 CYLONPHOTO / ISTOCK / THINKSTOCK
CYLONPHOTO / ISTOCK / THINKSTOCK
3D Printing in Dentistry
This promising technology has many uses in the delivery of oral health care services—from restorative care to implant dentistry.
This course was published in the July 2016 issue and expires July 31, 2019. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the process of three-dimensional (3D) printing within the field of dentistry.
- Identify the advantages and disadvantages of 3D printing when compared with conventional techniques.
- Discuss the incorporation of 3D printing technology into various dental procedures such as orthognathic surgeries, oral and maxillofacial procedures, surgical guide fabrication for implants, and the design of certain prosthetics.
Technological advances have allowed oral health professionals to provide more accurate treatment in a timely and effective manner. The integration of digital impressions and computer-aided design/computer-aided manufacturing (CAD/CAM) are examples of how technology has revolutionized treatment approaches. The evolution of new modalities—including three-dimensional (3D) printing—has broadened the scope of dental practice. It has also benefited lab fabrication by creating a 3D final product via an additive process. Among other indications, 3D printing and CAD/CAM technologies enable the precise fabrication of aligners, removable prosthodontics, and surgical templates for implants.1 Dental hygienists need to understand evolving technology within the dental field. 3D printing can lead to the fabrication of more precise fitting dental products after an impression is taken by a dental hygienist.
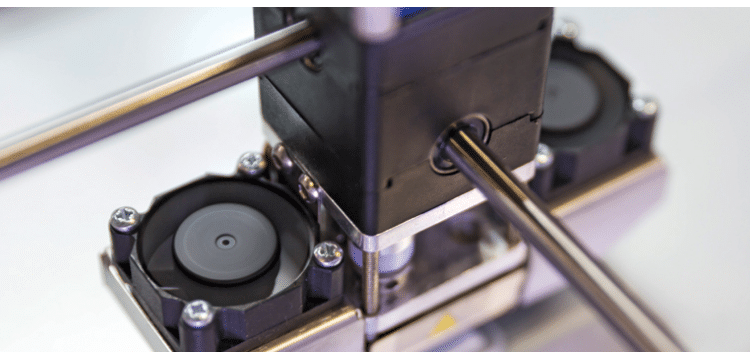
The use of 3D printing also has applications for oral and maxillofacial treatment, as well as orthognathic surgeries (Figure 1). It can be used to produce models for treatment planning, preoperative positioning of the jaws, fabrication of splints, and similar indications.2 Moreover, 3D printing is compatible with digital software and digital files obtained during magnetic resonance imaging.3 The future is encouraging for the fabrication of crowns, bridges, inlays, onlays, and dentures using 3D printing, but further research is needed to demonstrate the durability of the final product in the oral environment.
The 3D printing process starts by creating a virtual image of an object to be produced. This requires CAD software that transforms the information into a digital file. If the goal is to replicate an existing object, a 3D scanner provides the digitized information. In the creation of an entirely new object, a 3D modeling program produces the virtual design for the printer to follow.4
In the case of objects to be replicated, obtaining the image is similar to the process used with the milling technique, but the production processes used in milling and 3D printing are distinct. Milling is subtractive, namely the final product is carved from an existing block of material. The 3D printing process is additive meaning that the final product is created (ie, printed) in layers.1
METHODS AND PROCESSES
Within the delivery of oral health care, multiple methods exist for rapid prototyping, such as stereolithography (SLA) or optical fabrication, inkjet-based systems, selective laser sintering (SLS), and fused deposition modeling (FDM).5 Each of these technologies is used to create 3D dental items, yet each offers certain advantages for particular types. SLA is widely utilized for reconstructive surgeries and for producing surgical templates for implants. SLS is effective for producing removable partial denture frameworks, while the FDM method assists in the production of direct wax-ups for dental restorations.5
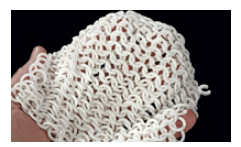
SLA and inkjet-based printing are the most commonly used technologies. Once the digital image is obtained, both SLA and inkjet-based printing use 3D modeling software that sections the final image into horizontal layers, and then prints these in increments to create the final product.4 In the SLA process, the layers are laser cured and, following fabrication (Figure 2), the entire model must be cured. Compared with inkjet-based systems, SLA technology is intended to produce larger objects, but is more cumbersome and may be less cost-effective.6
The inkjet-based technique involves light-based curing of a liquid polymer layer by layer. A gel-like material provides support during the production process.6 The gel is then easily dissolved away in water after the process is finished. Once created, the items can be used immediately without having to wait for a final cure. Production via the inkjet-based technique provides a quick and easy means to precisley fabricate smaller objects.6
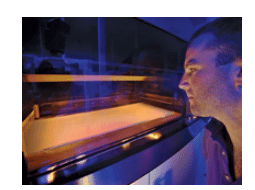
