
Expand Your Practice
How incorporating dental hygienists into multidisciplinary health care teams can improve health outcomes.
This course was published in the March 2011 issue and expires March 2014. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss why expanding the practice of dental hygienists into other medical specialities may benefit health outcomes.
- List the medical specialities that are most suitable for dental hygienists’ skill sets.
- Explain the barriers to expanding the practice of dental hygienists.
- Detail the steps needed to facilitate the expansion of dental hygiene practice.
The American health care delivery system is currently under intense scrutiny because of President Obama’s health care reform bill. The current reform effort is driven by the increasingly high costs of health care, the large number of uninsured, and an overall dissatisfaction with many health care outcomes.
In 2008, approximately $2.4 trillion was spent on health care in the United States.1 Left unchecked, this amount is projected to reach $3.1 trillion in 2012 and $4.3 trillion by 2016.1 The dollars spent on health care approach 17% of the United States’ gross domestic product.1 In addition to extremely high
health care expenditures, the nation also has approximately 47 million uninsured citizens.2
While many argue that the American health care system is the best in the world, it falls short in numerous areas. The current delivery of health care needs to become more cost-effective and produce better outcomes. One approach to making these goals a reality is to introduce new paradigms that will expand the roles of health care providers and encourage
greater cohesion within the system. The time for greater utilization of dental hygienists by expanding their practice settings into medical specialties has come. Allowing dental hygienists to see more patients in a wider variety of settings can improve both oral and systemic health while increasing access to care.
The evidence is clear—oral and systemic health are undoubtedly intertwined. This link drives the need to expand the alternative practice settings of dental hygienists to include
medical specialties. Dental hygienists currently work in some nontraditional settings, such as schools, public health clinics, hospitals, managed care organizations, correctional institutions, and nursing homes, and their efficacy in these settings demonstrates the potential that dental hygienists have to offer in the medical arena.
NURSING HOME/LONG-TERM CARE FACILITIES
In 2004, the California Task Force on Oral Health and Aging looked at the oral health of some elderly residents of nursing homes.3 The task force found that many residents had chipped teeth, untreated gingivitis and decay, and ill fitting prosthetic devices. The report also noted that many residents needed help with their daily oral hygiene care but most of the investigated nursing homes were understaffed to the point where daily dental care was either not performed at all or not done optimally.3 Unfortunately, the need for better dental care in nursing homes is not unique to California.
Proper dental care in the nursing home setting can have far reaching positive effects on overall health. A study investigating the effect of professional oral health care and respiratory infection was conducted on older adults living in nursing homes. One group received professional oral health care provided by dental hygienists and the other did not. The levels of microorganisms, respiratory infection pathogens, enzymatic activity in saliva, and prevalence of pneumonia were examined in both groups. The group that received professional oral health care by dental hygienists had significantly lower levels of potent respiratory pathogens, as well as reduced rates of fatal aspiration pneumonia, fever, and influenza.4
Dental hygienists currently work in the longterm care setting either as independent contractors or as employees of an affiliated dentist or the facility itself. Nursing homes and longterm care facilities are potential growth areas for dental hygienists, especially in states where some level of independent practice is allowed.
UNCHARTED TERRITORY
The American health care delivery system currently employs physician’s assistants, nurse practitioners, pharmacy technicians, and assistants for physical and occupational therapists. When these allied personnel are used to the full extent of their training and scopes of practice, health outcomes improve and financial savings are gained. A logical extension of this concept is to expand the dental hygienist’s practice settings to include a broad base of medical specialties. Following are medical specialties that are particularly well suited for dental hygienists’ unique skill sets.
FAMILY PRACTICE
Family medicine is a form of primary care that provides continuing, comprehensive health care for the individual and family across all ages, sexes, diseases, and parts of the body. Dental hygienists working in a medical practice can assess the oral health status of each patient, plan appropriate care strategies, implement oral health literacy plans, refer patients for needed dental care interventions, and assess the outcomes of the care plan at subsequent medical appointments.
