
The Hidden Sleep Disorder Linked to Oral and Systemic Health
Oral health professionals are uniquely positioned to detect pediatric obstructive sleep apnea early and help change a child’s lifelong health trajectory.
This course was published in the May/June 2026 issue and expires June 2029. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 430
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define obstructive sleep apnea (OSA) and pediatric obstructive sleep apnea (POSA) and understand complications of untreated POSA.
- Discuss risk factors, signs and symptoms, and possible treatments of POSA.
- Identify the role of dental hygienists in early detection of and treatment referral for POSA.
Pediatric obstructive sleep apnea (POSA) occurs in 1% to 6% of children, making it a significant public health concern.1 POSA can be linked to a variety of developmental delays and chronic health issues, including cardiovascular concerns and overall failure to thrive. Additionally, POSA can lead to problems with skeletal, jaw, and dentition development.2 POSA also may contribute to neurocognitive and emotional developmental delays, including attention-deficit/hyperactivity disorder (ADHD).
Because early detection of POSA and related conditions can significantly improve oral and general health outcomes in children, oral health professionals should screen for signs and symptoms of POSA during routine exams.3
Obstructive sleep apnea (OSA) is a partial or complete airway obstruction during sleep that interrupts normal sleep patterns and nighttime breathing. This includes episodes of intermittent hypoxia (lack of oxygen) and frequent sleep arousal.2 OSA usually occurs when the pharyngeal airway soft tissue relaxes during sleep. When an individual inhales, the airway can be partially or completely obstructed, thereby inhibiting oxygen flow. OSA is the most common type of sleep-disordered breathing in children.4
A major complication of untreated POSA is strain on the heart and vascular system, which can increase the risk of chronic cardiovascular disease. Episodes of apnea (breathing pauses) can trigger intermittent hypoxia (a drop in blood oxygen levels). That drop in oxygen levels activates the sympathetic nervous system, increasing heart rate and blood pressure. Repeated episodes over time can lead to cardiac remodeling. These effects are more pronounced in children who are obese or have elevated blood pressure.1,5,6
Another complication of POSA is its impact on physical growth and development. Children with POSA may experience poor weight gain, growth delays, and failure to thrive. Cognitive, learning, and behavior issues can also be linked to untreated POSA. The lack of oxygen resulting from apnea can significantly affect neurocognitive development, attention deficits, memory, and academic performance. Unsurprisingly, these complications of POSA may inhibit a child’s ability to learn and function well in school, causing behavioral difficulties, irritability, and social issues.2
POSA in children may also affect craniofacial development. Children with POSA may have differences in their dental arch dimensions when compared with healthy children. These include narrower maxilla, deeper palatal height, receding mandible (deficient chin), crossbites, overjets, and dental malposition. These alterations are believed to result from chronic postural adaptations of the head, jaw, and tongue aimed at maintaining an open airway during sleep.7 These abnormalities can affect dental crowding, breathing patterns, bite, and facial structure. Additionally, chronic mouth breathing can lead to xerostomia, increasing the risk of dental caries and periodontal diseases.8
Causes and Risk Factors
The leading cause of OSA in children is thought to be adenotonsillar hypertrophy, or enlarged tonsils and/or adenoids. This enlargement can narrow the upper airway, especially during sleep, leading to airflow obstruction.9 This correlates with the fact that peak prevalence of childhood OSA occurs between the ages of 2 and 5, when the size of even a healthy child’s adenoids and tonsils are large relative to their developing airway size.10
Obesity in young children also can be an important risk factor for POSA, leading to fat deposits in the neck and throat that narrow the upper airway, making it more prone to collapse during sleep. This fat deposition also reduces the effectiveness of muscles that help keep the airway open.11 However, unlike in adults, obesity in children is not the most significant risk factor for POSA.10,11
