
Revisiting Instrumentation in Anterior Segments
Selecting and implementing the appropriate instruments for the anterior region of the mouth are key to keeping this area healthy.
Instrumenting anterior segments of the mouth can be challenging. Prophylaxis, nonsurgical periodontal therapy and/or periodontal maintenance are all needed in anterior regions because of deposit accumulation. This can be caused by malocclusion, oral habits, self-care challenges, mandibular salivary duct location, and tooth anatomy. Practitioners know that heavy deposits frequently accumulate in the mandibular anterior region. However, deep deposits can also be present on the maxillary anteriors. Concentrating on efficacious subgingival debridement in addition to instrumenting supragingival deposits is critical for patient health. Appropriate instrument selection for subgingival deposit removal is essential to effectively promote healing.
Root Anatomy
 Practitioners may find that mentally visualizing developmental depressions and grooves, root width, cementoenamel junction (CEJ) curvature, and contact areas helps in performing quality instrumentation. Instrumenting developmental depressions can be tricky. When instrumenting them, practitioners need to remember:
Practitioners may find that mentally visualizing developmental depressions and grooves, root width, cementoenamel junction (CEJ) curvature, and contact areas helps in performing quality instrumentation. Instrumenting developmental depressions can be tricky. When instrumenting them, practitioners need to remember:
- They are more pronounced in the mandibular incisors and canines when compared to the maxillary teeth.
- The distal root concavity on maxillary lateral incisors is significant.
- The mandibular incisors and canines also have proximal concavities.
The mandibular incisors might have a concavity that runs the entire length of the root surface with a groove at the base. Occasionally, a bifuraction exists in the apical one-sixth. The mesial depression on the mandibular canine is more pronounced and deeper than the distal surface. Generally, developmental depressions are .5 mm to 1 mm. Therefore, adapting the instrument into the depth of the depression is important. If depressions are not felt in these areas, then deposit may be present within the depression.
 Narrow and deep developmental grooves are located within proximal depressions. Another notable location for grooves is the maxillary incisors along the palatogingival groove. Palatal grooves are found in 5.6% of maxillary lateral incisors and 3.4% of maxillary central incisors. Approximately half of these have some degree of associated root defect.1 The palatogingival groove is a contributing factor in initiation or progression of periodontitis because it attracts deposit accumulation and is difficult to access so the tooth is compromised.1
Narrow and deep developmental grooves are located within proximal depressions. Another notable location for grooves is the maxillary incisors along the palatogingival groove. Palatal grooves are found in 5.6% of maxillary lateral incisors and 3.4% of maxillary central incisors. Approximately half of these have some degree of associated root defect.1 The palatogingival groove is a contributing factor in initiation or progression of periodontitis because it attracts deposit accumulation and is difficult to access so the tooth is compromised.1
The root in the labio/lingual dimension is related to the length of the instrument’s working end. On maxillary teeth, the labiolingual diameter at and just below the cervix is between 5 mm and 8 mm. The canine is the widest at 7 mm to 8 mm and the lateral is the narrowest at 5 mm to 6 mm. On the mandible, the width in the labiolingual dimension is from 6 mm to 7.5 mm. As the root tapers and narrows subgingivally, a shorter working end—such as a mini-bladed area-specific curet—is appropriate for instrumentation, whereas a mini-bladed curet might not be effective at the midline of wider anterior teeth.
Curvature of the CEJ is a factor to consider when evaluating the endpoint of instrumentation. The curvature on maxillary teeth on mesial surfaces ranges from 2.5 mm to 3.5 mm and from 1.5 mm to 2.5 mm on the distal surfaces. For the mandible, mesial curvature is 2.5 mm to 3 mm and distal curvature is 1 mm to 2 mm. This information helps the practitioner determine deposit from anatomy. Realistically, only 30% of the CEJ will feel smooth and flat because the cementum overlaps enamel in 60% to 65% of teeth and the dentin is exposed 5% to 10% of the time.2
 Practitioners may find that visualizing the proximal anatomy in order to compare tactile sensations with the expected location of the contacts is helpful. Contact areas are located in the incisal or middle one-third. If instrument vibrations are felt in the lower to middle one-third, then perhaps calculus exists. Anterior contacts are about 1.5 mm in length and 1 mm in width. If the contact feels broader than this, then deposit could be present. With age, contact areas become larger and flattened.3
Practitioners may find that visualizing the proximal anatomy in order to compare tactile sensations with the expected location of the contacts is helpful. Contact areas are located in the incisal or middle one-third. If instrument vibrations are felt in the lower to middle one-third, then perhaps calculus exists. Anterior contacts are about 1.5 mm in length and 1 mm in width. If the contact feels broader than this, then deposit could be present. With age, contact areas become larger and flattened.3
Instrument Selection
An explorer shaped like an area specific curet is an ideal choice for shallow and deep pockets. An extended shank 11/12 explorer is appropriate for pockets 5 mm and deeper. Also, a curved explorer shaped like a universal curet is effective. Practitioners might also use a pocket feeler or right-angled design that is straight and narrow with a short 2 mm working end, particularly when deep pockets exist. However, the short working end limits its effectiveness. The 3A explorer is another choice specifically designed for deep pockets (5 mm or greater).
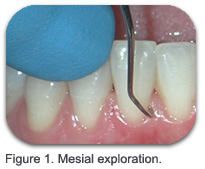
 Exploring effectively is essential in the anterior segments with narrow surfaces, variable contact locations and lengths, anatomical depressions, and variable deposit accumulation. As with exploring in any area, reaching the epithelial attachment is paramount to ensuring complete coverage of the root surface. Correlating the normal anatomical features of the tooth with its radiographic appearance on proximal surfaces is important. Short (1 mm to 2 mm) vertical/oblique overlapping strokes are used to reduce the chance of missing a deposit. Horizontal strokes are applied at line angles for areas with erosion, abrasion, or abfractions; restorative margins; and in narrow pockets and on facials or linguals. One approach for basic exploring is to divide the anterior teeth into three segments: 1) mesial, 2) distal, and 3) facial/ lingual to explore, using overlapping strokes at line angles (see Figures 1-3).
Exploring effectively is essential in the anterior segments with narrow surfaces, variable contact locations and lengths, anatomical depressions, and variable deposit accumulation. As with exploring in any area, reaching the epithelial attachment is paramount to ensuring complete coverage of the root surface. Correlating the normal anatomical features of the tooth with its radiographic appearance on proximal surfaces is important. Short (1 mm to 2 mm) vertical/oblique overlapping strokes are used to reduce the chance of missing a deposit. Horizontal strokes are applied at line angles for areas with erosion, abrasion, or abfractions; restorative margins; and in narrow pockets and on facials or linguals. One approach for basic exploring is to divide the anterior teeth into three segments: 1) mesial, 2) distal, and 3) facial/ lingual to explore, using overlapping strokes at line angles (see Figures 1-3).
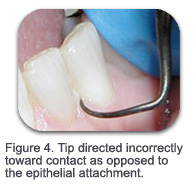
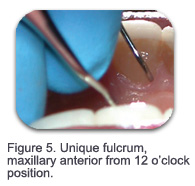
Fulcrum placement is located as close to the working surface as possible. A common error is to direct the tip of the explorer toward the contact (see Figure 4), versus directing it toward the epithelial attachment. This error is easy to correct by standing high on the fulcrum and directing the tip apically at all times. Alternate fulcrums are employed in this region, such as the finger-on-finger for mobile teeth and a unique fulcrum on the maxillary anterior teeth to enhance vision, access, and thoroughness (see Figure 5).
 A file used directly on a tenacious deposit will fracture it so that removal can be completed with curets. The small diameter file is a great instrument for breaking up tenacious deposit in the anterior because of its ability to adapt to flat surfaces such as facials and linguals and proximal surfaces (see Figure 6). Files are also used for burnished calculus and when ultrasonic instrumentation is contraindicated.
A file used directly on a tenacious deposit will fracture it so that removal can be completed with curets. The small diameter file is a great instrument for breaking up tenacious deposit in the anterior because of its ability to adapt to flat surfaces such as facials and linguals and proximal surfaces (see Figure 6). Files are also used for burnished calculus and when ultrasonic instrumentation is contraindicated.
