
Local Anesthesia
Providing effective anesthesia is dependent on understanding the drug, the dosage, and the patient in conjunction with clinical skill.
Delivering local anesthesia and effectively for each patient can be stressful as many important factors must be considered, from pKa values to clinical technique. When considering local anesthetic delivery practices and results, three key factors1contribute tocommon errors: armamentarium-relto commontors (including drug selection and dosage), patient-related factors (anatomical variances in skeletal form and nerve innervations), and clinician related factors (inexperience and poor technique).

Click here to view the a list of the pKa values of anesthetic drugs
ARMAMENTARIUM-RELATED FACTORS
While learning local anesthesia administration in school, many students dread the calculations necessary to convert micrograms to milligrams to ccs. However, the math is important so the correct amount of anesthetic will be safely delivered. Understanding the limiting factors for determining the maximum number of cartridges and pKa values are two key factors in ensuring that the maximum safe dosage of anesthetic is not exceeded.
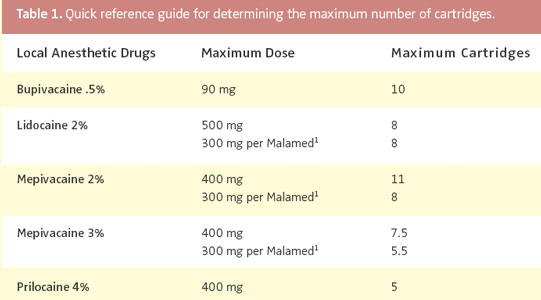
When using local anesthetic agents containing a vasoconstrictor concentration of 1:100,000 or 1:200,000, remember that the vasoconstrictor typically is NOT the limiting factor for determining the maximum number of cartridges that should be safely delivered. The limiting factor is the local anesthetic drug itself. Table 1 provides a quick referenceguide that can be kept close at hand in the operatory.
Situations do occur where these maximums are still too much drug for the patient. The maximum safe doses published in drug information inserts are based on a healthy 150 lb man and even these doses are considered too high by some researchers.2
When delivering local anesthetic agents to smaller people (such as children and small adults weighing less than 150 lbs), decrease the amount of drug given accordingly. For patients weighing more than 150 lbs, no modification is indicated. The maximum dose of 400 mg will be the same for a 200 lb person, but it is 266 mg for a 100 lb person. Keep in mind that modifications may be required for medically compromised patients—the recommended safe dosage is reduced to 1/5th of the total given for a healthy patient.
|
|
|


In literal terms, pKa is the logarithmic expression of an acid dissociation constant, in other words, the drug’s readiness to give up or accept hydrogen ions. P is the negative log of Ka, K is equilibrium constant, and Ka is the equilibrium constant of an acid. The pKa value encompasses two parts: the basic (anion) and acidic (cation). The basic component is responsible for getting the anesthetic through the tissue to the nerve membrane. The acidic component actually blocks the nerve impulse once the drug is delivered at the target area.
The pKa value of anesthetic drugs (see the web version of this article for a list of the pKa values of anesthetic drugs) indicates how quickly the drug will begin to block nerve sensations (onset) and how long the drug is expected to last (duration) without the benefit of a vasoconstrictor. Remember, the closer the pKa value of the local anesthetic is to 7.4 (normal tissue pH), the faster the onset of the drug.
When a drug is more acidic, the pKa value is higher. Therefore, the drug’s onset is slower, resulting in more discomfort for the patient during the injection. A lower pKa indicates just the opposite—quicker onset and less discomfort during injection.
The effect of inflammation in the soft tissues surrounding the injection site is another important factor to consider. When infection is present, the body creates a more acidic environment (pH 5.5). When you inject anesthetic into the area, the basic component of the drug is used up before it can effectively pass through the tissues to block the nerve impulses. Choosing a drug with a lower pKa value may increase drug effectiveness in the presence of inflammation.
PATIENT- AND CLINICIAN-RELATED FACTORS
The greatest error in delivering local anesthetics is the failure to deposit the drug where it is most effective. Injection technique can be modified to find >the most effective locations.
1. Posterior superior alveolar nerve block (PSA). Considering a new perspective for the traditional concept of “up, in, and back”2can result in an easy, successful PSA injection. The key is using external landmarks to guide you. To begin, face the patient from an 8 o’clock position, imagine an “X” across the patient’s face that intersects at the tip of the nose and passes through the pupil of each eye (Figure 1).
|
|