Neuromuscular and functional risk factors for POSA include weakness in the muscles of the upper airways, impaired upper airway reflexes during sleep, abnormal central arousal mechanisms, and weak protective airway responses. These conditions reduce airflow and can cause apneas and/or hypoxia during sleep. These symptoms may appear in isolation or may occur with neuromuscular diseases such as spinal muscular atrophy, muscular dystrophy, and congenital myopathies.12
Craniofacial abnormalities, such as retrognathia (small or recessed jaw) and/or high-arched or narrow palate, can be risk factors for POSA because they physically restrict the upper airway. As a smaller or constricted airway is more prone to collapse during sleep, this can lead to the breathing interruptions. Nasal obstructions (allergic rhinitis, deviated septum) also play a role in POSA for the same reasons. These craniofacial and nasal factors may be congenital, developmental, or secondary to chronic mouth breathing. All of these can contribute to a constricted airway.2,13
Other factors to consider when evaluating potential for POSA are exposure to allergens and second-hand smoke, which can contribute to nasal inflammation. Additionally, POSA more frequently occurs in boys, children between the ages of 2 and 8, and those with a family history of sleep apnea.10
Signs and Symptoms
Most children with OSA experience symptoms that include snoring and difficulty breathing during sleep. Because it can be challenging to differentiate OSA from snoring, parents should be on the lookout for symptoms including restless sleep, night sweats, bedwetting, and morning headaches.10
 Some children with OSA may also exhibit signs of daytime sleepiness, although this is less commonly reported in children than in adults. Children may also exhibit behavior issues similar to ADHD, as well as loss of appetite, learning difficulties, aggressive behavior, and poor academic performance.9,10 Additional physical signs and symptoms of POSA include recessed or retrognathic jaw and receding chin, and forward head posture, as well as dark undereye circles and an overall look of fatigue compared with healthy children.10
Some children with OSA may also exhibit signs of daytime sleepiness, although this is less commonly reported in children than in adults. Children may also exhibit behavior issues similar to ADHD, as well as loss of appetite, learning difficulties, aggressive behavior, and poor academic performance.9,10 Additional physical signs and symptoms of POSA include recessed or retrognathic jaw and receding chin, and forward head posture, as well as dark undereye circles and an overall look of fatigue compared with healthy children.10
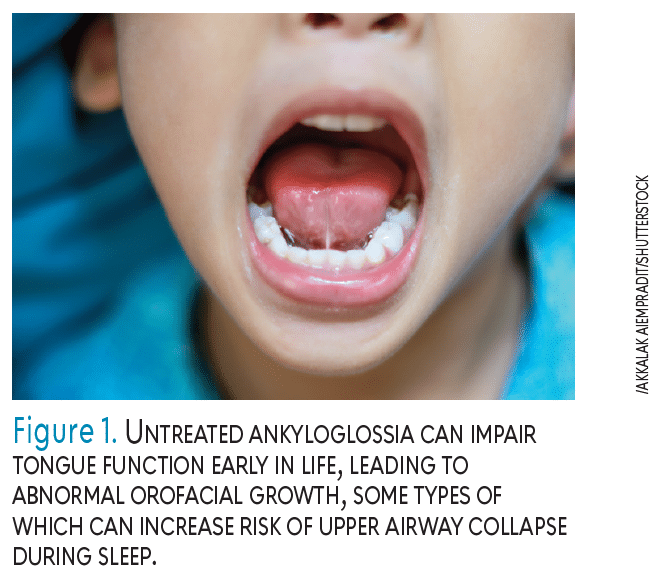
POSA exhibits many physical signs, such as enlarged tonsils, bruxism, and signs of tooth wear such as abrasion, attrition, erosion, and abfraction. Duran-Cantolla et al14 found a statistically significant association between apnea episode frequency and tooth wear severity. Additional symptoms within the mouth include high arched or narrow palate, enlarged tongue, and ankyloglossia (tongue ties) or untreated short lingual frenum. Untreated ankyloglossia can impair tongue function early in life, leading to abnormal orofacial growth, some types of which can increase risk of upper airway collapse during sleep (Figure 1).15
Diagnosis and Treatment
POSA can only be diagnosed by a qualified physician before beginning any treatment. Therefore, patients experiencing symptoms of OSA should seek diagnosis by a physician, preferably one specializing in sleep disorders. They use specific techniques including endoscopy, laryngoscopy, and pharyngometry, and computed tomography or magnetic resonance imaging to evaluate airway narrowing or other structural concerns.10
Polysomnography (PSG) is considered the gold standard for diagnosing OSA.10 This is usually done in a clinical setting where the patient is monitored to measure sleep patterns, breathing, and oxygen levels. The PSG will provide an apnea-hypopnea index (AHI), which represents the number of apneas and hypopneas divided by the hours the individual sleeps. While a minimum of five apneas is considered evidence of OSA in adults, children can be diagnosed with an AHI of greater than one and less than five.10
The right treatment plan depends on individual risk factors and symptoms, but the most common approaches are surgery, positive airway pressure (PAP) therapies, myofunctional therapy (MFT), and orthodontic treatments. For most children, treatment for POSA includes a procedure to remove enlarged adenoids and tonsils via adenotonsillectomy. Although this is the first line of treatment, surgical therapy sometimes fails to provide a long-term solution.10
