A Paradigm Shift
William Giannobile, DDS, MS, DMedSc, discusses how tissue engineering is changing the practice of dentistry, making restorations passé and regeneration possible.
Q. Please explain the concept of tissue engineering.
 A. Tissue engineering is a discipline that exploits living cells in a variety of ways to restore, maintain, or enhance tissues and organs. A more broad term—applicable to regenerative biology—is regenerative medicine. Regenerative medicine involves the manipulation of cells, extracellular matrices, and bioregulatory molecules to promote the repair, replacement, or enhancement of tissue or organ function. Regenerative medicine and tissue engineering have tremendous potential impact for dentistry and dental hygiene.
A. Tissue engineering is a discipline that exploits living cells in a variety of ways to restore, maintain, or enhance tissues and organs. A more broad term—applicable to regenerative biology—is regenerative medicine. Regenerative medicine involves the manipulation of cells, extracellular matrices, and bioregulatory molecules to promote the repair, replacement, or enhancement of tissue or organ function. Regenerative medicine and tissue engineering have tremendous potential impact for dentistry and dental hygiene.
Q. What techniques are used in tissue engineering?
A. Tissue engineering has grown into a very broad field that involves harvesting cells from patients or tissue banks that are then expanded and manipulated (via biochemical or genetic means) for delivery into a new site through the use of tissue scaffolds or carriers.
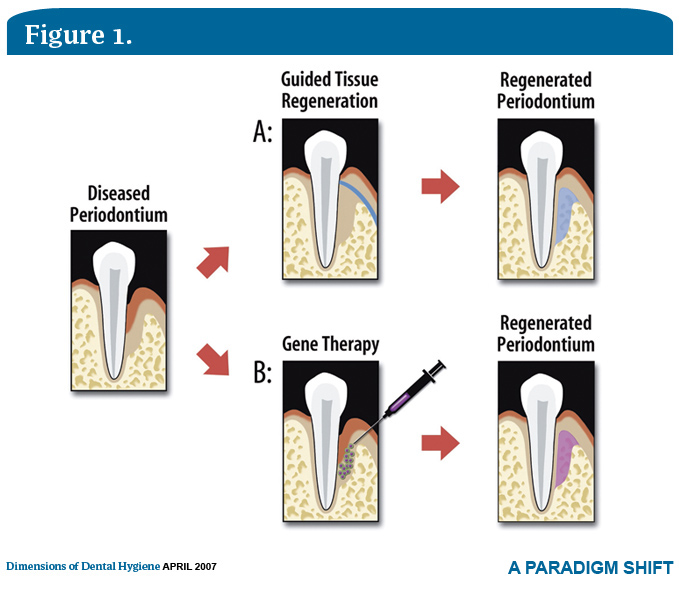
These approaches use scaffolds or templates that guide cells from the body in the vicinity of the defect or site of injury to repopulate and fill in the area of tissue destruction. Such techniques include cell therapy (cells harvested from the patient that are grown in the laboratory to expanded numbers and then delivered back to the individual, or modified cells from other individual tissue donors transplanted to defects or sites of compromised healing potential). Another approach is gene therapy, whereby genes that encode for a missing protein or a protein in short supply are delivered to the body. The goal of the transplanted genes is to produce therapeutic proteins at increased levels to substitute for the missing or depleted genes required to form more tissue or instruct the cells to develop into specific structures.
Q. Tissue engineering is a relatively new concept in dentistry. Is it more prevalent in medicine?
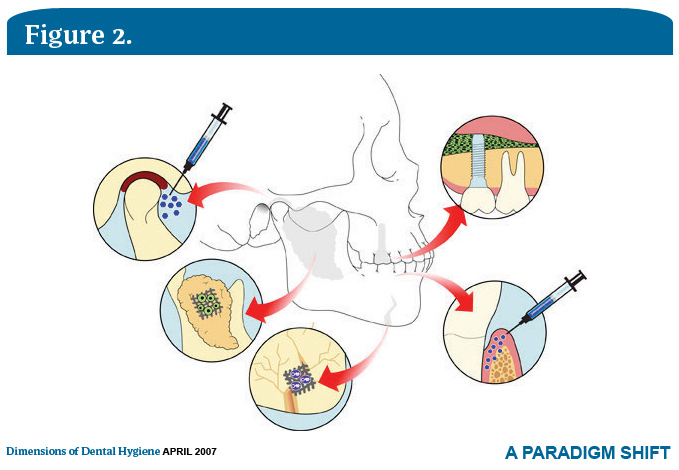
A. Actually, in terms of the potential benefits gained from tissue engineering, dentistry has the greatest number of current applications, eg, tooth extraction is the most common surgical procedure and tooth replacement has tremendous potential. Dental procedures stand to gain significantly from tissue engineering, such as bioactive dental implants, dental restorations, periodontal reconstruction, and endodontic repair of teeth.