INTERNAL MEDICINE
Internal medicine is focused on the health of the internal organs in adults, including the diagnosis and treatment of disorders affecting the internal organs. Internal medicine encompasses the treatment of cardiovascular disease, diabetes, gastrointestinal disorders, liver disease, and anemia. Employing a dental hygienist within an internal medicine practice provides the physician with a practitioner who can recognize and help diagnose diseases through examination of the oral cavity.
Studies show people with periodontal diseases are at an increased risk of cardiovascular disease and stroke.5 Oral-based bacterial infections contribute to the inflammatory process, which is a significant component of heart disease and stroke.6 Besides providing preventive services, dental hygienists can also assist these patients with xerostomia management, a common side effect of the pharmacologic treatment of both heart disease and stroke.
Diabetes is a debilitating and expensive disease to treat, and it is becoming more prevalent in the United States every year.7 The relationship between periodontitis and diabetes works both ways—periodontitis is a major complication of diabetes and periodontitis increases the risk of poor glycemic control among people with diabetes.8 Dental hygienists are well suited to perform glucometer testing, nutritional counseling, and oral health instruction with this patient population. Older adults frequently face gastroesophageal reflux disease (GERD). Patients with
GERD often experience an increase of acid in the oral cavity, which can cause erosion of enamel and exposure of the underlying dentin.9 Dental hygienists can perform oral
examinations to reveal any exposed dentin and help confirm the presence of GERD.
Chronic liver disease impacts the coagulation pathway by impeding the proper absorption of vitamin K from the intestines. Additional clotting factors in the clotting cascade
are also synthesized in the liver, therefore, impaired liver function interferes with hemostasis.10 Orally, this may manifest as petechiae or excessive gingival bleeding. These signs are especially indicative when no obvious oral inflammation is observed.10 The dental hygienist examining the oral cavity and noticing
the absence of inflammation in the presence of petechiae and/or excessive oral bleeding will be alerted to the strong possibility of underlying liver disease.
Eating habits among older adults commonly exclude essential minerals necessary for the prevention of anemia. Oral manifestations of anemia include mucosal pallor and or
glossitis. Oral examination easily reveals these symptoms.

OBSTETRICS AND GYNECOLOGY
Pregnancy significantly alters the oral health of expectant mothers.11 The physiologic changes that occur during pregnancy can exacerbate pre-existing periodontal conditions such as gingivitis and periodontitis. Evidence shows an association between periodontal infection and adverse pregnancy outcomes, such as premature delivery and low birth weight.12 Evidence also suggests that most young children acquire caries-causing bacteria from mothers. Improving the oral health of expectant and new mothers, and providing oral health counseling may reduce the transmission of such bacteria from mothers to children, thereby delaying or preventing the onset of caries.11
ENT/HEAD AND NECK
An otolaryngologist or ear, nose, and throat (ENT) physician deals with the diagnosis and treatment of disorders of the head and neck. A subspecialty of otolaryngology focuses on the treatment of cancerous and noncancerous tumors of the head and neck. In this setting, the dental hygienist can play a vital role identifying abnormal manifestations and disease processes.
RADIATION/ONCOLOGY
Cancer therapy cannot begin until a patient’s oral infections have been successfully treated and/or eliminated.13 The side effects of chemotherapy, such as regurgitation and nausea, decrease oral pH and can result in dental caries. Radiation therapy destroys salivary glands, which causes a marked reduction in salivary flow and increases the risk of decay. Patients undergoing radiation therapy and chemotherapy are susceptible to mucositis, which can result in weeks of red, painful blisters on the mouth, throat, and tongue.
Oral side effects occur in virtually all patients receiving radiation for head and neck malignancies, in approximately 80% of transplant recipients, and in about 40% of patients receiving primary chemotherapy.14 Patients are often warned of potential side effects but they are rarely offered or provided oral care.