As many practitioners may remember, the sickle is best used supragingivally and subgingivally, where the gingiva permits access. On the other hand, curets adapt to the curved root surface, and the tip is rounded to limit striations and gouging. Comfort is also a factor because the round back, curved blade, and rounded curet toe permit subgingival access in a more comfortable manner when compared to the straighter blades and pointed toe of the sickle. Channeling subgingival deposit with a curet is much more effective and efficient than with a sickle. In fact, using a sickle subgingivally, because of its lack of adaptability, could enhance burnished deposit.
 Curets with straight shanks, particularly the area-specific Gracey 1/2 , 3/4, and 5/6, are commonly used. The shank of the Gracey 1/2 is longer and thinner than the Gracey 3/4. Additionally, the mini-bladed and extended shank versions are appropriate for use with specific areas or conditions. For example, the mini-bladed anterior area-specific curets are ideal for the root developmental depressions and grooves on proximal surfaces. They are also excellent for the direct lingual and facial surfaces, especially in deep pockets (5 mm or greater) due to the short blade length (50% shorter than the traditional design). Extended shank curets may also be used for 5 mm pocket depth or greater because of the 3 mm longer shank length.
Curets with straight shanks, particularly the area-specific Gracey 1/2 , 3/4, and 5/6, are commonly used. The shank of the Gracey 1/2 is longer and thinner than the Gracey 3/4. Additionally, the mini-bladed and extended shank versions are appropriate for use with specific areas or conditions. For example, the mini-bladed anterior area-specific curets are ideal for the root developmental depressions and grooves on proximal surfaces. They are also excellent for the direct lingual and facial surfaces, especially in deep pockets (5 mm or greater) due to the short blade length (50% shorter than the traditional design). Extended shank curets may also be used for 5 mm pocket depth or greater because of the 3 mm longer shank length.
Nagy et al4 evaluated 140 maxillary and mandibular incisors, canines, and premolars for effectiveness of subgingival scaling/root planing with extended shank curets and standard gracey curets with rigid shanks in a timed study. No statistically significant difference was found when the results were measured with a stereomicroscopic evaluation. Calculus was retained less on mesial root surfaces (27%) with the most deposits remaining on the distal surfaces. Remaining calculus was located in root flutes, below CEJs, and on line angles. Mean curet efficiency subgingivally ranged from 1 mm to 3.46 mm.
Diamond-coated instruments can also be used to finish surfaces, using light pressure only, after curet use. They are used for polishing root surfaces, especially during endoscopic evaluation, and are not indicated for heavier deposit removal.
Subgingival or precision thin inserts are effective for biofilm debridement and non-tenacious deposit removal in the anterior segments as well. They are used in addition to the traditional larger ultrasonic inserts that are indicated for heavier and/or tenacious deposit. Many practitioners select the straight shank precision thin insert design for subgingival use, although other slimmer universal designs are used. Always follow-up the use of the ultrasonic insert subgingivally with a curet where needed. Areas under the contact are challenging to totally debride with the ultrasonic as well as proximal depressions and grooves.
Evaluation
Practitioners need to plan how to select and implement different instruments for the anterior region of the mouth. New instruments and sequences can be tried to improve care and to incorporate life long learning into practice. Persistent bleeding and inflammation are not always attributed to self-care. Residual deposit may be the answer because these areas are difficult to access and re-evaluate. If bleeding and inflammation persist, then perhaps calculus is still present and/or self-care is not optimal. The patient needs to be re-revaluated in order to detect subgingival burnished deposit. Endoscopic evaluation of residual calculus is a useful strategy for reevaluation, if available.
References
- Kogon SL. The prevalence, location, and confirmation of palato-radicular grooves in maxillary incisors. J Periodontol. 1986;57:231-234.
- Fiorellini JP, Kim DM, Ishikawa SO. The tooth supporting structures. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA. Carranza’s Clinical Periodontology. 10th ed. St Louis: Saunders; 2006:76.
- Woelfel JB. Dental Anatomy: Its Relevance to Dentistry. 4th ed. Philadelphia: Lea and Febiger; 1990.
- Nagy RJ, Otomo-Corgel J, Stambaugh R. The effectiveness of scaling and root planing with curets designed for deep pockets. J Periodontol. 1992;63:954-959.
From Dimensions of Dental Hygiene. February 2007;5(2): 30, 32-33.

{kind=link}