Next, with your index finger palpate the maxillary vestibule to locate the zygomatic strut (near the first molar [Figure 2]), then pivot downward on your finger tip to create a 45° angle to the maxillary occlusal table (Figure 3). This is the “up” (to achieve this your syringe will drop down). Remember the target is upward and inward, behind the maxillary tuberosity, on the back of the maxilla (Figure 4).
Now, with your finger pointing at your down angle, retract the lip outward to a 45° angle to the patient’s midline, lining up with the imaginary “X”bisecting the patient’s face (Figure 5). This is the “in”(to achieve this your syringe will be angled out). You are now “down and out” and can follow this line for insertion (Figure 6). Additionally, you have created a visual pathway with the “X”and a stable finger rest for the syringe barrel during the injection.
The target is up and in, on the backside of the maxilla. Advancing now moves you backward to reach your deposition site, completing the “back” step (Figure 7). Aligning to the “X” and aiming for a visual target between the inner corner of the opposite eye and the pupil aligns you to deposit anesthetic at the backside of the maxilla and the location of the PSA foramina. An easy way to gauge your depth is to visualize a line from the front of the needle hub to the gingival margin or cementoenamel junction (CEJ) of the first or second molar, in most cases this will be equal to 2/3 the length of a short needle. This is especially helpful to confirm that you haven’t withdrawn during aspiration (Figure 8).
|
behind the makillary tuberosity. |
and up as the syringe is advanced. |
 Figure 5.Syringe aligned in the downand out position. From down and out,insert to your target depth. |
 Figure 8. Note the position of theneedle hub at the CEJ. This isyour reference point for depth. |
 Figure 6.Advance along the “X”toward the patient’s opposite pupil. |
 Figure 9. Premature contact. |


The keys to success with this approach are: retracting the lip downward and outward to clear the path of the syringe and creating a visual cue for maintaining an angle that is approximately 45° to the patient’ midline plane and maxillary occlusal table to put you up and behind the maxillary tuberosity, at the site of the PSA foramina.
2. Inferior alveolar nerve block (Mandibular Block, IA.) Making a few adjustments in technique for the IA will improve your odds for success. Discussions about technique for the IA often include the statement “when in doubt, error high.”3 The word “error” infers a bad choice, when, in fact, this approach is a good way to offset the potential for missing the block because you’re below the foramen. Consider a slightly higher penetration site as the norm, not the exception. The most common error for the IA is injecting too low and/or too lateral, which makes adjusting to a higher penetration site a prudent practice.
A common result of penetrating too low is premature contact with bone. This can also be the case when the initial penetration is too lateral and close to the inner (medial) border of the ramus (Figure 9). Both of these situations can occur naturally and when the cheek and soft tissue are retracted too aggressively, actually displacing the pterygomandibular raphae onto the inner border of the ramus. A more gentle retraction of the buccal soft tissues and gently deflecting the raphae with the needle, away from the inner surface of the ramus, at the point of insertion will reduce this (Diagram 1). This technique also may make the raphae more visible.
3. Pediatric considerations.4,5 Following are tips for delivering local anesthetic to pediatric patients:
• When administering maxillary infiltrations for primary dentition, do not assume that the roots are short and, therefore, the deposition site shallower than for an adult. This will result in delivery below the apex of the root.
• Due to the more diffuse bone structure, infiltrations of mandibular primary teeth (including molars) can provide profound anesthesia without the soft tissue trauma implications of a numb lip and tongue. Administering bilateral mandibular blocks for a child may not increase the incident of post-operative lip biting. Current literature4 shows fewer traumas than with a unilateral injection.5
ACKNOWLEDGEMENTS
Thank you to photographer Ron Oyama, illustrator Richard Smith, DDS, and Shirley Chung who provided the digital graphics.
REFERENCES
- Wong JK. Adjuncts to local anesthesia: separating fact from fiction. J Can Dent Assoc. 2001;67:391-397.
- Malamad SF. Techniques of maxillary anesthesia. In:Malamad SF, ed. Handbook of Local Anesthesia. 5thed. St Louis: Elsevier Mosby; 2004:189-224.
- Malamed SF. The renaissance in local anesthesia. Presented at: International Dental Seminars; November 6, 2004; Seattle.
- Pediatric Dental Health. Available at: http://dentalresource.org/topic38anesthesia.htm. Accessed February 15, 2005.
- College C, Feigal R, Wandera A, Strange M. Bilateral versus unilateral mandibular block anesthesia in thepediatric population. Pediatr Dent2000;22:453-457.
From Dimensions of Dental Hygiene. March 2005;3(3):22, 24-25, 27.

{kind=link}