
Changing the Rules
The use of extraoral fulcrums can mean the difference between success and failure in periodontal therapy.
Many of the traditional “rules” of hand instrumentation, such as the insistence on only using intraoral toothborne finger rests, are legacies from the era when most scaling—particularly by dental hygienists—was done supragingivally. In the early part of the 20th century, a large percentage of the American population was composed of children and young adults. These age groups suffered more from caries than periodontal diseases. Older patients with periodontitis and pockets with subgingival deposits were not as prevalent in dental operatories as they are today.

right molars. © ANNA M. PATTISON, RDH, MS
In the 1920s, the first dental hygienists were taught to perform a “prophylaxis” as a preventive procedure to remove supragingival deposits in a relatively healthy mouth of a child or young adult. Periodontitis patients were treated by a small number of dentists or pioneer periodontists who would scale subgingivally or perform periodontal surgery. As there were not enough periodontists or skilled dentists to treat all of these patients, many received only supragingival scaling. For decades, the periodontal needs of patients were not adequately met and many teeth were needlessly extracted.
Today, the United States has more older adults than ever before, and this affects both dentistry and dental hygiene. Because we have succeeded in decreasing the caries rate, more of these patients have their full dentition but now suffer from periodontitis. Unfortunately, many clinicians and dental hygiene educators still use and teach techniques that were originally intended for supragingival calculus removal. Periodontists alone cannot treat the millions of patients with periodontitis; general dentists and dental hygienists must become better educated to perform advanced periodontal instrumentation. Clinical education should incorporate innovative extraoral and alternative fulcrums with newer hand instruments, such as mini-bladed curets, to adequately prepare graduates for these challenges.
Meeting the Needs of Patients
In dental hygiene, the development of advanced periodontal instrumentation has been thwarted by two main factors: rigid adherence to old rules of supragingival instrumentation that include using only intraoral fulcrums, and the inability of dental hygienists in many states to administer local anesthesia.

posterior teeth using wrist motion results in a
shorter, shallower stroke. © ANNA M. PATTISON, RDH, MS
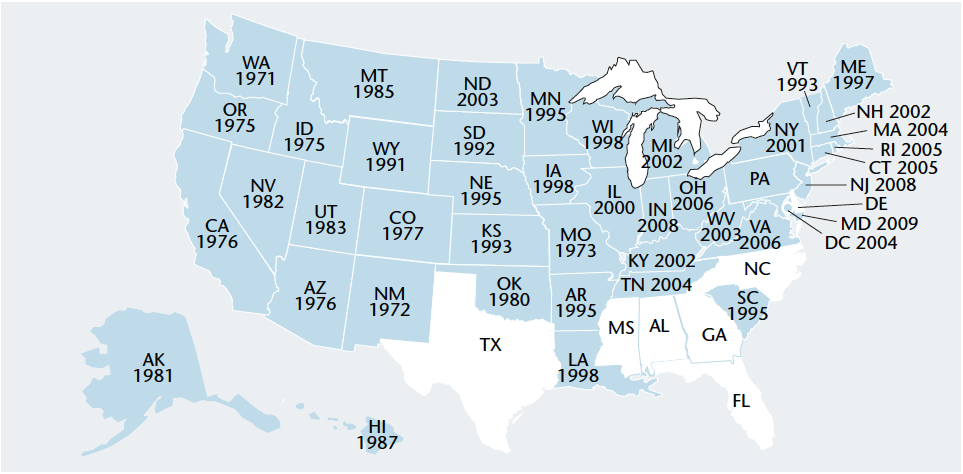
Beginning in 1971, several Western states passed laws allowing dental hygienists to administer local anesthesia. As the dental hygienists in these states began to use local anesthesia to scale in deeper pockets of more involved periodontal patients, they developed extraoral and alternative fulcrums to overcome the limitations of traditional intraoral fulcrums and positions. For the past 40 years, extraoral fulcrums have been taught in many Western dental hygiene schools, including thousands of students at the University of Southern California. Today, 43 states and the District of Columbia allow dental hygienists to administer local anesthesia (see Figure 1).1 As more dental hygienists use local anesthesia, the transition from traditional intraoral finger rests to more advanced fulcrums and positions is gradually occurring.
Strict adherence to intraoral fulcrums for the maxillary posterior teeth is especially problematic. The practice of using an intraoral fulcrum on the premolars and reaching back to the molars with a Gracey 11/12 or 13/14 is a perfect example (Figure 2). This ineffective split fulcrum technique is still taught and being used by thousands of dental hygienists. Separating the grasping fingers from the fulcrum finger and dropping the handle into the web of the hand commits the clinician to finger flexing and results in a short, weak, shallow, picking stroke that will not extend deeply enough. If it is able to reach the calculus in a deep pocket, the stroke will usually fail to remove the calculus completely and will “shave” over the deposit instead of breaking it away from the root surface. If the fingers are kept together and wrist motion is used with a palm-up fulcrum, the stroke is stronger but still too short for deep pockets (Figure 3). The use of extraoral, opposite arch, and reinforced fulcrums allows a longer, more powerful, even stroke in deeper pockets and permits ideal blade adaptation and angulation in areas where this is difficult to achieve with traditional intraoral fulcrums.

