 ZLIKOVEC/ISTOCK/GETTY IMAGES PLUS
ZLIKOVEC/ISTOCK/GETTY IMAGES PLUS
Caring for the Primary Dentition
Managing teething pain, preventing caries, and educating parents/caregivers are key facets of oral health care when treating young patients.
Vast developmental oral changes occur in children during the first 6 years of life. The amount of education needed to properly care for the primary dentition may seem overwhelming to parents/caregivers. Developing an effective self-care regimen requires a team effort between children, parents/caregivers, and oral health professionals.
TEETHING
The American Dental Association (ADA), American Academy of Pediatrics, American Academy of Pediatric Dentistry (AAPD), and American Association of Public Health recommend that children have their first dental visit by the age of 1.1–3 This is generally within 6 months of the eruption of the first tooth. In many children, tooth eruption begins around 6 months and can last until age 3, averaging one new tooth every month during this period.4 Tooth eruption (teething) can bring localized and systemic discomfort, as it is a combination of trauma, inflammation, and healing.5 During the teething process, immunoregulatory events enable the tooth’s eruption pathway to occur through the bone and gingiva.5 This complex process involves the release of cytokines, activation of osteoclasts, and diffusion of glycoproteins in the blood.5 This physiological process triggers an inflammatory immune response, causing pain and fever5,6 along with gingival irritation, sleep disturbance, loss of appetite, upset stomach, and irritability.4–7 Discomfort associated with teething lasts approximately 8 days per tooth, 4 days prior to tooth eruption and 4 days after.7
Common methods to alleviate the discomfort caused by teething are chilled teething rings or pacifiers, massaging the gingiva, antipyretics, analgesics, and topical anesthetic agents or teething gels.6 Recently, the United States Food and Drug Administration (FDA) published guidelines regarding teething gels. The FDA states: “Teething is a normal part of childhood and should not be treated with homeopathic remedies, like teething tablets, or prescription or over-the-counter medications that are rubbed on the gums.”8 Topical agents generally are quickly washed away by saliva, are ineffective, and potentially hazardous.8 The current FDA recommendations are particularly important for children younger than 2.8
Benzocaine is a topical anesthetic agent used prior to the administration of local anesthesia injections. It has been safely administered in the dental office for years and is available over the counter. Products that contain benzocaine—such as ointments, gels, creams, liquids, and sprays—have concentrations that range from 6% to 20%. Benzocaine provides quick relief, can take effect in as little as 30 seconds, and offers a duration of up to 15 minutes.
The concern regarding benzocaine is its ability to induce methemoglobinemia, a rare but serious blood disorder in which an abnormal amount of methemoglobin is created. Methemoglobinemia occurs when oxidizing agents, such as benzocaine, oxidize hemoglobin into methemoglobin. Oxygen cannot bind with methemoglobin, resulting in a decrease in the amount of oxygen released into body’s tissues.9
Signs and symptoms of methemoglobinemia can occur within minutes to hours after administration and include dizziness, shortness of breath, and cyanosis of the skin or mucous membrane. Severe complications such seizures, coma, and death can occur. Repeated use, excessive dosing, and long duration all increase the risk of methemoglobinemia, however, it can develop after a single dose.8 Children younger than 2 are particularly susceptible because they lack a sufficient amount of nicotinamide adenine dinucleotide (NADH)-dependent methemoglobin reductase, which is necessary to reduce methemoglobin back to hemoglobin, and they have an increased body-mass-to body-surface ratio compared with adults.10
Benzocaine can also cause localized adverse reactions, such as burning, stinging, skin sloughing, and discoloration of the tissue. These symptoms may be mistaken for teething pain, resulting in additional applications of the medication and increasing the risk of overdose. Dental hygienists should discuss the current FDA safety warnings regarding benzocaine with their patients and parents/caregivers and provide recommendations for safe alternatives.
To manage teething pain, the American Academy of Pediatrics recommends the use of a firm rubber teething ring vs one that is frozen to prevent trauma and injury to the gingiva.11 The teething ring should also be large enough to ensure it is not a choking hazard.11 The child’s physician should be consulted before recommending any pain medicine for teething.
PROTECTING THE PRIMARY DENTITION
The primary dentition is necessary for acquiring adequate nutrition, maintaining space for permanent teeth, and facilitating speech development.12 The importance of the primary dentition goes beyond function, as its health relates to the health of permanent teeth, especially when it comes to caries.13
Dental caries is a significant public health concern and the most prevalent chronic disease in children.14 The ADA defines early childhood caries as the presence of one or more decayed, missing, or filled tooth surfaces in any primary tooth in children between birth to age 6.1 Prevention strategies must start as soon as the first tooth erupts. Parents/caregivers may wrongly believe that decay in the primary dentition ends when the teeth are shed.15 While caries is an infectious, transmissible disease, when managed properly, it can be effectively prevented and possibly arrested.16
Implementing effective preventive strategies may prevent the need for lifelong and invasive intervention. Extensive decay in young children may require surgery and general anesthesia.15 Rates of retreatment for dental caries that require general anesthesia are high (50%).15 Parents/caregivers need to be informed about the etiology of caries and preventive strategies, such as fluoride, plaque control, and diet modifications.15 Caries risk assessment should also be part of every pediatric dental appointment.17
ORAL HYGIENE
Biofilm control is a major contributor in caries prevention. Primarily, biofilm control should be initiated at home. To clean an infant’s mouth, parents/caregivers can use a soft wash cloth to gently wipe the gingiva. Toothbrushing with a soft brush should start as soon as the first tooth erupts. Parents/caregivers should assist their children with brushing twice daily and flossing closed contacts daily until age 3. The AAPD recommends supervising oral hygiene twice daily until the child is at least 8.18,19 A general rule is once children gain enough dexterity to tie their own shoes, they are most likely able to independently brush their teeth.
Demonstrating brushing technique is critical for patients and parents/caregivers. Caregivers value practical tips and demonstration of proper technique over the mere transmission of information.15 One study showed that parents preferred demonstrations and found them more effective over verbal recommendations, pamphlets, and printed information.15 Using the tell-show-do approach is effective.20 A toothbrush prophylaxis is efficient in removing plaque in most young children and is an opportunity to demonstrate proper brushing/flossing technique.20
FLUORIDE
For additional caries prevention, fluoride toothpaste should be used, starting with a small smear or the size of a rice grain from ages 0 to 2. The amount of toothpaste can be increased to a pea-sized amount from ages 3 to 6.21 Children older than 6 may use a 0.05% sodium fluoride mouthrinse on a daily basis to decrease caries risk.22 Fluoride mouthrinse is not recommended for children younger than 6, due to the risk of fluorosis if repeatedly swallowed.22
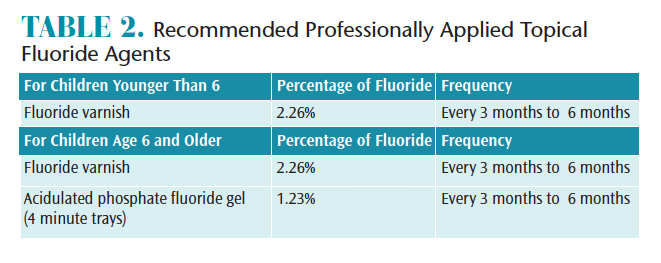
Professional application of topical fluoride can begin with tooth eruption for children at elevated caries risk.23 For children younger than 6, only fluoride varnish is recommended. For children age 6 and older, both fluoride varnish and acidulated phosphate fluoride (APF) gel are recommended for caries prevention. Evidence supports a 4-minute tray application time for APF gel.24,25
The professional application of silver diamine fluoride (SDF) can arrest carious lesions. It has also shown efficacy in preventing caries in tooth surfaces adjacent to carious lesions. However, it causes tooth staining; this side effect must be fully explained to patients and their parents/caregivers.26