The SLS method produces a prototype via a layer-by-layer deposition of a specific powder on a building cylinder (Figure 3). The layers are fused together via a computer-operated laser. The laser facilitates optimal melting of the powder, thus ensuring effective bonding through sintering of subsequent layers. The process produces intact 3D dental prototypes.5 Moreover, SLS can effectively use a wide variety of materials, such as nylon, thermoplastic composites, metals, casting waxes and ceramics. For example, SLS technology has successfully produced cobalt chromium removable partial denture frameworks.5
JAMES KING-HOLMES / SCIENCE SOURCE IMAGES
By comparison, FDM technology produces a prototype via a layer-by-layer deposition of a thermoplastic polymer material. The material is held into a nozzle apparatus, where it is transformed into a semi-liquid state and ejected onto the building base. The nozzle is temperature controlled and the motion is computer operated, resulting in accurate deposition of the warmed polymer. The semi-liquid thermoplastic material becomes solid within 0.1 second and bonds to the previous layer. The process continues until the object is produced. The fabrication process occurs in a chamber in which the temperature is preset just below the melting temperature of the thermoplastic material. This process is used for making wax-ups and can produce up to 150 items per hour.5
DENTAL IMPLICATIONS
3D printing can be helpful for a variety of treatments. Orthognathic surgeries can be enhanced through the use of 3D printing. This is accomplished by performing a radiographic analysis, followed by a transfer of mandibular movements to the models. Surgical simulation is performed on the dental models to create the desired post-operative occlusion.7 Based on this preoperative analysis, an acrylic surgical wafer is fabricated using 3D printing and used during surgery as an acrylic-based interocclusal splint that helps develop optimal occlusion.7
Conventional orthognathic surgeries require alginate impressions of the arches, obtaining a facebow record, and articulating the casts onto an adjustable articulator. The dental models are manually positioned into the final post-operative occlusion, and the surgical wafers are produced. The process can be cumbersome, time consuming, and error-prone.7 Cousley and Turner7 compared conventional fabrication methods for orthognathic surgical wafers with 3D printing. Alginate impressions were obtained for both arches and dental stone models were prepared. A 3D scanner produced digital images of the models, which were used to print the wafer used in developing final post-operative occlusion.7 The authors concluded that, compared with the conventional technique, 3D printing eliminated steps—including facebow recording and transfer to the articulator—that could alter the accuracy of the surgical wafer.7
This technology has also been used in mandibular reconstruction procedures. Cohen et al6 reported three clinical cases of mandibular reconstruction, including partial mandibulectomies performed in ameloblastoma cases. Using 3D printing as part of oral and maxillofacial surgical procedures provides the opportunity to perform a preoperative finishing of the final mandibular reconstruction. It also allows surgeons to view 3D models and determine the essential preoperative steps to obtain more precise results.6
Orthognathic surgeries require a model surgery prior to the actual procedure, and the effectiveness of 3D printing and digital model surgery has been evaluated clinically. Model surgery provides a view of the post-operative jaw movement in three dimensions.8 Traditionally, this is accomplished with a manual model technique that can potentially lead to inaccuracies due to manual errors. Kim et al8 found that these inaccuracies could be minimized through digital modeling and 3D printing technologies. Comparing the accuracy of manual and digital model surgery, the study showed that interocclusal wafers fabricated through the digital printing process were more accurate than those fabricated using manual methods.8
Traditional orthognathic surgeries are planned using plaster study models. Such conventional methods have limitations, such as a lack control over movements of the cranium during the preoperative surgery performed on the plaster study model.9 Advances in digital technology have facilitated a combined approach incorporating traditional and digital methods with improved post-operative results.9 The use of cone-beam computed tomography (CBCT) integrated with 3D modeling software can facilitate the manipulation of the boney details into presurgical treatment planning.9 Metzger et al9 reported the use of such combined technique on a patient with Class 3 malocclusion. The study suggests that even though digital techniques improve certain aspects of orthognathic surgical treatment planning, the value of manual manipulation should not be ignored.