Used to improve air flow and reduce nighttime apneas, PAP therapies generally are effective for adults, but present challenges when used to treat children.16 The use of PAP therapy masks in children can potentially affect midfacial growth and cause maxillary retrognathia over time.17 Other concerns include mask fit, anxiety, and embarrassment. Questions surrounding whether pediatric patients will use the therapy consistently and whether children who use continuous PAP therapy will need it indefinitely create uncertainty as to its long-term effectiveness.18
 MFT, used to strengthen muscles and improve tongue and facial muscle function, increases patient proprioception (body awareness) and improves airway health. Myofunctional therapists help patients use exercises to improve nasal breathing, lip tone, and lip seal. They may also recommend a lingual frenectomy. According to Bandyopadhyay et al,19 studies show that MFT decreased AHI by 43% in children and increased oxygen saturations in children with mild to moderate OSA. As with other therapies, MFT’s effectiveness relies on the patient’s ability to consistently follow directions for completing exercises. Compliance can be an issue with MFT in children and therefore requires continuous parental involvement to increase effectiveness.15
MFT, used to strengthen muscles and improve tongue and facial muscle function, increases patient proprioception (body awareness) and improves airway health. Myofunctional therapists help patients use exercises to improve nasal breathing, lip tone, and lip seal. They may also recommend a lingual frenectomy. According to Bandyopadhyay et al,19 studies show that MFT decreased AHI by 43% in children and increased oxygen saturations in children with mild to moderate OSA. As with other therapies, MFT’s effectiveness relies on the patient’s ability to consistently follow directions for completing exercises. Compliance can be an issue with MFT in children and therefore requires continuous parental involvement to increase effectiveness.15
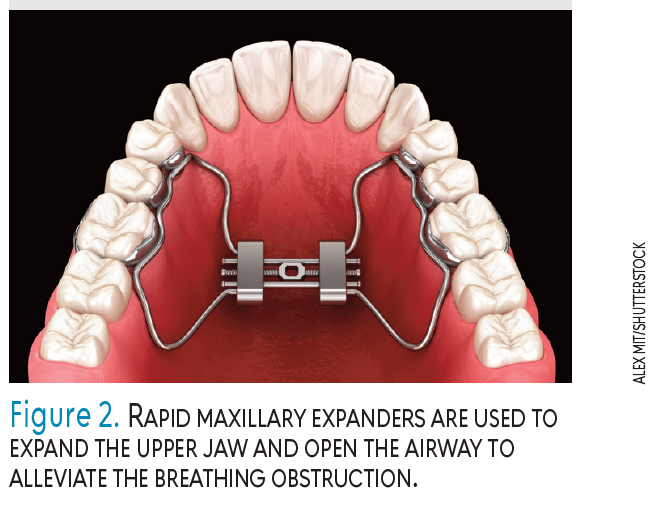
Orthodontic treatments are used to expand the upper and/or lower jaw to create room for the tongue and open the airway. Rapid maxillary expansion (RME) is used to expand the upper jaw and open the airway to alleviate the breathing obstruction (Figure 2). Studies show that RME can be effective beyond 2 years following treatment, and when combined with adenotonsillectomy, RME resolves POSA in most children.10
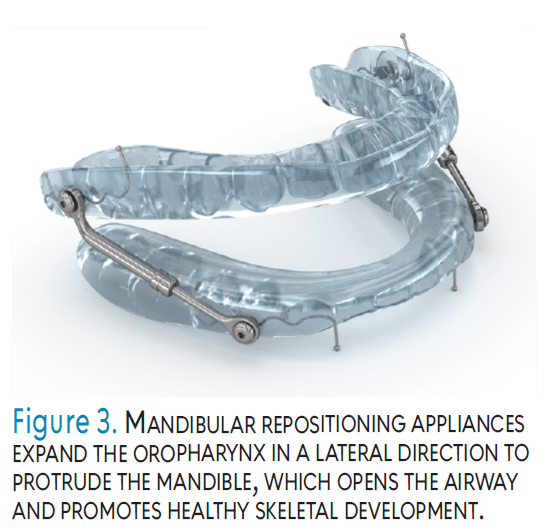
Mandibular repositioning appliances (MRAs) expand the oropharynx in a lateral direction to protrude the mandible, which opens the airway and promotes healthy skeletal development (Figure 3). MRAs are more often used in adults and limited evidence is available to suggest their effectiveness in children.10 Children and adults with oral appliances of any kind should have regular and thorough dental examinations, periodontal examinations, and temporomandibular joint evaluations to ensure optimal tooth alignment, periodontal health, and proper joint function.10
Tobacco smoke, allergens, and pollutants that irritate the airway and contribute to congestion should be avoided. Though obesity is more commonly associated with OSA in adults, an unhealthy weight can also be a contributing factor in children and teenagers experiencing OSA.20
Oral health professionals are uniquely situated to help detect early signs of POSA and identify patients who may benefit from seeing a sleep specialist. Oral health professionals may see children more frequently than physicians. In addition, their specialized oral health expertise can help them spot abnormalities that general practitioners may overlook.3,10
Interprofessional practice is important to treating the whole patient. By screening for POSA and collaborating with other healthcare providers, oral health professionals can improve long-term health outcomes for children.21 For this reason, the American Academy of Pediatric Dentistry recommends children be screened for sleep disorders at the first dental visit.8
The Ask, Look, Refer Method
When clinicians are educated about the signs of sleep disorders, they can efficiently identify potential concerns by adding a simple three-step process to the already existing clinical assessment. We propose the ask, look, refer (ALR) method to support the accurate detection of POSA.
 Ask. A thorough health history that includes common POSA symptoms can help providers assess the potential need for referral. Dental hygienists can ask parents/caregivers about specific daytime symptoms, including sleepiness, mouth breathing, and behavior problems, as well as nighttime symptoms such as snoring, gasping for air, grinding teeth, and bedwetting.8 A sleep questionnaire or screening form can help parents/caregivers and providers spot signs of disordered sleep they may not otherwise notice.
Ask. A thorough health history that includes common POSA symptoms can help providers assess the potential need for referral. Dental hygienists can ask parents/caregivers about specific daytime symptoms, including sleepiness, mouth breathing, and behavior problems, as well as nighttime symptoms such as snoring, gasping for air, grinding teeth, and bedwetting.8 A sleep questionnaire or screening form can help parents/caregivers and providers spot signs of disordered sleep they may not otherwise notice.
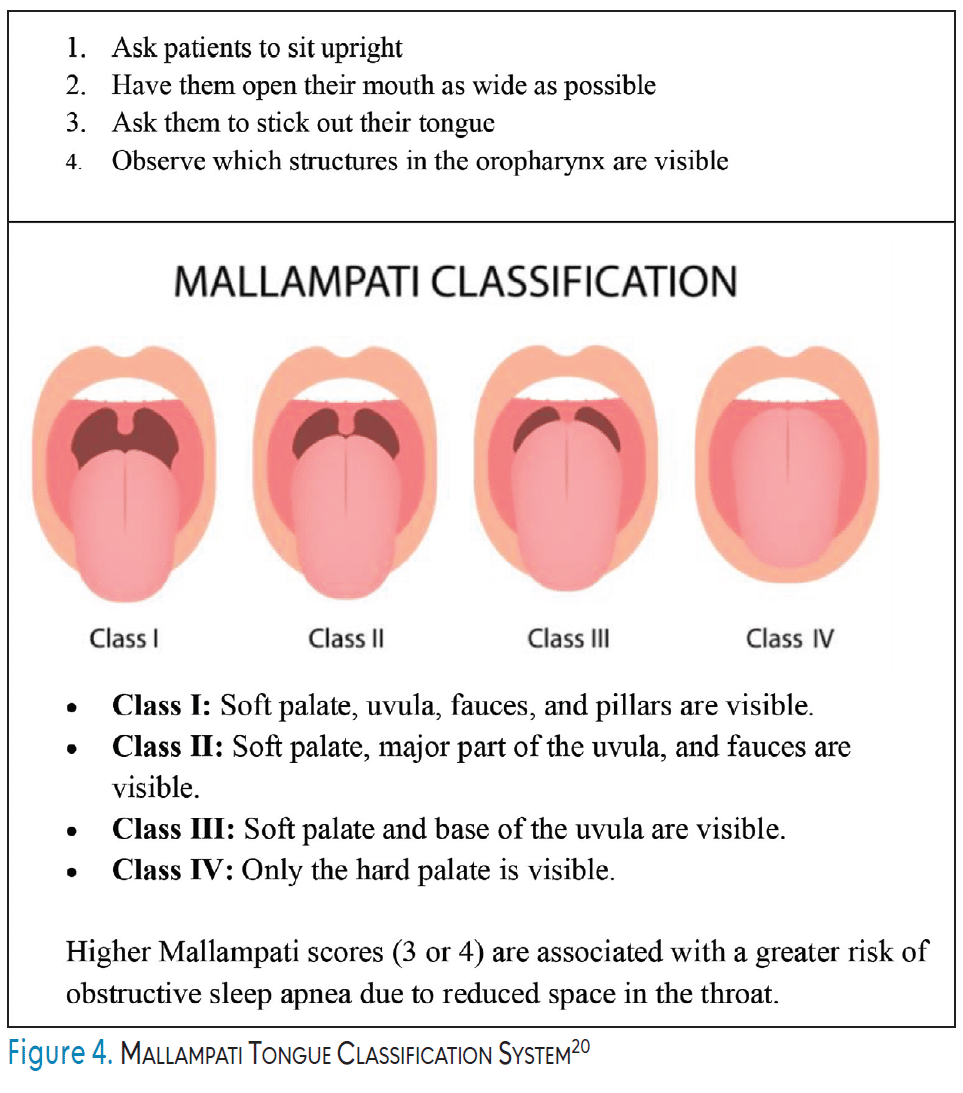
Look. Dental hygienists should first note visible signs of POSA, including retrognathic jaw, receding profile, dark undereye circles, and signs of obesity. During the intraoral assessment, the presence of enlarged tonsils should be noted. The Mallampati tongue classification system can be used to visually assess tongue size and airway obstruction (Figure 4).10, 22 Untreated tongue tie, high arched or narrow palate, as well as bruxism, mouth breathing, and shiny or swollen gums should be noted.8,14
Refer. Once the assessment is complete, the dental hygienist, with consultation and approval of the dentist, should determine whether to recommend a referral based on the number and combination of potential POSA symptoms. The dental hygienist can then educate the parent/caregiver and patient by discussing noted signs and symptoms, as well as explaining the risks of untreated POSA. The dentist may then refer the parent/caregiver to a sleep specialist. The parent/caregiver should be informed that POSA must be diagnosed by a physician, but that treatments may occur in a dental or orthodontic office depending on the physician’s treatment plan.
The ALR method simplifies POSA screening by giving clinicians a structured, simple evaluation process that can be integrated into the processes already in place during preventive care visits.
Conclusion
POSA can have serious long-term health consequences if left untreated. Dental hygienists can screen for POSA during routine exams, educate caregivers/parents and patients, and, with the help of the dentist, refer patients to physicians, all of which can significantly improve the overall health and well-being of children.
References
- Baker-Smith C, Amal I, Melendres MC, et al. Sleep-disordered breathing and cardiovascular disease in children and adolescents: a scientific statement from the American Heart Association. J Am Heart Assoc. 2021;10:022427.
- Alsubie HS, BaHammam AS. Obstructive sleep apnea: children are not little adults. Paediatr Respir Rev. 2017;21:72-79.
- Levine B, Patterson F, Covington L. Pediatric dentists: frontline public health providers leading the way in identifying and preventing childhood obstructive sleep apnea syndrome. Del J Public Health. 2024;10:44-45.
- Chang SJ, Chae KY. Obstructive sleep apnea syndrome in children: epidemiology, pathophysiology, diagnosis, and sequelae. Korean J Pediatr. 2010;53:863-871.
- Hanlon CE, Binka E, Garofano JS, Sterni LM, Brady, TM. The association of obstructive sleep apnea and left ventricular hypertrophy in obese and overweight children with history of elevated blood pressure. J Clin Hypertens. 2019;21:984-990.
- Maniaci A, Lavalle S, Parisi FM, Barbanti M, Cocuzza S, Iannella G, et al. Impact of obstructive sleep apnea and sympathetic nervous system on cardiac health: a comprehensive review. J Cardiovasc Dev Dis. 2024;11:204.
- Al-Hammad NS, Hakeem LA, Salama FS. Oral health status of children with obstructive sleep apnea and snoring. Pediatr Dent. 2015;37:35-39.
- American Academy of Pediatric Dentistry. Policy on obstructive sleep apnea (OSA). The Reference Manual of Pediatric Dentistry. Chicago: American Academy of Pediatric Dentistry; 2023:137-140.
- Gupta, S, Sharma, R. Pediatric obstructive sleep apnea: diagnostic challenges and management strategies. Cureus. 2024;16:1-19.
- Stauffer J, