 ASISEEIT/E+/GETTY IMAGES PLUS
ASISEEIT/E+/GETTY IMAGES PLUS
Health Literacy for the Dental Professional
Assessing and addressing low oral health literacy can help improve patient adherence to recommendations and outcomes.
This course was published in the March 2017 issue and expires March 2020. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define oral health literacy.
- Describe the health implications and financial impact of low oral health literacy.
- Discuss methods for assessing oral health literacy.
- Identify strategies to effectively communicate with patients who have low oral health literacy.
The concept of oral health literacy is similar to health literacy but is specific to oral health as opposed to overall health. The multiple factors that comprise oral health literacy include:
Knowledge About a Specific Disease. For example, the public and medical professionals are often unaware that dental caries is both infectious and preventable.
Interpreting Risk and Benefits of Recommended Treatment. Materials are frequently written at advanced reading levels. Many patients may find interpreting the proportions or ratios required to adequately understand treatment risks difficult.
Performing a Specific Task. Functional oral health literacy refers to the ability to carry out a skill such as making dental appointments, following through with a referral for specialty care, or improving flossing technique.
Cultural Background, Societal Influences, and Familiarity with the Health Care System. Culture strongly influences how people think and feel about oral health. In many developing countries, preventive care is rare and seeking dental services for reasons besides acute pain is uncommon.3 Immigrants often retain similar care-seeking practices upon relocating to the US, and these practices may be passed down to subsequent generations.
Daily demands of living, lack of insurance, and difficulty locating an appropriate provider are also barriers to seeking routine dental services. The complexity of the information presented in addition to dental anxiety may also impact an individual’s ability to comprehend and communicate preferences to dental providers.4,5
Studies show that low oral health literacy is more common among adults with less than a high school education, older adults, immigrants and refugees, racial and ethnic minorities, and low-income individuals.6–8 While oral health literacy has not been studied as extensively as health literacy, oral health literacy alone may be a better predictor of poor oral health outcomes than any other demographic factor.9
Individuals with low oral health literacy are less likely to exhibit oral health-related behaviors including daily toothbrushing and flossing, seeking preventive and restorative dental care, and eating a low cariogenic diet.10–13 Poor oral health outcomes include more severe periodontal disease, advanced caries, tooth loss, and reduced quality of life.4,12,14
ASSESSMENT OF ORAL HEALTH LITERACY
Approximately 20 surveys measure oral health literacy.15 Some are more appropriate for use in research settings than clinical practice. The Test of Functional Health Literacy in Dentistry is appropriate for use in the clinical setting. Patients read a toothpaste label and answer questions reflecting reading ability, comprehension, and numeracy.16 Another assessment method used in patient care consists of four questions that can be administered independently or added to a health history. The questions focus on patients’ confidence in the ability to complete medical forms and read medication labels, as well as any difficulties they may have learning about health topics due to limited reading abilities.17 While most assessments are helpful with measuring reading and numeracy, they may be of limited usefulness when measuring how well patients navigate the health care system or make health care decisions. Researchers continue to develop and test oral health literacy instruments that can be used in clinical practice. As a standard tool or index has not been accepted for routine clinical use to date, alternative strategies—such as conducting informal individual assessments—may be more practical for many clinicians.
An informal method to assess oral health literacy is to observe patients as they fill out forms. Patients who take a long time to read and sign consent forms, look confused, make excuses such as “I forgot my glasses,” or ask for assistance may have trouble reading.18 In a recent study, oral health professionals reported asking unscripted open-ended questions to assess oral health literacy. Through conversation, oral health professionals gained a sense of both patients’ oral health knowledge level and interest in improving their oral health.19
Researchers have found that if clinicians take the time to ask patients to explain exactly what they understand about their conditions and instructions, they would find many gaps in knowledge, difficulties in understanding, and misinterpretations.4 Because of the difficulty in assessing every patient seen in a clinical setting, an approach similar to the universal precautions used for infection control can be effective.20 The assumption that all patients may need some level of assistance to understand oral health information can help dental professionals approach each patient at an appropriate level. This approach does not assume the existing health literacy level of individual patients, but rather creates an environment where patients may feel more comfortable asking questions.20The clinical encounter may routinely include a conversational assessment to find out the patient’s educational level; readiness to learn and learning preferences; and determine any cultural, developmental, and religious considerations that may affect health care.4The communication can then be steered to meet the requirements of evidence-based dentistry, where the most current treatments intersect with the patient’s preferences and the clinician’s expertise.21
ADDRESSING ORAL HEALTH LITERACY
The extent and complexity of the oral health literacy problem requires a comprehensive solution. The American Dental Association proposed a plan that addresses three major areas of intervention to improve patient oral health literacy, and, in turn, improve oral health outcomes.22 The three areas of intervention are at the broad levels of culture and society, educational system, and health care system (Figure 1).22 While dental professionals can implement change in these areas, this article focuses on addressing oral health literacy within health care.