The systemic use of fluoride is also effective in reducing tooth decay. Optimally fluoridated community water supplies can reduce caries rates by 20% to 40%.27 According to the US Department of Health and Human Services, 0.7 mg of fluoride per liter of drinking water is the most effective level to prevent caries.28 For individuals at elevated caries risk who do not have access to community fluoridated water, fluoride supplements are an option. Oral health professionals need to investigate all sources of patients’ fluoride exposure to reduce the risk of fluorosis.23
NONFLUORIDE CARIES PREVENTION
In the event parents/caregivers express concern regarding fluoride or decline its use, dental hygienists should discuss nonfluoride caries preventive agents. Sodium bicarbonate, or baking soda, is a highly soluble bacteriostatic agent that can penetrate oral biofilms and prevent the bacterial growth of Streptococcus mutans. Additionally, the alkalinizing properties of sodium bicarbonate increase salivary pH to neutral levels after the consumption of carbohydrate-rich foods when pH periodically becomes more acidic. Baking soda is found in dentifrices, but has shown efficacy in caries prevention as an oral rinse and in chewing gum in 2% and 4% concentrations.29,30
Xylitol is a five-carbon sugar alcohol that inhibits bacterial metabolism, increases salivary flow, and reduces vertical transmission of bacteria from mother to child.25,29 For caries prevention, the recommended daily dose is 5 g to 6 g consumed at least three or more times per day.31,32 The AAPD supports the use of xylitol for caries prevention in children who have moderate to high caries risk and the ADA supports xylitol use for children with a history of dental caries.33 Due to the risk of choking, however, the American Academy of Pediatrics advises against chewing gum use for children younger than 5 and those who have swallowing disorders.34
Additional caries preventive agents include chlorhexidine, arginine, calcium phosphate technologies, triclosan, sialogogues, and iodine.29 The ADA’s Center for Evidence-Based Dentistry published its findings regarding nonfluoride caries preventive agents, stating that more evidence is needed on the use of these methods in caries prevention.33 A chairside guide is available here: ebd.ada.org.
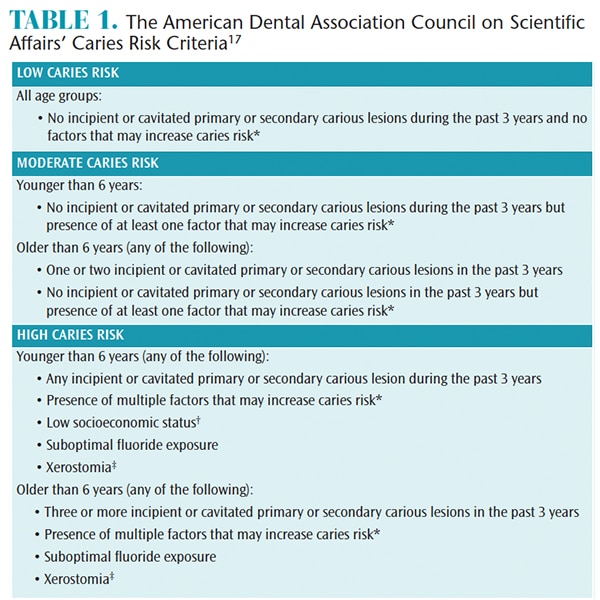
† On the basis of findings from population studies, groups with low socioeconomic status have been found to have an increased risk of developing caries.38,39 In children too young for their risk to be based on caries history, low socioeconomic status should be considered as a caries risk factor.
‡ Medication-, radiation- or disease-induced xerostomia. From: American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. J Dent Educ. 2007;71:393–402.
SEALANTS
The use of sealants is a well-documented caries prevention measure in the pits and fissures of posterior teeth.35 Approximately 90% of carious lesions present on posterior teeth.36 A recent Cochrane Review reports sealants produce an 11% to 51% reduction in occlusal caries compared with no sealant application.37 Pits and fissures require supplementary intervention to prevent biofilm retention as the tooth’s morphology creates anatomical spaces that retain biofilm.35,36,38 Sealants should be applied soon after tooth eruption to increase efficacy. Retention should be evaluated at each hygiene visit as retention rates decrease over time.39,40
The placement of sealants also provides future benefits. Medicaid data show that sealant placement on permanent first and second molars correlates with a reduced incidence in future restorative treatment.39 A study showed that children without sealants were three times more likely to have future restorative therapy.41 The same study also correlated sealant placement with less invasive cavity preparations when future restorations were indicated.41 Sealants are typically only covered by insurance when placed on permanent molars. However, any teeth at risk for caries can benefit from sealant placement.