SURGICAL TEMPLATES
CAD technology and 3D printing are also used to create surgical templates for implants.10 Fuster-Torres et al10 found that a CAD/CAM system, along with stereolithographic rapid prototyping, produced a surgical template that facilitated more accurate implant placement.
In 2014, Vidal and Vidal11 described a new method that incorporated digital scanners, 3D printing, and CBCT to perform implant planning in a completely digital environment. The method involved taking intraoral and extraoral images to evaluate for esthetic considerations. The smile line, tooth position, and gingival margins were evaluated and marked digitally. Study models were scanned with a 3D scanner, creating a virtual wax-up, and the desired position of the implant-based restoration was determined. Next, a tomographic implant guide was produced using specialized software and 3D printing. The guide was subsequently positioned while CBCT images were obtained and used in a mock surgery to determine final implant placement and position.11
The actual surgical guide was modeled and printed when the CBCT image of the tomographic guide and digital wax-up were integrated and confirmed to be a viable implant placement plan. The study showed that the implants were accurately placed, as per the presurgical implant planning conducted through the combined use of CBCT, scanning, and 3D printing. The implants healed appropriately and and were later restored. This combined use of technological advances was reported to be more precise than conventional methods of manual wax-up and fabrication of surgical templates.11
Schneider et al12 conducted a literature review to examine the accuracy and clinical application of computer-guided, template-based implant dentistry. The review found that six clinical trials demonstrated a survival rate of 91% to 100% after an observation period of
12 months to 60 months for implants placed through the computer-based systems.12 Ghiuta et al13 studied the efficacy of using a CAD/CAM system along with stereolithographic printing for the fabrication of implant surgical templates, and the subsequent functional loading of the implant. The results indicated that the implants were placed without complications. The surgery was flapless and the post-operative examination showed no signs of pain, bleeding, or swelling.13
FABRICATING RESTORATIONS
When fabricating restorations, CAD/CAM milling systems provide a number of advantages to clinicians and patients, including precision and, in the case of in-office milling systems, same-day restorations. But there are also disadvantages. Milling the restoration from a ceramic block wastes some of the raw material. In addition, exposure to tooling during manufacturing raises the risk of microscopic cracks forming in ceramic surfaces. These shortcomings could be minimized or even eliminated with 3D printing.14
Elbert et al14 examined the effectiveness of direct inkjet 3D printers in producing zirconia-based dental prostheses. The study used a ceramic suspension composed of zirconia powder, distilled water, boehmite sol, and dispersants. The results indicated that it is possible to produce components of the size and shape and with the occlusal features of a crown through this process.14 While the printed components showed some microscopic cracks, the density of the printed components was estimated at 96.9%—enough to provide the strength and physical properties essential to withstand oral function despite the microscopic cracks.14
Another study described the technique of producing core and fixed partial denture frameworks and robocasting of crown structures using a process in which ceramic materials are built up layer by layer in an additive method.15 The study described two methods of robocasting. One used a process in which the core is printed from zirconia-based ink via a stereolithography file. The second method is a fugitive process in which carbon black is codeposited with the ceramic material. The carbon black is removed during the sintering process.15
Hussein and Hussein3 reported on the fabrication of a removable partial denture framework for a mandibular Kennedy Class 1 arch using a study cast made from a silicone-based impression material. A digital file of the cast was made using a 3D scanner, and the removable partial denture framework was created using software to design the components, such as connectors and clasps. The 3D model was printed in a layer-by-layer process using polymer powder and a CO2 laser. The authors concluded that the final framework exhibited optimal adaptation to the original cast. In addition, production costs were comparable to conventional methods, but printed fabrication proved more efficient.3
Bibb et al16 assessed the effectiveness of a method that combined CAD and 3D printing via selective laser melting. The study utilized a 3D scan of a partially edentulous patient cast, which allowed digital design of the removable partial denture’s component parts.16 One framework was fabricated via selective laser melting from stainless steel, and a second was produced using cobalt chromium alloy, thus providing two frameworks for comparative purposes. Compared with the stainless steel framework, the cobalt chromium alloy framework proved more efficient. Both exhibited accurate fit on the patient cast, but the retentive components of the stainless steel framework showed deformation after repeated insertion and removal.16 In addition to showing no signs of deformation, the cobalt chromium framework fit well on the cast and also in the patient, who reported no signs of discomfort. Compared with manual investment and casting procedures and in terms of decreased preparation time and reduced likelihood of errors, this research supports the viability of using 3D printing to produce removable partial denture frameworks.16
CONCLUSION
While 3D printing is becoming more popular, its full potential for oral health care delivery remains unknown. One area that shows promise, for example, is its use in producing crowns, bridges, and complete dentures. Although precise fit appears to be a major advantage, the human tactile sense may still be needed to produce ideal restorations. More extensive studies of 3D printing and associated technology are required to prove the efficiency and effectiveness of these modalities for restorative and other dental procedures.
