A Natural Toothbrush
Supporting users of miswak with evidence-based education and recommendations is an important part of providing cross-cultural dental hygiene care.
This course was published in the May 2014 issue and expires May 31, 2017. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the diversity of the United States population.
- Define cross-cultural dental hygiene care.
- Identify the benefits and disadvantages of using miswak.
- Explain how to use miswak.
Today, the US population is more diverse than ever before, with one in eight residents being a foreign-born national.2 Considering these statistics, dental hygienists will encounter cross-cultural patients who may wish to use oral hygiene practices customary to their native countries. For those with origins in Asia, Africa, Latin America, or the Middle East, the use of miswak to clean the teeth and tongue is a customary and common practice.3–5
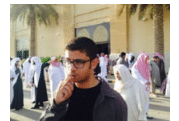
FIGURE 1 COURTESY OF KHALID AYOUB
Miswak is a chewing stick that is used as a natural toothbrush.4 In some parts of the world, particularly in rural areas, miswak is utilized because it is inexpensive, occurs naturally, and is accessible.5–8 Endorsed by several world religions that support its use for religious purposes, miswak is commonly used to clean the mouth before prayer.5,8,9,10 It is not uncommon to see individuals using miswak on the grounds of religious buildings and holy places (Figure 1).
In addition to its cultural relevancy, the practice of miswak is also known as a complementary and alternative medicine (CAM) therapy. Dental hygienists can provide CAM-based oral health instruction and cross-cultural assessments that include the use of the miswak. These concepts underline a more modern approach to dental hygiene practice.
CROSS-CULTURAL DENTAL HYGIENE CARE
Cross-cultural dental hygiene care cannot be achieved by learning how to treat or respond to a particular group. Rather, it involves understanding the complexity and dynamics of culture in the context of oral health care. Culture—or the combined pattern of characteristics, customary beliefs, and behaviors shared by people in a place or time—influences oral health practices. Darby and Walsh state “an individual’s perception of oral health, wellness, and disease are culturally determined.”11 In this way, each cross-cultural dental hygiene encounter presents individuals with unique values and beliefs, who may or may not adhere to their cultural groups’ traditional oral health practices.
A cultural assessment is needed to determine whether an individual is using miswak.1 This assessment should integrate interviewing styles that elicit the patient’s perspective. Responsive communication about health beliefs, practices, and culture can help bring about positive health outcomes. Incorporating these cultural values and beliefs into the dental hygiene assessment and treatment plan is correlated with an individual’s satisfaction with dental hygiene care, compliance, and conflict management.3,4 Culturally competent care in the dental hygiene setting promotes effective patient-provider relationships and the delivery of high-quality care.11,12
Cultural competence is an evolving process that progresses through cultural encounters. It involves adapting best practices for each individual’s behaviors, values, and societal norms.13 Darby and Walsh define cross-cultural dental hygiene practice as “the effective integration of the client’s socio-ethnocultural background into the process of care”—also calling to light that “cross-cultural dental hygiene encompasses the social, political, ethnic, religious, and economic realities that people experience in culturally diverse human interactions and environments.”11
Despite the widespread use of toothbrushes, toothpastes, mouthrinses, and other oral hygiene adjuncts, performing oral hygiene with chewing sticks has been practiced for thousands of years—and continues to be used as an alternative dental hygiene aid. Over the past decade, Americans have become more open to adopting health therapies that vary from traditional approaches. Regardless of the practice used, oral health professionals must understand the body of knowledge available on scientific and cultural constructs as they change within populations.
COMPLEMENTARY AND
ALTERNATIVE MEDICINE
The use of CAM is gaining popularity, with patients in both the US and the world exploring the use of natural products and practices.14–16 The National Center for Complementary and Alternative Medicine defines CAM as “the medical and health care practices, systems, and products that are not included yet in the conventional medicine delivery system and are now in the process of being studied under rigorous scientific inquiry.”17 CAM practices include the use of the following methods: integrated medicine (eg, acupuncture or meditation); natural products derived from herbs, vitamins, minerals, and probiotics; and mind-body practices, such as relaxation techniques, Tai chi, and massage therapy.17 CAM is used by some individuals exclusively or in combination with conventional medicine.