Health care settings can make it easier for patients to access and understand health information. Examples include designing websites that are easy to navigate and presenting information in plain language. Providing an interactive map on the practice’s website can help patients find the office. In the dental office, directional signage using pictograms aids patients with limited reading ability. Staff can review forms and written materials to ensure they are at the 6th grade reading level. Reception areas should be welcoming and staff should be friendly.9,23
Oral health professionals have a significant role in bridging the gap between what is known about oral health and what the patient actually understands.24 For example, a patient-provider conversation may help the patient identify a therapy or adapt behavior change that improves oral health. Communication can also have a less direct pathway to impact patient health. If communication results in the feeling of validation, reduces fear or anxiety, improves understanding, or provides social support, the patient may be more apt to comply with provider recommendations. Conversely, engaging in controlling communication laced with disagreement and directives may lead to poor adherence to directions.25 Dental professionals need to remember that individuals may have skills but choose not to use them in certain settings.26 In other words, a motivated patient with low oral health literacy may be more receptive to improving his or her oral health behavior compared with a more informed patient who doesn’t value oral health.
Understanding patients’ levels of motivation and communicating this are at the core of moving patients toward behavior change to improve their oral health. Communication practices that include the patient as an active participant rather than the recipient of information can help ensure that patients understand recommendations. Motivational interviewing (MI), which incorporates learning and building on patient priorities, is an effective tool to facilitate behavior change.27 Using MI strategies to establish a patient’s level of engagement and priorities for care can help clinicians determine the most effective communication strategies. Through asking open-ended questions about the patient’s attitudes about oral health, barriers to making a change in self-care, and perceived benefits of making a change, clinicians can use the patient’s attitudes and priorities to meet his or her oral health goals. An open-ended question is one where a response is required rather than a simple “yes” or “no.” For example, clinicians may ask, “Can you tell me about your at-home oral hygiene routine?” or “How important is it for you to keep your teeth?”
The stages of change (or transtheoretical) model is the foundation of MI and provides a framework for determining patients’ readiness for change. Patients who have no desire or intention to make a change are in the precontemplation stage. Those thinking about making a change in the future are in the contemplation stage. Patients getting ready to make a change are in the preparation stage. They are willing to invest the time and effort needed to learn new knowledge and skills. Those in the process of making a change are in the action stage. These patients have exhibited behavior change or initiated the new skill. The maintenance stage occurs after the patient has accomplished the behavior change.28 Studies show that this approach is more effective than standard health education.29
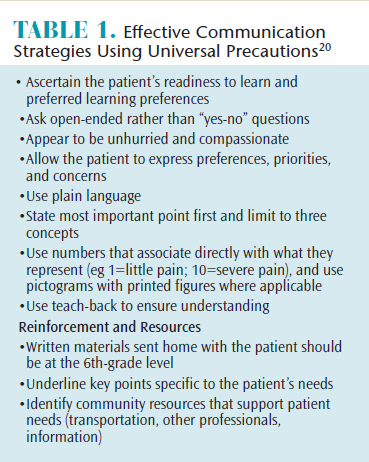
After establishing rapport and using MI to determine if the patient is willing to participate in a discussion about oral health (ie, contemplation or preparation phase), several specific communication strategies are recommended for use with low oral health literacy patients. Each strategy may be used alone or in combination (Table 1).20
The most effective and adaptable strategy is called “teach-back” and confirms understanding by asking the patient to explain information back to the provider (Figure 2). For example, after presenting a recommendation for scaling and root planing, a dental hygienist may say, “I want to make sure that I explained this correctly. Please tell me in your own words how you understand the treatment plan.” If a misunderstanding exists or modification is required, the oral health professional can clarify the explanation. Ensuring both understanding and agreement about the care plan is essential to achieving patient adherence.22 Perhaps most importantly, clinicians have reported that teach-back doesn’t take more time out of their day and is worth the effort to learn a different method of communicating with patients.30

A large study of health literacy interventions reported several other strategies were effective with low health literacy patients.31 These include presenting the most essential information first or by itself and adding video content to verbal descriptions. Written material should include simplified text at the 6th grade reading level. Numerical information is more effective if icons or pictograms were added to number displays.31
The use of plain language is recommended. Plain language was historically referred to as “layman’s terms” and more recently as “simple language.” This means making information easier to understand by using basic terms and breaking complex information into smaller pieces.4 Examples include using the term “cavities” for “caries,” “sticky film with germs on your teeth” for “plaque,” and “hard, crusty deposits” to describe “calculus.”