Clinicians need to stay abreast of advances that have the potential to benefit both practitioners and patients. In this regard, 3D printing represents a promising technology that could bring an array of advanced treatment methods that can improve oral health outcomes.
References
- Bunek SS, Brown C, Yakas ME. The evolving impressions of digital dentistry. Available at: https://cdeworld.com/courses/4733-The_Evolving_Impressions_of_Digital_Dentistry. Accessed June 10, 2016.
- Yun Young P. The application of three-dimensional printing techniques in the field of oral and maxillofacial surgery. J Korean Assoc Oral Maxillofac Surg. 2015;41:169–170.
- Hussein MO, Hussein LA. Novel 3D modeling technique of removable partial denture framework manufactured by 3D printing technology. Int J Adv Res. 2014;9:686–694.
- 3dprinting.com. What is 3D printing? Available at: 3dprinting.com/what-is-3d-printing/#whatitis. Accessed June 10, 2016.
- Azari A, Nikzad S. The evolution of rapid prototyping in dentistry. Rapid Prototyping J. 2009;15:216–225.
- Cohen A, Laviv A, Berman P, Nashaf R, Abu Tair J. Mandibular reconstruction using stereolithographic3-dimensional printing modeling technology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:661–666.
- Cousley R, Turner M. Digital model planning and computerized fabrication of orthognathic surgery wafers. J Orthod. 2014;41:38–45.
- Kim BC, Lee CE, Park W, et al. Clinical experiences of digital model surgery and the rapid prototyped wafer for maxillary orthognathic surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111:278–285.
- Metzger MC, Majert Hohlweg B, Schwarz U, Teschner M, Hammer B, Schmelzeisen R. Manufacturing splints for orthognathic surgery using a three dimensional printer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:e1–e7.
- Fuster-Torres MA, Albalat-Estela S, Alcaniz-Raya M, Penarrocha-Diago M. CAD/CAM dental systems in implant dentistry: Update. Med Oral Patol Oral Cir Bucal. 2009;14:E141–E145.
- Vidal F, Vidal R. Development of a novel protocol for digital implant planning using cone beam CTs, scanners and 3D printers: the full digital implant planning protocol. Clin Oral Implants Res. 2014;25(Suppl):175.
- Schneider D, Marquardt P, Zwahlen M, Jung RE.A systematic review on the accuracy and the clinical outcome of computer guided template-based implant dentistry. Clin Oral Implants Res. 2009;20(Suppl):73–86.
- Ghiuta C, Cristache CM, Mihai A, et al. Predictable computer guided flapless surgery for dental implants insertion. AMT. 2015;20(2):119–122.
- Ebert J, Ozkol E, Zeichner A, et al. Direct inkjet printing of dental prostheses made of zirconia. J Dent Res. 2009;88:673–676.
- Silva NRFA, Witek L, Coelho PG, Thompson VP, Rekow ED, Smay J. Additive CAD/CAM process for dental prostheses. J Prosthodont. 2011;20:93–96.
- Bibb R, Eggbeer D, Williams R. Rapid manufacture of removable partial denture frameworks. Rapid Prototyping J. 2006;12:95–99
From Dimensions of Dental Hygiene. July 2016;14(07):48–51.