![]() CONCLUSION
CONCLUSION
Establishing a strong foundation of accurate, effective, and safe oral health information with parents/caregivers can keep children healthy. Parents and caregivers should understand the correlation between oral health and their child’s general health and well-being.
REFERENCES
- American Dental Association. Statement on Early Childhood Caries. Available at: ada.org/en/about-the-ada/ada-positions-policies-and-statements/statement-on-early-childhood-carie. Accessed October 18, 2018.
- American Academy of Pediatric Dentistry. FAQs. Available at: aapd.org/resources/frequently_asked_questions/#311. Accessed October 18, 2018.
- American Association of Public Health. First Oral Assessment. Available at: apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2014/07/29/14/08/first-oral-health-assessment. Accessed October 18, 2018.
- Sarrell EM, Horev Z, Cohen Z, Cohen HA. Parents’ and medical personnel’s beliefs about infant teething. Patient Educ Couns. 2005;57:122–125.
- Lam CU, Hsu CY, Yee R, et al. Early-life factors affect risk of pain and fever in infants during teething periods. Clin Oral Investig. 2016;1:20:1861–1870.
- Lyttle C, Stoops F, Welbury R, Wilson N. Tooth eruption and teething in children. The Pharmacuetical Journal. 17 Nov 2015.
- Macknin ML, Piedmonte M, Jacobs J, Skibinski C. Symptoms associated with infant teething: a prospective study. Pediatrics. 2000;105:4:747–752.
- United States Food and Drug Administration. Risk of serious and potentially fatal blood disorder prompts FDA action on oral over-the-counter benzocaine products used for teething and mouth pain and prescription local anesthetics. Available at: fda.gov/Drugs/DrugSafety/ucm608265.htm. Accessed October 18, 2018.
- Rehman HU. Evidence-based case review: methemoglobinemia. West J Med. 2001;175:193.
- So T, Farrington E. Topical benzocaine-induced methemoglobinemia in the pediatric population. J Pediatr Health Care. 2008;6:335–339.
- American Academy of Pediatrics. Teething Pain. Available at: healthychildren.org/English/ages-stages/baby/teething-tooth-care/Pages/Teething-Pain.aspx. Accessed October 18, 2018.
- López-Gómez SA, Villalobos-Rodelo JJ, Ávila-Burgos L, et al. Relationship between premature loss of primary teeth with oral hygiene, consumption of soft drinks, dental care, and previous caries experience. Sci Rep. 2016;6:211–247.
- Çolak H, Dülgergil ÇT, Dalli M, Hamidi MM. Early childhood caries update: A review of causes, diagnoses, and treatments. J Nat Sci Biol Med. 2013;4:29–38.
- Benjamin RM. Oral health: the silent epidemic. Public Health Rep. 2010;125:158–159.
- Amin MS, Harrison RL. Understanding parents’ oral health behaviors for their young children. Qual Health Res. 2009;19:1:116–127.
- Kawashita Y, Kitamura M, Saito T. Early childhood caries. Int J Dent. 2011;2011::725320.
- American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. J Dent Educ. 2007;71:393–402.
- American Academy of Pediatrics. A Pediatric Guide to Children’s Oral Health: a Reference Guide. Available at: aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Oral-Health/Documents/OralHealthRefGuide.pdf. Accessed October 18, 2018.
- American Academy of Pediatric Dentistry. AAPD Reminds Parents and Caregivers to Brush Children’s Teeth Two Minutes, Twice a Day for a Healthy Halloween. Available at: aapd.org/aapd_reminds_parents_and_caregivers_ to_brush_childrens_teeth_two_minutes_twice_a_day_for_a_healthy_halloween/. Accessed October 18, 2018.
- Ramos-Gomez FJ, Crystal YO, Ng MW, Crall JJ, Featherstone JD. Pediatric dental care: prevention and management protocols based on caries risk assessment. J Calif Dent Assoc. 2010;38:746.
- American Dental Association Council on Scientific Affairs. Flouride Toothpaste Use for Young Children. Available at: jada.ada.org/article/S0002-8177(14)60226-9/fulltext?dgcid=PromoSpots_EBDsite_fluoride-toothpaste-young-children&code=adaj-site. Accessed October 18, 2018.