The demeanor of the clinician is also important. Studies where clinicians provided clear explanations, appeared compassionate, and involved patients in decision-making correlated with lower blood pressure and reduced anxiety.32 Clinicians who used a superior tone or talked down to patients appeared judgmental, negatively affecting outcomes.31,33
Sharing information about available resources in the surrounding area is also helpful for patients with low oral health literacy. Keeping up to date on community resources in order to refer patients to additional services such as transportation options and other health care or social service professionals can support patients with low oral health literacy.
Appointments should conclude with an invitation for patients to ask questions. Rather than posing a yes or no question, an open-ended question, such as, “What questions do you have for me?” will be more effective. Clinicians should discern whether a follow-up phone call or text may be helpful and ask permission to check in at certain intervals. When patients feel their providers care about them, a stronger patient-provider relationship is forged.25,34
CONCLUSION
In summary, a large proportion of Americans have low oral health literacy and may struggle to make oral health decisions. Clinicians who are prepared with tools, such as MI, will be best able to assist their patients improve their oral health. Determining whether patients are willing to listen, learn, and change behaviors to enhance their oral health is important. Using communication strategies shown to be helpful for patients with low oral health literacy can help encourage patients toward better health outcomes.
REFERENCES
- Kutner M, Greenberg E, Jin Y, Paulson C. The Health Literacy of America’s Adults: Results From the 2003 National Assessment of Adult Literacy. Washington, DC: US Department of Education; 2006.
- Institute of Medicine Committee on Health Literacy. Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press; 2004.
- Vered Y, Zini A, Livny A, Mann J, Sgan-Cohen HD. Changing dental caries and periodontal disease patterns among a cohort of Ethiopian immigrants to Israel: 1999–2005. BMC Public Health. 2008;8:345.
- New York State Department of Health, Oral Health Division. Oral Health Literacy Toolkit: 2015. Available at: static1.squarespace.com/ static/53bc58e3e4b060a82ab 7359d/t/552d2c18e4b057e7ac6e3e3e/1429023768340/Oral+Health+Literacy+Toolkit.pdf. Accessed February 9, 2017.
- Allison P, Locker D, Jokovic A, Slade G. A cross-cultural study of oral health values. J Dent Res. 1999;78:643–649.
- Jones M, Lee JY, Rozier RG, Bender D, Ruiz RE. Oral health literacy among adult patients seeking care. J Am Dent Assoc. 2007;138:1199–208.
- McQuistan M, Qasim A, Shao C, Straub-Morarend C, Macek M. Oral health knowledge among elderly patients. J Am Dent Assoc. 2015;146:17–26.
- Maserejian NN, Trachtenberg F, Hayes C, Tavares M. Oral health disparities in children of immigrants: dental caries experience at enrollment and during follow-up in the New England Children’s Amalgam Trial. J Public Health Dent. 2008;68:14–21.
- Podschun G. National plan to improve health literacy in dentistry. J Calif Dent Assoc. 2012;40:317–320.
- Divaris K, Lee JY, Baker AD, Vann WF. Caregivers’ oral health literacy and their young children’s oral health-related quality-of-life. Acta Odontol Scand. 2012;70:390–397.