The 2007 National Health Interview Survey Report, conducted by the US Centers for Disease Control and Prevention and the National Center for Health Statistics, is the most recent look at CAM use in the US. This report examined 8.5 million Americans and revealed that 38.8% of adults (age 18 years and older) and 11.8% of children reported using some variation of CAM within 12 months of the survey.15 The World Health Organization’s (WHO) review of global CAM and traditional medicine prevalence found that more than 80% of Ethiopians use traditional medicine, while 70% of Canadians report using one or more natural health products. In Eastern Mediterranean regions, 70% of rural Pakistani populations use CAM and traditional medicine.6 In Europe, 12% of the British population have tried CAM, while the practice is used in Southeast Asia by 70% of rural Indonesians.6 Traditional medicine adopted outside of its indigenous culture is also referred to as CAM.
CAM self-care therapies include the use of herbs, herbal materials, herbal preparations, and finished herbal products that contain parts of plants or other plant materials as active ingredients.18 Because miswak is plant based, it is considered an herbal aid. Cultural competency includes understanding the value of scientific and cultural aspects of all sectors of health-related fields—from herbal remedies to CAM therapies.
MISWAK CHEWING STICKS
Chewing sticks derive from more than 182 plant species that, when manipulated, can be prepared into a toothbrushing stick. Peelu, olive, neem (licorice), and walnut trees produce plant parts conducive to making chewing sticks.16,19 They are widely cultivated and distributed in the dry regions of India, Northern and Central Africa, Asia, the Arabian peninsula, and South America. WHO has cited research to recommend the use of chewing sticks as an economical approach to managing oral disease in developing countries.1,6,8
Miswak is harvested from plant parts of the Salvadora persica or arak tree. Stems, twigs, and roots can be chewed and frayed into a brush that is used to clean the teeth (Figure 2). The arak tree is a large evergreen tree or shrub with soft white or yellowish wood, aromatic roots, and bluish-green leaves. While there are several types of chewing sticks, miswak is often preferred for its pleasant taste, texture, and availability.16,20
S. persica is considered an herbal plant used for medicinal purposes for both oral and systemic conditions. Extracts from the miswak contain biological and botanical properties with antibacterial and antifungal effects.16 Miswak tree ingredients include chemical compounds (with varied potencies) silica, tannic acid, resins, alkaloids (salvadorine), volatile orils (simgrins), sulfur, vitamin C, sodium bicarbonate, potassium chloride and chloride, calcium, benzylisothiocyanate, salicylic acids, sterols, trimethylamine, saponins, and flavonoids.16 When chewed, the miswak releases varying levels of these chemical compounds and essential oils. The chewing stick also has a chemotherapeutic benefit on oral health. Extracts released from S. persica have been shown to reduce bacteria related to the development of dental plaque.10,21–29
Al-Otaibi et al10 demonstrated that miswak reduced plaque microorganisms and concluded that extracts from S. persica might interfere with the growth of Aggregatibacter actinomycetemcomitans—a microorganism involved in the etiology of periodontitis. Almas23 and Elvin-Lewis et al,24 in separate studies, concluded that the antibiotic effects found in S. persica may interfere with plaque bacteria, preventing dental pellicle formation and attachment.
Silica found in miswak acts as a mild abrasive and aids in stain removal.5 Essential oils—including benzyl nitrite, eugenol, thymol, isotheymol, eucalyptol, isoterpinolene, and g-caryophyllene—have antibacterial effects, and their bitter taste stimulates salivary flow.5,22,25,27,28 Vitamins and minerals—such as vitamin C, calcium, and chloride—inhibit calculus formation, prompt healing and soft tissue repair, and incite remineralization of hard dental tissues.5,22,28 The mechanical benefits of properly used miswak include reducing plaque and gingivitis.19,29 Additionally, miswak is used as a cessation tool for smoking and thumb sucking, a teething tool for infants, and a digestive aid.3,25 When used properly, miswak is a helpful oral hygiene aid.