Dental hygienists are the ideal professionals to provide the preventive, therapeutic, and educational services needed by cancer patients. They can help maximize the oral health of these patients prior to and during treatment. Oral hygiene instruction should be stressed, with emphasis on educating patients on what to expect and providing them with the armamentarium to alleviate symptoms.
PREVENTIVE MEDICINE
Preventive health physicians focus on helping to protect, promote, and maintain health, as well as prevent disease, disability, and premature death. The preventive medicine specialty is an ideal practice setting for the newly evolving dental hygiene specialty: oral health coach. An oral health coach creates and manages strategic plans—in collaboration with patients—to help them meet their personal oral health goals and immediate dental health needs. Oral health coaches assess the oral health status of patients, provide the information needed to make educated decisions about their oral health, and refer them for oral disease treatments as needed.
PEDIATRIC AND ADOLESCENT MEDICINE
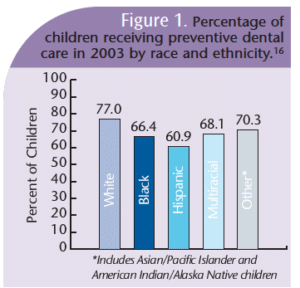
Pediatric medicine focuses on the treatment of infants and children. Adolescent medicine is a medical subspecialty that focuses on the care of patients from puberty to adulthood. Oral health screenings are traditionally done during visits to the dental office. This opportunity, however, is lost when dental visits are not part of a child’s routine. In a study conducted by the Institute for Health Policy Studies, researchers discovered that over the past 2 decades the number of children who receive no dental care fell from 38.5% to 26.3%.15 While this improvement is significant, more than one-quarter of children between the ages of 2 years and 17 years are not receiving oral health services.15
Figure 1 demonstrates the relationship between race and access to care.16 The existence of these disparities begs the implementation of a solution to address the problem. Dental hygienists are uniquely qualified to screen for dental and oral health problems. Likewise, they can provide necessary oral health literacy information to the child and parent, apply topical fluoride, and provide proper referrals to patients who need additional or more extensive treatment. Interventions by dental hygienists can be greatly facilitated by the use of screening instruments.

GERIATRIC MEDICINE
Including the dental hygienist as part of the medical team at the very beginning of health care experiences can work as a preventive measure against oral diseases. Unfortunately, many older adults do not receive any oral preventive care,17 and thus have untreated oral disease. One way to address this problem is to include an oral health screening by a dental hygienist as part of an examination in primary physicians’ and specialists’ offices.
This screening can be done to detect special needs related to dental caries and tooth loss, periodontal diseases, oral pharyngeal cancer, oral mucosal lesions, candidiasis, and temporomandibular disorders, as well as screen for oral indicators of systemic diseases.17 Dental hygienists can become part of a patient’s health status screening team to guide the patient through the self-screening checklist and perform the visual examination. Dental hygienists can then develop the dental hygiene treatment plan and make appropriate referrals.
RECOMMENDATIONS
Expanding the practice of dental hygienists into the medical arena has many positive benefits but there are still significant barriers to overcome. First, the support of dentists must be secured. The leadership of medical professionals must also recognize and support the need for dental hygienists in alternative practice settings. Reimbursement systems and referral mechanisms must be created. State Medicaid/Medicare agency support must be achieved. Appropriate training would be required, as well.18 The American Dental Hygienists’ Association is addressing these issues as it promotes the advanced dental hygiene practitioner (ADHP). With advanced education, dental hygienists can earn the designation of ADHP and provide preventive and basic restorative oral health care to people with limited or no access to oral health care services in a more cost-effective manner.
Elements that will facilitate the development and implementation of alternative models of delivering preventive oral health care services include:
- Greater public awareness of the need for good oral health.
- Destigmatizing of services provided by nondentists as new oral health care providers emerge.
- Promotion of the new oral health care provider model and making it eligible for reimbursement.