- Lee JY, Divaris K, DeWalt DA, et al. Caregivers’ health literacy and gaps in children’s Medicaid enrollment: findings from the Carolina Oral Health Literacy Study. PloS One. 2014;9:e110178.
- Miller E, Lee JY, DeWalt DA, Vann WF Jr. Impact of caregiver literacy on children’s oral health outcomes. Pediatrics. 2010;126:107–114.
- Vann WF Jr, Divaris K, Gizlice Z, Baker AD, Lee JY. Caregivers’ health literacy and their young children’s oral-health-related expenditures. J Dent Res. 2013;92:55S–62S.
- Naik A, John MT, Kohli N, Self KD, Flynn P. Validation of the English language version of the OHIP-5. J Prosthodont Res. 2016;60:85–91.
- Dickson-Swift V, Kenny A, Farmer J, Larkins S. Measuring oral health literacy: a scoping review of existing tools. BMC Oral Health. 2014;14:148.
- Gong DA, Lee JY, Rozier RG, Pahel BT, Richman JA, Vann WF, Jr. Development and testing of the Test of Functional Health Literacy in Dentistry (TOFHLiD). J Public Health Dent. 2007;67:105–112.
- Chew L, Bradley K, Boyko E. Brief questions to identify patients with inadequate health literacy. Family Med. 2004;36:588–594.
- National Institute of Dental and Craniofacial Research.The invisible barrier: literacy and its relationship with oral health. J Public Health Dent. 2005;65:174–182.
- Flynn P, VanWormer J, Schwei K, Skrzypcak K, Acharya A. Assessing dental hygienists’ communication techniques with low oral health literacy patients. J Dent Hyg. 2016;90:162–169.
- DeWalt D, Callahan L, Hawk V, et al. Health Literacy Universal Precautions Toolkit. Rockville, Maryland: The Cecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill, April 2010. Report No: AHRQ Publication No. 10-0046-EF.
- Frantsve-Hawley J, Clarkson J, Slot D. Using the best evidence to enhance dental hygiene decision making. J Dent Hyg. 2015;89:35–38.
- American Dental Association Council on Access Prevention and Interprofessional Relations. Health Literacy in Dentistry Action Plan, 2010-2015. Chicago: American Dental Association; 2009.
- Horowitz AM, Kleinman DV. Creating a health literacy-based practice. J Calif Dent Assoc. 2012;40:341–350.
- Horowitz AM, Clovis JC, Wang MQ, Kleinman DV. Use of recommended communication techniques by Maryland dental hygienists. J Dent Hyg. 2013;87:212–223.
- Street RI, O’Mallley KJ, Cooper LA, Haidet P. Understanding concordance in patient-physician relationships: personal and ethnic dimensions of shared identity. Ann Fam Med. 2008;6:198–205.
- Pleasant A. Advancing health literacy measurement: a pathway to better health and health system performance. J Health Commun. 2014;19:1481–1496.
- Rollnick S, Miller W, Butler C. Motivational Interviewing in Health Care: Helping Patients Change Behavior. New York: Guilford Press; 2007.
- Norcross JC, Krebs PM, Prochaska JO. Stages of change. J Clin Psychol. 2011;67:143–154.
- Stewart J, Wolfe G, Maeder L, Hartz G. Changes in dental knowledge and self-efficacy scores following interventions to change oral hygiene behavior. Patient Educ Couns. 1996;27:269–277.
- DeWalt DA, Broucksou KA, Hawk V, et al. Developing and testing the health literacy universal precautions toolkit. Nurs Outlook. 2011;59:85–94.
- Sheridan SL, Halpern DJ, Viera AJ, Berkman ND, Donahue KE, Crotty K. Interventions for individuals with low health literacy: a systematic review. J Health Commun. 2011;16(Suppl 3):30–54.
- Street R, Makoul G, Arora N, Epstein R. How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ Couns. 2009;74:295–301.
- Samuels-Kalow M, Hardy E, Rhodes K, Mollen C. “Like a dialogue:”: teach-back in the emergency department. Patient Educ Couns. 2016;99:549–554.
- Waldenstrom U. Continuity of carer and satisfaction. Midwifery. 1998;14:207–213.
From Dimensions of Dental Hygiene. March 2017;15(3):46-49.
