Incorporate Channeling Into Instrumentation
Originally used only during manual debridement, channeling strokes are also helpful in power scaling to increase the efficacy of therapy.
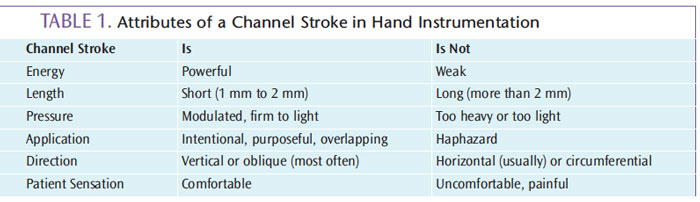
Channel scaling is the removal of deposits through the use of overlapping strokes on the root surface until complete coverage has been provided. Deliberate, powerful, and controlled, channel strokes are an important part of the activation phase of hand instrumentation (Table 1). The practice of channeling originally applied only to hand-activated instrumentation; however, the strategy can be useful for ultrasonic debridement as well.
ULTRASONIC INSTRUMENTATION
During power-driven instrumentation, a pattern of calculus removal should be implemented to prevent leaving fragments behind, missing surfaces, and burnishing deposits. Compared to manual instrumentation, the pressure used in ultrasonic scaling is often lighter. Unlike the use of hand instruments to exert modulated lateral pressure, ultrasonic energy fractures deposits. The very firm lateral pressure applied in manual instrumentation is not necessary with ultrasonic instrumentation.
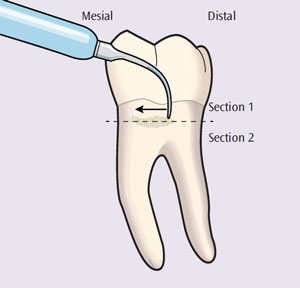
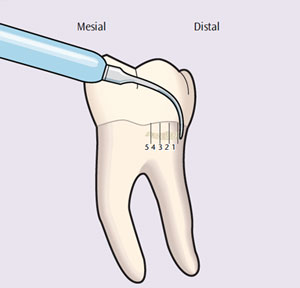
The use of heavy lateral pressure during ultrasonic instrumentation can bind the process of energy transfer, resulting in partial deposit removal or burnishing. If calculus is moderate to heavy and dense, a coronal to apical—or “top down” —approach should be used. The ultrasonic insert/tip (UIT) is adapted on the top of the deposit and tapped in small increments, moving in a crosswise, horizontal pattern (Figure 1). After removal of the most coronal portion (Section 1), the second most coronal portion (Section 2) should be removed in the same manner. However, when the deposit is small and not as dense—and precise, thin UITs are used—a channel-like approach from the epithelial attachment to the gingival margin can be effective for thorough debridement (Figure 2). If circumferential strokes are used with ultrasonic instrumentation, channeling strategies do not apply.
TIMING DURING THERAPY
Calculus should be detected and then evaluated for location, shape, and size. If appropriate for removal with a curet, then the process occurs between assessment (ie, exploratory) strokes and debridement strokes (ie, finishing, final, or root planing). However, if the calculus is heavy and tenacious, then it first needs to be prepared in order for channeling with hand instrumentation to be effective. This preparation, or removal of gross deposit, is accomplished with a periodontal file, such as the Hirschfeld 3/5 and 7/11, and/or a traditional UIT to fracture the deposit. After this process, the deposit is less dense and fragmented, and ready for a curet and channeling. In this case, a universal curet with moderate shank strength would precede area-specific designs to save time, effort, and fatigue from the use of many repetitive strokes that might occur if only area-specific curets with flexible shanks are used. Following is a possible succession of instrumentation for use with the blended approach:
- Periodontal files and standard UITs
- Universal designs to area-specific designs
- Mini-bladed, area-specifics
- Precision, thin inserts (ie, microultrasonics)
![]()
Even if the deposit is small or moderate in size and granular on the exterior, channeling is recommended. A smaller, less dense deposit can be intricately attached to the root at its undermost layers, making it resistant to removal. In this situation, preparation is probably not necessary, and the fundamental principles of instrumentation still apply while channeling strokes are used.
SELF-ASSESSMENT OF HAND INSTRUMENTATION
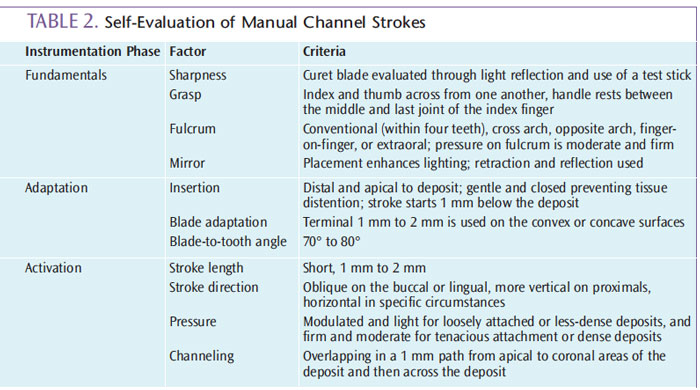
Clinicians who are suffering from hand pain while struggling to remove deposits, and whose patients express discomfort in the dental chair, may need to add channeling to their technique. If a sharp curet blade is being used, then the absence of channeling may be the reason that both the practitioner and the patient are experiencing pain. The self-assessment of working strokes should be ongoing to prevent development of poor habits, evaluate the pressure applied, and assess the clinician’s and patient’s health and stress. Most important, self-assessment leads to efficacious deposit removal, critical thinking, problem solving, and lifelong learning, which are all crucial in clinical practice (Table 2).
CLOSING THOUGHTS
Although patients will not necessarily know that a clinician is channeling, its use translates into comfort, thoroughness, organization, efficiency, minimal post-operative discomfort, and optimum healing. Channeling strokes are typically more comfortable than longer, uncontrolled strokes with heavier pressure. Therapy that is controlled and precise also instills a feeling of safety, as opposed to the use of uncontrolled strokes, which may increase patient stress and fear.
It takes time and experience for clinicians to become skilled in the use of channeling strokes.1 Visualization and concentration during competency development are necessary to acquire exemplary instrumentation skills.2 This dedication to improving instrumentation technique will pay back many dividends in practitioner safety, patient comfort, and, ultimately, successful therapeutic outcomes.
REFERENCES
- Chambers DW, Glassman P. A primer on competency-based evaluation. J Dent Educ. 1997;61:651–666.
- Matsuda S. Anatomy of a stroke. Dimensions of Dental Hygiene. 2008.6(11):22–26.
From Dimensions of Dental Hygiene. July 2013; 11(7): 36–38.

{kind=link}