Miswak’s limitations are associated with its natural design. The bristles of the miswak stick lie on the same long axis as its handle. This makes brushing the lingual surfaces of the teeth challenging. Gingival recession has been reported among users who brush excessively with miswak. Lastly, it is difficult to determine the exact amounts of plant ingredients or chemical compounds brushers receive during each use because miswak is naturally occurring. Commercial oral health products sold in the US are dose specific and often formulated to address specific dental health problems, such as xerostomia or recurrent aphthous ulcers.11 When the need for fluoride or other supplemental products is identified, the dental hygienist can recommend, in addition to miswak, the use of dental products with specific dosages or therapeutic properties. This can help ensure individuals receive sustained levels of fluoride or antimicrobials while also incorporating the patient’s cultural values.

HOW TO USE MISWAK
Miswak comes in different diameters and lengths, and users may need to cut the stick to a size that is manageable. A length of 20 cm for adults and 15 cm for children is recommended to ensure proper grip and ease of use. A 1 cm or pencil-sized girth is ideal—sticks should not be too thick as they may be difficult to chew (Figure 3). Also, miswak should not be too thin to prevent breakage under the pressure of brushing.29 Smaller miswak sticks are designed for use as toothpicks.
Once the proper size has been determined, the miswak can be readied for use. To prepare a newly purchased or freshly cut miswak, the tip of the stick should be cut and approximately a half-inch area of bark peeled. The exposed inner core will eventually become a fibrous bristle-like brush.29 The bristled end should be moistened with fresh water. Users gently chew the moistened, bark-free area until bristles separate and soften (typically 15 minutes to 20 minutes). The now-loosened miswak bristles are used to brush the teeth (Figure 4).

FIGURE 4 COURTESY OF CARMELO PADRINO BARRIOS AND OLD DOMINION UNIVERSITY RESEARCH CENTER
Dental hygienists should review miswak use with patients to ensure proper application and angulation for maximum bacterial plaque removal. There are two ways to hold the miswak: a pen grasp using a three-finger grip and a palm grasp with a five-finger grip. Both grasps allow for firm but controlled movements.29 Every effort should be made to access all tooth surfaces. The vertical brushing stroke should be directed away from the gingival margin of the teeth on both the buccal and labial surfaces to avoid gingival trauma and limit the risk of recession.30 A mesial to distal movement removes plaque and food debris from occlusal surfaces.29,30 While bristles do flex and bend into interproximal areas, they do extend far enough to effectively remove subgingival plaque.
Users of miswak should continue to floss for subgingival plaque removal. Individuals may use a combination of both conventional and traditional oral hygiene strategies.29,30 The miswak can also be used to clean the tongue and is believed to help control breath malodor. Miswak sticks may be used up to five times a day for at least 5 minutes per interval. After use, the miswak should be rinsed with clean water. For maintenance, worn brush fibers should be clipped and preparatory directions repeated. A miswak end that is ready for maintenance may exhibit a decrease in flavor intensity.
Miswak is environmentally friendly as it is biodegradable. When purchased in bulk, miswak should be stored in aluminum foil in the freezer. Regularly used miswak should be stored in a plastic travel case. Dental hygienists who understand miswak usage can help patients develop effective technique and ensure proper maintainenance of the sticks. Culturally competent oral health professionals understand how to synthesize culture-specific data within the dental hygiene assessment. This is essential to ensuring positive, culturally informed interactions with patients.9
COMMON MISWAK PRACTICES
Dental hygienists should encourage patients to talk about their oral health practices to facilitate good cross-cultural communication and to demonstrate an understanding of individuals’ cultural perspectives. Specifically, dental hygienists should inquire about home remedies, cultural practices, and alternative or herbal-based oral hygiene aids. Showing a picture of a chewing stick or other culturally-based dental practice is one way to facilitate open communication.
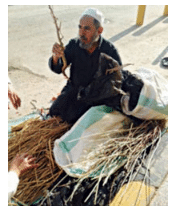
Individuals from different countries may use local names for chewing sticks; for example, miswak is an Arabic term, koyoji is a Japanese word, qesam is the Hebrew name, and datun is a Hindi term. Other common names for chewing sticks are arak, meswak, peelu, siwak, and natural toothbrush tree. Many communities in different regions of the world depend on chewing sticks as their primary oral hygiene aid. Miswak is sold in the US at international grocery stores and can be purchased through the Internet in vacuum-sealed bags to preserve freshness. Locally grown miswak is sold by street vendors. Dental hygienists with patients who use miswak can inquire about habits, provide support, and show understanding of traditional oral hygiene practices.
