 ANRPRODUCTION/ISTOCK/GETTY IMAGES PLUS
ANRPRODUCTION/ISTOCK/GETTY IMAGES PLUS
Hand Instrumentation of First Molar Teeth
Memorizing the anatomy and proper instrument selection are key to successful scaling of this part of the dentition.
Efficacious mechanical debridement is an essential component of care for patients with periodontitis. Generally, the more advanced the periodontitis, the more complex the instrument selection and periodontal instrumentation. One of the first considerations for hand-activated instrumentation for first molar teeth is the suspected anatomy of the root.
MAXILLARY FIRST MOLAR ANATOMY
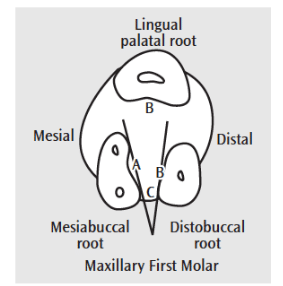
The root morphology of the maxillary first molar includes a concavity leading into the furcation area between the two buccal roots (Figure 1).1 The palatal root is usually convex, however, it could contain shallow concavities. The mesial surface of the maxillary first molar has a concavity leading into the furcation. The distal surface has a broad and shallow surface depression extending coronally to the cementoenamel junction (CEJ) (Figure 2). The buccal and lingual root lengths are about 12 mm and 13 mm, respectively.

It is important to remember how close in proximity maxillary first molar furcation roofs can be to the CEJ. Usually, the buccal furcation roof is located only 4 mm from the CEJ. Likewise, the mesial furcation roof is 3 mm from the CEJ and the distal furcation roof is 5 mm from the CEJ. Therefore, the furcation can be exposed with slight, moderate, or severe (advanced) periodontitis depending on the height of the gingival margin and the amount of recession (Table 1).2 Access to the mesial furcation is best from the lingual surface because the entrance is located lingually and not directly in the midline. The distal furcation entrance, however, is located in the midline and can be approached from either the buccal or lingual surface.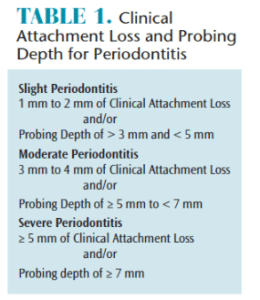
The opening at the roof of the furcation is very narrow, making entrance by a hand-activated instrument challenging. The opening of the buccal furcation is only 0.5 mm wide, the mesial furcation is 0.75 mm and the distal furcation is 0.5 mm to 0.75 mm wide. In fact, the blade face width of universal and area-specific curets is from 0.75 mm to 1.1 mm and area-specific curets are slightly narrower than universal curets. It is also important to review the internal concavities of the first molar furcations, which present an additional challenge for instrumentation if destruction of the periodontium has permitted exposure (Figure 3).
The location of the cervical line or CEJ is of interest when removing deposit from proximal surfaces. This molar has a mesial proximal curvature of 1 mm, and no curvature on the distal surface. This cervical line curvature, or lack thereof, is important for deciphering calculus deposit from root surface anatomy.
Additionally, the width of a molar’s root near its cervix is important. One-half of the width is used to gauge if an instrument’s working end can reach and overlap the midline of the proximal surface. This molar has a bucco-lingual diameter of 11 mm and is the widest tooth in the oral cavity, emphasizing the importance of using an instrument with a working end long enough to overlap at the midline.
MANDIBULAR FIRST MOLAR ANATOMY
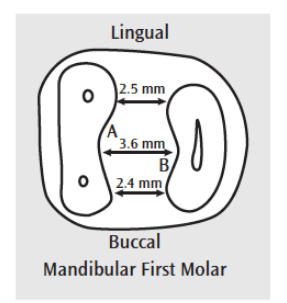
The double-rooted mandibular first molar has a convex root trunk on the buccal and lingual surfaces.1 This buccal and lingual root trunk has a concavity starting about half-way between the CEJ and the furcation roof and extending into the furcation. Also, a groove might exist within the concavity (Figure 4). Enamel pearls or projections could also be present at the mid-buccal CEJ and concavity. Enamel projections are found more frequently in the mandibular molars than the maxillary molars (2:1), and perhaps more frequently on second molars.3 The prevalence, however, has been shown to be significant in molar teeth (eg, 72%).4 The association of enamel projections and furcation involvement is statistically significant, indicating the role these anomalies play in the progression of periodontal diseases.3,4 As for the proximal surfaces, the mesial is flat and has a slight concavity and the distal is flat to convex (Figure 5).
Again, assessing the degree of furcation involvement is paramount for thorough periodontal debridement and tooth survival rates. The buccal furcation is only 3 mm from the CEJ and the lingual furcation is only 4 mm from the CEJ. The furcation openings are a little wider than the maxillary molars at 0.75 mm to 1 mm. Lastly, the internal structure, if exposed, is challenging to instrument during nonsurgical periodontal therapy (Figure 6).
This molar has a mesial proximal cervical curvature of 1 mm, and no curvature on the distal surface. This mandibular molar’s length is about 14 mm and its diameter is 10.5 mm from buccal to lingual. It is also a very wide tooth where extension to the midline with curets is challenging.1
INSTRUMENT SELECTION
Large and tenacious deposits will likely be present, accompanied by significant subgingival oral biofilm during initial nonsurgical periodontal therapy. Consequently, ultrasonic instrumentation with large and/or edged inserts/tips, as well as hand-activated instruments are recommended. Hand-activated instruments employed to initiate the instrumentation process might include working files (eg, Hirschfeld 3/7 and 5/11); universal curets (eg, Columbia 4R/4L); and Gracey area-specific curets (eg, 11/12 or 13/14). If using area-specific curets, choose rigid or extra-rigid shanks to enhance removal of heavier tenacious deposits. Flexible shanks might not provide the strength needed to break and remove the deposit piece by piece as it is channeled.5,6

After larger and tenacious deposits are removed, finer hand-activated instruments will be incorporated. Examples of universal designs are the Columbia 13/14 or the Barnhardt 1/2 or 5/6. Gracey area-specific standard curets with flexible shanks are appropriate for this stage of the instrumentation process because of the remaining lighter deposit. A flexible shank permits moderate and fine deposit removal while decreasing the potential for causing unnecessary root striations and gouging.
Also, Gracey area-specific extended shank designs indicated for deep pocket depth should be considered. With a 3 mm longer shank and a narrower working end than the standard design, these instruments may aid clinicians in reaching probing depths of 5 mm or greater. Another Gracey area-specific extended shank option is the mini-bladed instrument, which has a blade length 50% shorter than extended shank or standard instruments. They are ideal for open and/or exposed furcation involvement (Grade II or greater) on these molars. Lastly, micro mini-bladed Gracey curets are the smallest of the series, making them ideal for concavities, depressions, and furcation involvement.
CONCLUSION
First molar teeth provide isolated challenges in instrumentation due to the complex root anatomy. Memorizing the potential anatomy and proper instrument selection from a robust hand-activated instrument armamentarium are key to successful hand instrumentation of this part of the dentition.
REFERENCES
- Hodges KO. Instrument selection: philosophy and strategies. Concepts in Nonsurgical Periodontal Therapy. Boston: Delmar Publishers; 1998.
- American Academy of Periodontology. Task Force Report on the Update to the 1999 Classification of Periodontal Diseases and Conditions. J Periodontol. 2015;86:838–943.
- Bhusari P. Prevalence of enamel projections and its co-relation with furcation involvement in maxillary and mandibular molars: a study on dry skull. J Indian Soc Periodontol. 2013;17:601-604.
- Zee KY, Bratthall G. Prevalence of cervical enamel projections and its correlation with furcation involvement in eskimos dry skulls. Swed Dent J. 2003;27:42–48.
- Hodges KO. Incorporating channeling into instrumentation. Dimensions of Dental Hygiene. 2013;11(7):31–36.
- Hodges KO. Channeling for success. Dimensions of Dental Hygiene. 2013;11(5):34–37.
From Dimensions of Dental Hygiene. May 2018;16(5):16-18.

{kind=link}