- Clark MB, Slayton RL. Fluoride use in caries prevention in the primary care setting. Pediatrics. 2014;134:626–633.
- American Dental Association. Fluoride: Topical and Systemic Supplements. Available at: ada.org/en/member-center/oral-health-topics/fluoride-topical-and-systemic-supplements. Accessed October 18, 2018.
- American Dental Association Council on Scientific Affairs. Professionally Applied Topical Fluoride. Evidence-Based Clinical Recommendations. Available at: ada.org/~/media/ADA/Science%20and%20Research/Files/ report_fluoride.ashx. Accessed October 18, 2018.
- Darby ML., Walsh MM, Bowen DM. Dental Hygiene: Theory and Practice. St. Louis: Elsevier/Saunders; 2015:586.
- Llodra JC, Rodriguez A, Ferrer B, et al. Efficacy of silver diamine fluoride for caries reduction in primary teeth and first permanent molars of schoolchildren: 36-month clinical trial. J Dent Res. 2005;84:721–724..
- American Dental Association. Fluoridation Facts. Available at: ada.org/en/public-programs/advocating-for-the-public/fluoride-and-fluoridation/fluoridation-facts. Accessed October 18, 2018.
- California Dental Association. Revised optimal fluoride level in drinking water released. Available at: cda.org/news-events/revised-optimal-fluoride-level-in-drinking-water-released. Accessed October 18, 2018.
- Macri D. Implementing a multifaceted approach to caries prevention. Dimensions of Dental Hygiene. 2018;16(5):21–25.
- Zero DT. Evidence for biofilm acid neutralization by baking soda. J Am Dent Assoc. 2017;48:S10–S14.
- Riley P, Moore D, Ahmed F, Sharif MO, Worthington HV. Xylitol-containing products for preventing dental caries in children and adults. Cochrane Database Syst Rev. 2015;3:CD010743.
- Richards D, Duane B, Sherriff A. Maternal consumption of xylitol for preventing dental decay in children. Available at: cochranelibrary-wiley.com/doi/10.1002/14651858.CD010202/abstract;jsessionid=A121CC3D4630C45CE876F1AA548CF8F6.f02t02. Accessed October 18, 2018.
- Rethman MP, Beltrán-Aguilar ED, Billings RJ, et al. Nonfluoride caries preventive agents. Full report of a systematic review and evidence-based recommendations. J Am Dent Assoc. 2011;142:1065–1071.
- American Academy of Pediatrics. Policy Statement—Prevention of Choking Among Children. Available at: http://pediatrics.aappublications.org/content/ pediatrics/early/2010/02/22/peds.2009-2862.full.pdf. Accessed October 18, 2018.
- Al-Jobair A, Al-Hammad N, Alsadhan S, Salama F. Retention and caries-preventive effect of glass ionomer and resin-based sealants: an 18-month-randomized clinical trial. Dent Mater J. 2017;36:654–661.
- Govindaiah S, Vinodh B. Dentists’ level of evidence-based clinical knowledge and attitudes about using pit-and-fissure sealants. J Am Dent Assoc. 2014;145:849–855.
- Ahovuo-Saloranta A, Forss H, Walsh T, et al. Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst Rev. 2017;7:CD001830.
- Naaman R, El-Housseiny AA, Alamoudi N. The use of pit and fissure sealants—a literature review. Dent J (Basel). 2017;5:34.
- Beauchamp Caufield PW, Crall JJ, et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2008;139:257-268.
- Folke BD, Walton JL, Feigal RJ. Occlusal sealant success over ten years in a private practice: comparing longevity of sealants placed by dentists, hygienists, and assistants. Pediatr Dent. 2004;26:5.
- Griffin SO, Naavaal S, Scherrer C, et al. Evaluation of school-based dental sealant programs: An updated community guide systematic economic review. Am J Prev Med. 2017;52:407–415.
From Dimensions of Dental Hygiene. November 2018;16(11):10,11–12.

{kind=link}
[…] into why some children present with caries, while others don’t. Clinicians can also develop a home-care regimen for parents and caregivers to effectively care for the child’s primary dentition, as well as […]
Currently working in Pediatrics this is a very valuable article for all RDH that have pediatric pts in their practice.