxillary proclination, open bite, and compensated Class III malocclusion. For these patients, CBCT may be indicated in certain circumstances (II). Patients with severe treatment difficulties, such as skeletal discrepancies, craniofacial anomalies (eg, cleft lip and palate, craniofacial synostosis), sleep apnea, speech disorders, and post-surgical/trauma, CBCT is indicated (I). Finally, CBCT of various fields of view are most likely (I) or possibly indicated in certain circumstances (II) with the presence of additional skeletal and dental conditions.
The AAOMR document provides a number of common-sense recommendations for the use of CBCT in orthodontics. First, CBCT should be considered only when lower-dose conventional dental radiography—such as panoramic, intraoral, or cephalometric imaging or alternate nonionizing imaging modalities—cannot provide the necessary information to answer a specific clinical question. For example, when orthodontic therapy on a submerged/impacted tooth produces no movement and ankylosis is suspected, small field-of-view, high resolution (<0.2 mm nominal voxel size) CBCT imaging is indicated to identify the periodontal ligament space. No other modality is able to provide an accurate representation of ankylosis.
Second, the use of CBCT should be avoided as the sole method of creating virtual models of the dentition when nonradiographic imaging methods are available. CBCT can practically be used as a virtual impression material to assist in the placement of orthodontic appliances, including aligners, brackets, or custom arch wires. Such techniques, however, are often performed at higher resolutions and at a greater exposure, with an increased radiation dose to the patient than would otherwise be necessary for a diagnostic scan.3
Finally, CBCT exposures should be task specific and tailored to the patient’s unique circumstances. This may include adjustments in exposure (mA and kVp), image-quality parameters (such as the number of basis images or resolution), and reduction of the field of view to adequately visualize the region of interest.
2. Assess the radiation dose risk
Dental practitioners should be knowledgeable about radiation risks when performing CBCT imaging in orthodontics, and they must communicate this information to their patients or guardians prior to treatment. Currently, this risk is calculated by the effective dose (described in Part 1 of this series).4 This is particularly important when treating children, whose risk is three times to five times higher than adults for the same CBCT procedure. A child’s risk compared to an adult’s depends on his or her age. The AAOMR panel suggests the use of relative radiation risk (RRL), developed by the American College of Radiology,5 as useful for assessment of orthodontic radiation dose risk. Practitioners should also be mindful that a course of orthodontic therapy often incorporates multiple radiographic examinations (eg, pre-, peri-, and post-treatment imaging). Every effort should be made to reduce the effective radiation dose to the patient, not only for a single exposure, but also for the cumulative dose over time.
3. Minimize patient radiation exposure
Numerous methods are available to reduce radiation exposure when CBCT imaging is used. The most simple is to reduce the field of view of the CBCT unit to cover a specific region of interest by collimating the X-ray beam, which limits the area of exposure. Exposure settings, number of basis projection images, and resolution—depending on the equipment type and operator preferences—can also be adjusted to reduce exposure. The patient radiation dose for an equivalent field-of-view examination, however, can vary between CBCT units by as much as 10-fold. Avoiding regions that are most sensitive to radiation (eyes and thyroid glands) can also reduce patient risk. The use of patient protective shielding, such as lead torso aprons and thyroid shields,6,7 is recommended to minimize exposure to radiosensitive organs outside the field of view. The Image Gently® in Dentistry campaign, launched in September 2014, is an education and awareness initiative focusing on radiation safety in pediatric maxillofacial radiology. The goal of this campaign is to raise awareness of the special considerations needed for pediatric dental radiology and to promote radiation safety by providing a six-step plan of considerations to standardize clinical workflow and encourage team responsibility. More information is available at: imagegently.org/Procedures/Dental.aspx.
4. Maintain professional competency in performing and interpreting CBCT studies
Any radiographic procedure, including CBCT, may reveal information important to patients’ general health. Incidental findings in CBCT images of orthodontic patients are common,8,9 and some may be critical to their health.2 Clinicians who order or perform CBCT for orthodontic patients are responsible for interpreting the entire image.1,2,10 Qualified specialists, such as oral and maxillofacial radiologists, should be consulted when practitioners are unable to review the whole exposed tissue volume.10 Clinicians should become familiar with the technical and operational aspects of CBCT and maintain current knowledge of scientific advances and health risks associated with its use.
SUMMARY
The introduction of CBCT into the field of orthodontics has advanced the ability of clinicians to treat a variety of challenging conditions—from developmental anomalies to malocclusion and skeletal discrepancies. Its use, however, is not without risk. While it is the practitioner’s responsibility—in collaboration with the patient and his or her family—to decide what imaging is in the patient’s best interest, evidence-based clinical guidelines are available to support the decision-making process. Specific recommendations provide selection guidance based on variables such as phase of treatment, clinically assessed treatment difficulty, presence of dental and/or skeletal modifying conditions, and pathology. These guidelines should be followed in order to ensure the safe use of CBCT among all patients.
ACKNOWLEDGMENT
Some of this information was provided with permission from the American College of Radiology (ACR) and taken from the ACR Appropriateness Criteria®. The ACR is not responsible for any deviations from the original ACR Appropriateness Criteria content.
REFERENCES
- American Dental Association Council on Scientific Affairs. The use of cone-beam tomography in dentistry. An advisory statement from the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2012;143:899–902.
- American Academy of Oral and Maxillofacial Radiology. Clinical recommendations regarding use of cone beam computed tomography in orthodontics. [corrected]. Position statement by the American Academy of Oral and Maxillofacial Radiology. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116:238–257. Erratum in: Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116:661.
- Grünheid T, Kolbeck Schieck JR, Pliska BT, Ahmad M, Larson BE. Dosimetry of a cone-beam computed tomography machine compared with a digital X-ray machine in orthodontic imaging. Am J Orthod Dentofacial Orthop. 2012;141:436–443.
- Scarfe WC, Pinheiro LR, Farman AG. CBCT imaging in orthodontics. Dimensions of Dental Hygiene. 2014;11(4):60–64.
- American College of Radiology. ACR appropriateness criteria®. Radiation dose assessment introduction. 2013. Available at: acr.org/~/media/ a27a29133302408bb86888eafd460a1f.pdf. Accessed January 7, 2015.
- Tsiklakis K, Donta C, Gavala S, Karayianni K, Kamenopoulou V, Hourdakis CJ. Dose reduction in maxillofacial imaging using low dose cone beam CT. Eur J Radiol. 2005;56:413–417.
- Qu XM, Li G, Sanderink GC, Zhang ZY, Ma XC. Dose reduction of cone beam CT scanning for the entire oral and maxillofacial regions with thyroid collars. Dentomaxillofac Radiol. 2012;41:373–378.
- Cha, JY, Mah J, Sinclair P. Incidental findings in the maxillofacial area with 3 dimensional cone beam imaging. Am J Orthod Dentofacial Orthop. 2007;132:7–14.
- Pliska B, DeRocher M, Larson BE. Incidence of significant findings on CBCT scans of an orthodontic patient population.Northwest Dent. 2011;90:12–16.
- Carter L, Farman AG, Geist J, et al. American Academy of Oral and Maxillofacial Radiology executive opinion statement on performing and interpreting diagnostic cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:561–562.
From Dimensions of Dental Hygiene. February 2015;13(2):20–22.

{kind=link}