Q. What are some common tissue engineering procedures in medicine?
A. In medicine, examples include bone repair of orthopedic fractures using growth factors and cell therapy, such as bone marrow harvest of regenerative cells that are combined with dissolvable biomaterial carriers to target cells directly to tissue defects caused by disease or injury. Regenerative growth factors have been approved by the Food and Drug Administration (FDA) for the treatment of nonhealing wounds in diabetics or burn victims. Tissue engineering approaches have been involved in repairing heart defects and other vascular diseases and injury. Early work on a bioartificial tissue engineered kidney is in clinical trials here at the University of Michigan. Gene therapy approaches using tissue growth factors are also in clinical trial testing to repair skin and bone wounds.
Q. What dental conditions might be treated with tissue engineering?
When considering tooth loss; tooth damage (due to disease such as dental caries or trauma); periodontitis; and other oral and craniofacial bone defects caused by trauma, congenital malformation or disease, dentistry leads medicine in the greatest need. Dental care as we know it today still revolves around restoration. Because of the great needs in restorative and reconstructive procedures (tooth replacement and repair and regeneration of tooth support), dentistry has received a lot of attention in tissue engineering.
Q. How is tissue engineering distinguished from regeneration?
A. Regeneration is the active process of forming new cells, tissues, or organs that reproduce a lost body part. Tissue engineering is the tool that leads to the end result of regeneration, considering techniques in the fields of engineering and life sciences.
Q. What is the dental hygienist’s role in tissue engineering?
 A. Dental hygienists are collaborators in oral health care delivery. With tissue engineering, they assemble diagnostic information that identifies and assesses the need and results of tissue engineering procedures. In the future, regenerative therapies could be as simple as the local delivery of regenerative molecules placed subgingivally to promote repair of periodontal and gingival defects. New drug delivery systems to stimulate wound repair of soft tissue and extraction defects may be as simple as applying medicaments directly to wounds. For example, dental hygienists can deliver and target antibiotics formulated in bioabsorbable polymers to treat periodontal diseases. These same polymers are used in tissue engineering for other forms of drug delivery, regenerative factors, or genetic material.
A. Dental hygienists are collaborators in oral health care delivery. With tissue engineering, they assemble diagnostic information that identifies and assesses the need and results of tissue engineering procedures. In the future, regenerative therapies could be as simple as the local delivery of regenerative molecules placed subgingivally to promote repair of periodontal and gingival defects. New drug delivery systems to stimulate wound repair of soft tissue and extraction defects may be as simple as applying medicaments directly to wounds. For example, dental hygienists can deliver and target antibiotics formulated in bioabsorbable polymers to treat periodontal diseases. These same polymers are used in tissue engineering for other forms of drug delivery, regenerative factors, or genetic material.
Q. Are new tissue engineering concepts in the development phase that we may see in the near future?
A. This is a very exciting time in the field of tissue engineering and dentistry and oral reconstruction. Active research is underway in areas ranging from tooth tissue engineering to gene therapy of periodontium to salivary gland repair. At the basic level, work in stem cell biology as it relates to cell transplantation for the repair of oral, craniofacial, and periodontal defects has shown significant potential. The use of tissue growth factors, such as bone morphogenetic proteins, has recently shown potential to treat major bone defects in the jaw. Materials science and biomedical engineering have been critical at the basic developmental level for dental tissue engineering.
Since the delivery and use of tissue scaffolds are important in the reconstruction of oral and dental tissues, research is focusing on new bioresorbable materials that provide the necessary architecture to allow the body to replace damaged or missing tissue. For example, biomaterials using image-based scaffolds generated from microcomputed tomography that are highly accurate three-dimensional radiographic images can be used as templates to tissue engineer portions of the mandible and cranial defects, as well as teeth or periodontia. The development of “smart” matrices for protein and cell delivery may help target regenerative factors for oral engineering of bone and soft tissue.
Many new advances are on the way in regenerative medicine that will affect the practice of dentistry in the near future. Over the past few years, several bone reparative materials have entered the market. One example is a bone replacement graft that displays a biomimetic peptide coating its surface to promote bone regeneration, while enamel matrix-derivative shows growth factor-like activity to stimulate periodontal attachment. Tissue growth factors and new scaffolding materials approved for bone and periodontal repair are in development. Ongoing research using cell therapy for soft tissue grafting is in the clinical trial stage. Various forms of oral cell therapy have been reported in humans for soft tissue grafting in procedures like vestibuloplasty or tooth root coverage. New materials are on the horizon for promoting enamel remineralization and dentin regeneration. In addition, new developments in salivary gland repair may be able to repair damaged salivary glands due to Sjögren’s syndrome or post-radiation therapy.
Tissue-engineered teeth, although at the early stages of development, could eventually replace dental implants. Thus, the fields of tissue engineering and regenerative biology offer many exciting opportunities for clinicians to provide tissue replacement for patients who have lost or damaged oral or dental structures. It may be a decade or two before all of these new advances are accepted by the dental community and become readily adapted to chair-side practice.
From Dimensions of Dental Hygiene. April 2007;5(4): 14-15.

{kind=link}