- Additional study in medical specialties at the individual provider level to learn exactly what elements are necessary to make dental hygiene practice successful.18
Conclusion
As the provisions of the new health care reform bill are implemented, the dental hygiene profession must address and eliminate the barriers preventing dental hygienists
from working in all medical specialty settings. The reduction of health care costs and improved oral health status outcomes can be realized by broadening the scope of dental hygienists into all facets of health care.
The connections between oral and systemic health have been well established. What has not been addressed are ways to use these connections both diagnostically
and prophylactically to improve outcomes without increasing costs. The dental hygienist is uniquely positioned to bridge this gap by serving in settings outside the dental office.
REFERENCES
- Keehan S, Sisko A, Truffer C, et al. Health spending projections through 2017: the baby boom generation is coming to Medicare. Health Aff (Millwood). 2008;27:145-155.
- California Health Care Foundation. Medi-Cal beneficiaries with disabilities: comparing managed care with fee-for-service systems. Available at: www.chcf.org/publications/2005/08/medical-beneficiaries-with-disabilitiescomparing-managed-care-with-feeforservicesystems. Accessed February 9, 2011.
- Glassman P, Henderson T, Helgeson M, et al. Oral health for people with special needs: consensus statement on implications and recommendations for the dental profession. Calif Dent Assoc. 2005;33:619-623.
- Adachi M, Ishihara K, Abe S, Okuda K. Professional oral health care by dental hygienists reduced respiratory infections in elderly persons requiring nursing care. Int J Dent Hyg. 2007; 5:69-74.
- Meurman JH, Sanz M, Janket S. Oral health atherosclerosis and cardiovascular disease. Crit Rev Oral Biol Med. 2004;15:403-413.
- Epstein SE. The multiple mechanisms by which infection may contribute to athero sclerosis development and cause. Circ Res. 2002; 90:2.
- Mokdad AH, Bowman BA, Ford ES, Vinicor, F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the United States. JAMA. 2001;286:1195-1200.
- Ryan ME, Carnu A, Kamer A. The influence of diabetes on the periodontal tissues. J Am Dent Assoc. 2003;134:345-405.
- Ali DA, Brown RS, Rodriquez LO, Moody EL, Nasr MF. Dental erosion caused by silent gastroesophageal reflux disease. J Am Dent Assoc. 2002;133:734-737.
- Gurenlian JR. Inflammation: the relationship between oral health and systemic disease. Access. 2006;20(4):19.
- Boggess KA, Society for Maternal-Fetal Medicine Publications Committee. Maternal oral health in pregnancy. Obstet Gynecol. 2008;111: 976-986.
- Jeffcoat MK, Geurs NC, Reddy MS, Cliver SP, Goldenberg RL, Hauth JC. Periodontal infection and preterm birth: results of a prospective study. J Am Dent Assoc. 2001;132:875-880.
- Hong CH, Napeñas JJ, Hodgson BD, et al. A systematic review of dental disease in patients undergoing cancer therapy. Support Care Cancer. 2010;18:1007-1021.
- National Institute of Dental and Craniofacial Research. Oral complications of cancer treatment: what the oncology team can do. Available at: www.nidcr.nih.gov/oralhealth/topics/cancertreatment/oralcomplicationscanceroncology.htm. Accessed February 9, 2011.
- Hughes DC, Duderstadt KG, Soobader MP, Newacheck PW. Disparities in children’s use of oral health services. Public Health Rep. 2005;120: 455-462.
- Health Resources and Services Administration, Maternal and Child Health Bureau. The National Survey of Children’s Health 2003. Rockville, Md: US Department of Health and Human Services; 2005.
- Lamster IB, Northridge ME. Improving Oral Health for the Elderly. New York: Springer; 2009. 18. Center for Health Services Research and Policy, School of Public Health and Health Services. Research on the Impact of Laws and Policies on Public Health. Washington, DC: George Washington University Medical Center; 2010.
From Dimensions of Dental Hygiene. March 2011; 9(3): 80-83.