There are several common miswak habits and practices. Those who use miswak often chew or suck on it for several hours a day,8 keeping it readily available in their pockets or purses or resting it in their mouths. Some individuals may chew on it while performing activities of daily living. Keeping the miswak chewing stick close is convenient and encourages use throughout the day. For some users, however, the habit of keeping it in the mouth leads to holding the miswak in the oral cavity without actually using it. Dental hygienists can ask individuals where the miswak is kept when not in use and remind them to dedicate a time for using the stick.
Oral hygiene instructions should include choosing freshly cut or sold miswak because it is supple, easily chewed, and full of natural ingredients. A fresh miswak root should be a whitish-brown color; dark-brown coloring may indicate the miswak is no longer fresh. A dried out miswak can be abrasive to both hard and soft dental tissues. Although moistening the miswak before use is important, dental hygienists should remind individuals that soaking the stick for long time periods may dilute active ingredients and minimize therapeutic benefits.
It is the role of oral health professionals to discuss which hygiene habits benefit daily regimens and which need to be targeted for change. The dental hygiene human needs assessment model should include culturally relevant goals. These may include the use of culturally specific or alternative oral hygiene aids and practices used exclusively or in conjunction with mainstream dental hygiene products. Cultural beliefs and practices that do not cause harm should not be targeted for amendment, and dental hygienists should allow time for such change when advising patients on how to eliminate potentially harmful or ineffective habits or practices.11
CONCLUSION
Cultural awareness is an important component of embracing cultural competency in dental hygiene care.11,12 Understanding miswak brings awareness to a traditional oral hygiene aid used for centuries by many diverse populations in the US and abroad. Dental hygienists can apply knowledge of traditional oral hygiene regimens while practicing in the US, or when volunteering with international organizations around the world, in regions where miswak might be locally grown, sold, and/or used.
CAM practices are gaining in popularity in the US, driven by an ethnically diverse population that is eager to embrace natural remedies for self-care. While more research is needed to fully determine the oral health benefits of miswak, dental hygienists can support its use with instruction on correct application and technique. The value of the miswak chewing stick is both chemotherapeutic and mechanical. Understanding its benefits and limitations ensures safety and efficacy of culturally based dental hygiene therapies.31
Social and cultural norms are not only shared by groups but are also passed on between generations. The use of a toothbrush in addition to miswak is also effective and common among some ethnic subgroups, and dental hygienists are encouraged to recommend supplemental oral hygiene products as needed.
Reviewing common health care practices and inherent beliefs in an individual’s culture gives the dental hygienist an opportunity to provide culturally competent care. A positive cultural encounter can help establish trusting patient-provider relationships.11
REFERENCES
- Asad i SG, Asadi ZG. Chewing sticks and the oral hygiene habits of the adult Pakistani population. Int Dent J. 1997;47:275–278.
- United States Census Bureau. Place of Birth of the Foreign-Born Population: 2009. Available at: census.gov/prod/2010pubs/ acsbr09-15.pdf. Accessed April 17, 2014.
- Al Sadhan R, Almas K. Miswak (chewing stick): a cultural and scientific heritage. Saudi Dental Journal.1999;11(2):80–88.
- Wu C, Darout I, Skaug N. Chewing sticks: timeless natural toothbrushes for oral cleansing. J Periodontal Res. 2001;36:275–284.
- Sukkarwalla A, Ali SM, Lundberg P, Tanwir F. Efficacy of miswak on oral pathogens. Dent Res J (Isfahan). 2013;10:314–320.
- World Health Organization. Legal Status of Traditional Medicine and Complementary/Alternative Medicine: A Worldwide Review. Available at: apps.who.int/medicinedocs/pdf/h2943e/h2943e.pdf. Accessed April 17, 2014.
- Hattab FN. Miswak: the natural toothbrush. J Clin Dent.1997;8:125-129.
- Enwonuu C, Anyanwu R. The chewing stick in oral health care. World Health Forum.1985;6:232–234.