right posterior teeth from a 9 o’clock position
allows deeper insertion, dominant thumb position,
constant ideal angulation, and strong strokes.
Palm is facing up away from the patient’s face. © ANNA M. PATTISON, RDH, MS
Clinicians who prefer ultrasonic scaling over hand instrumentation may not realize that the superior access and adaptation attributed to ultrasonics is directly related to the extraoral fulcrums used. Many of these clinicians routinely use extraoral fulcrums with ultrasonic scalers but not with hand instruments. Using extraoral fulcrums with both hand and ultrasonic instrumentation allows better adaptation and angulation to be maintained throughout the procedure.
Elements of the Extraoral Fulcrum
Some clinicians believe that extraoral fulcrums should not be used because they are too unstable and may result in slipping and injury to the patient. This is very true if a one-point finger rest is attempted, however, the extraoral hand rest as described here uses a substantial portion of the front or back surfaces of the fingers and hand.
There are three essential elements for a stable extraoral hand rest.

posterior, mesio-lingual approach). An extraoral
fulcrum is established on skin overlying the
mandible on the left side of the face. The index
finger of the nonoperating hand is applying
pressure to the shank. © ANNA M. PATTISON, RDH, MS
The first involves maximizing the surface area of contact between the hand and the patient’s face (Figure 4). Usually a second element is the firmness used in placing the hand rest. Secure extraoral hand rests depend on the establishment of pressure against the face and underlying bone that is equal to that exerted against the tooth by the blade. A reinforcing finger from the nondominant hand can also be used to maintain adaptation and force (Figure 5).
The final element of an effective extraoral hand rest is an extended grasp. Sitting in a 9 o’clock position, place the thumb in a dominant position approximately one-third of the way down the instrument handle, away from the working end (Figure 6). The modified location of this grasp is necessary because without the extension, the instrument will not span the distance between the tooth surface and the hand rest. Clinicians accustomed to intraoral finger rests may be reluctant to use this grasp because they believe that instrument control is dependent on a grasp close to the working end. This is a common misconception. It is the fulcrum pressure, rather than the closeness of the grasp, that determines whether a stroke will be well controlled. Lack of control occurs when inadequate pressure is applied to the hand rest.
Plan of Action

in a dominant position, one-third of the way down
the handle away from the working end. Extraoral
palm-down rest for maxillary left posterior teeth. © ANNA M. PATTISON, RDH, MS
There was a time in the 1960s and 1970s when many patients with deep pockets and moderate to advanced periodontitis were referred immediately to the periodontist. The periodontist or dental hygienists in the periodontal practice would perform initial quadrant scaling and then periodontal surgery would be performed on the areas of remaining pocket depth. It is estimated that 90% of deep periodontal scaling is performed by dental hygienists in the general dental practice.2 A survey of 600 general dentists in Virginia found that 86% reported providing periodontal maintenance in their practices, and 58% reported that 90% or more of the scaling and root planing was performed by dental hygienists.3 Five thousand periodontists cannot possibly treat all of the periodontitis patients in this country. Dental hygienists today must meet the needs of the millions who currently have active periodontal disease. Replacing antiquated techniques and instruments with better alternative fulcrums, new specialized hand instruments, and improved ultrasonics will allow clinicians to deliver state-of-the-art periodontal care.
References
- American Dental Hygienists’ Association. States where dental hygienists can administer local anesthesia. Available at; www.adha.org/governmental_affairs/downloads/localanesthesiamap.pdf. Accessed May 5, 2011.
- American Dental Association. The 2005-2006 Survey of Dental Services Rendered. 2007:35.
- Lanning SK, Best AM, Hunt RJ. Periodontal services rendered by general practitioners. J Periodontol. 2007;78:823-832.
From Dimensions of Dental Hygiene. May 2011; 9(5): 52-54.

{kind=link}