Solving the Mystery
Radiography provides valuable clues to the correct diagnosis in this case study.
COURTESY OF CHI TRAN, DDS
Many people enjoy the board game Clue, and the process of ruling out suspects and analyzing clues is applicable to dental diagnosis and treatment planning. The circumstances of this case study will be provided with the hope that clinicians will be able to determine the culprit, or diagnosis at the end.
CASE STUDY
A long-time patient of the faculty dental practice at the Dugoni School of Dentistry, University of the Pacific in San Francisco is now in his eighties. His medical history is significant for atrial fibrillation and a small stroke that occurred 6 years ago. The patient takes aspirin, warfarin (blood thinner), lovastatin (statin), and clopidogrel (blood thinner) daily. On the upper arch, he is fully dentate. On the lower arch, the patient is missing six anterior teeth—#22 to #27—and he wears an anterior replacement removable partial denture. For the past 5 years, the patient has been on a 3-month periodontal recare interval for the treatment of moderate periodontitis. The patient has shown significant improvement in oral hygiene, as he is very motivated to prevent further tooth loss.
The patient complains of dry mouth. A drug database search of the patient’s medications reveals that only lovastatin is associated with xerostomia, and the prevalence of this side effect is less than 1%. Warfarin use can contribute to mouth ulcerations, as well as taste variations, and clopidogrel can cause taste disorders in fewer than 1% of patients. As such, the patient’s xerostomia is most likely due to his age as opposed to medication use.

COURTESY OF CHI TRAN, DDS
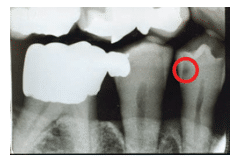
At his last recare appointment, the dental hygienist took bitewing radiographs. The last time the patient had a series of X-rays taken was 1 year prior. Since that time, the office had converted to digital radiography. All prior X-rays had been captured with film. A small radiolucency was noted on the distal aspect of tooth #28 (Figure 1). It was compared to the prior film image of the same area, and it was determined that the lesion appeared smaller 1 year ago (Figure 2). A clinical exam of the distal interproximal area of #28 did not reveal any roughness or softness of the enamel surface. The occlusal aspect of the tooth, specifically the distal pit, was not affected.
The dentist’s examination of the interproximal area did not reveal a portal of entry on #28 for distal caries, and assessment of the radiograph was consistent with this finding. After the patient was questioned about his sugar intake, he revealed that he had a longstanding habit of sucking on cough drops before sleeping to relieve the dryness in his mouth and throat. A repeat examination of all tooth surfaces did not reveal any additional information. The rest of the exam was noncontributory, and the patient was dismissed.
WHAT WAS THAT RADIOLUCENCY?
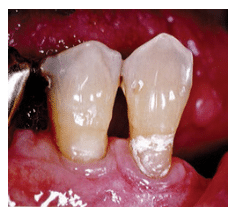
The dental hygienist, realizing that this patient was at increased risk for caries, wanted to be thorough in her assessment. The radiographic finding was documented for follow-up at the next dental appointment. The patient returned for his 3-month periodontal recare appointment. After reviewing the medical history and finding no changes, the dental hygienist reclined the dental chair and adjusted the overhead light. This time, a shiny spot on the buccal aspect of #28 caught her attention (Figure 3). She looked closely at what appeared to be a perfectly round, hard depression in the enamel but was puzzled by its etiology. The shape could only be man-made because it was so uniform. Determined to find the cause of the spot, the dental hygienist considered the patient’s removable partial denture. She reseated the partial denture in the patient’s mouth. The round spot fit perfectly beneath the tip of the metal clasp of the partial (Figure 4).
COURTESY OF CHI TRAN, DDS
DISCUSSION
Teeth that serve as abutments for removable partial dentures exhibit a variety of contours. Some teeth are round, and their height of contour is high on the enamel. Areas with a negative contour can be used to gain retention for a metal clasp arm. Tran et al1 identifies this area as “infrabulge,” meaning any part of the tooth below the height of contour. When these hard tissue undercuts are on root surfaces instead of enamel or they are extremely close to the soft tissue, problems arise with tissue impingement, plaque accumulation, and caries prevention. When natural teeth have unfavorable contours due to the design of the metal clasp arm, the restorative dentist may use a bur to create a more self-cleansing undercut on enamel surfaces. Post-operative radiographs may demonstrate a slight radiolucent area suggesting proximal caries, but the radiographic shadow is created by the depression preparation. The round dimple on tooth #28 exactly corresponded to the tip of the clasp arm of the partial denture, as shown in Figure 4. This provides an explanation for the radiolucent area in the bitewing radiograph. This finding emphasizes the importance of radiography in the documentation of a patient’s clinical status and the need for clinicians to consider a multitude of factors when looking for answers to clinical questions.

COURTESY OF CHI TRAN, DDS
References
- Tran C, LaBarre E, Landesman H. A removable partial denture using an esthetically designed round-rest distal clasp on maxillary anterior abutment teeth: A clinical report. J Prosthet Dent. 2009;102:286–289.
From Dimensions of Dental Hygiene. December 2015;13(12):16–17.

{kind=link}