- Tubaishat RS, Darby ML, Bauman Db, Box CE. Use of miswak versus toothbrushes: oral health beliefs and behaviours among a sample of Jordanian adults. Int J Dent Hyg. 2005;3:126–136.
- Al-Otaibi M, Al-Harthy M, Gustafsson A, Johansson A, Claesson R, Angmar-Mansson B. Subgingival plaque microbiota in Saudi Arabians after use of miswak chewing stick and toothbrush. J Clin Periodontal. 2004;31:1048–1053.
- Darby M, Walsh M. Dental Hygiene Theory and Practice. 3rd ed. Philadelphia: WB Saunders Co; 2010:56–70.
- Fitch P. Cultural competence and dental hygiene care delivery: integrating cultural care into the dental hygiene process of care. J Dent Hyg. 2004;78:11–21.
- Campinha-Bacote J. The process of cultural competence in the delivery of healthcare services: a model of care. J Transcult Nurs. 2002;13:181–184.
- Pérez MA, Luquis RR. Cultural Competence in Health Education and Health Promotion. 1st ed. San Francisco: Joss-Bass A Wiley Imprint; 2008:8–79.
- Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;12:1–23.
- Mohamed SA, Khan JA. Antioxidant capacity of chewing stick miswak Salvadora persica. BMC Complement Altern Med. 2013:13:40.
- National Center for Complementary and Alternative Medicine. Complementary, Alternative, or Integrative Health: What’s in a Name? Available at: nccam.nih.gov/health/ whatiscam. Accessed on April 17, 2014.
- Singh A., Purohit B. Toothbrushing, oil pulling and tissue regeneration: a review of holistic approaches to oral health. J Ayurveda Integr Med. 2011;2:64–68.
- Chaurasia A, Patil R, Nagar A. Miswak in oral cavity—an update. Journal of Oral Biology and Craniofacial Research. 2013;3(2):98–101.
- Elvin-Lewis M. The therapeutic potential of plants used in dental folk medicine. Odontostomaol Trop. 1982;5:107–117.
- Sher H, Al-yemni MN, Wijaya L. Ethnobotanical and antibacterial potential of Salvadora persica: a well know medical plan in Arab and Urani system of medicine. Journal of Medical Plants Research. 2011;5(7):1224–1229.
- Norton M, Addy M. Chewing sticks versus tooth brushes in West Africa. A pilot study. Clin Prev Dent. 1989;11:11–13.
- Almas K. The antimicrobial effects of extracts of Azadirachta indica (Neem) and Salvadora persica (Arak) chewing sticks. Indian J Dent Res.1999;10:23–26.
- Elvin-Lewis M, Hall JB, Adu-Tuto M, Afful Y, Asante-Appiah K, Lieberman D. The dental health of chewing stick users of southern Ghana. Preliminary findings. J Prev Dent. 1980:6:151–159.
- Almas K, Al-Zeid Z. The immediate antimicrobial effect of a toothbrush and Miswak on cariogenic bacteria: A clinical study. J Contemp Dent Pract. 2004;5:105–114.
- Darout IA, Albandar JM, Skaug N, Ali RW. Salivary microbiota levels in relation to periodontal status, experience of caries and Miswak use in Sudanese adults. J Clin Periodontol. 2002;29:411–420.
- Noumi E, Snoussi M, Trabelsi N, et al. Antibacterial, anti candida and antioxidant activities of Salvadora persica and Jaglans regia L extracts. Journal of Medical Plants Research. 2011;5(17):4138–4146.
- Baeshen HA, Kjellberg H, Lingstrom P, Birkhed D. Uptake and release of fluoride from fluoride-impregnanted chewing sticks (miswaks) in vitro and in vivo. Caries Res. 2008;42:363–368.
- Akhtar M, Ajmal M. Significance of chewing sticks (miswaks) in oral hygiene from a pharmacological view-point. J Pak Med Assoc. 1981;4:89–95.
- Almas K, al-Lafi TR. The natural toothbrush. World Health Forum. 1995;16:206–210.
- Almas K, Skaug N, Ahmad I. An in vitro antimicrobial comparison of miswak extract with commercially available non-alcohol mouth rinses. Int J Dent Hyg. 2005;3:18–24.
From Dimensions of Dental Hygiene. May 2014;12(5):56,59–62.
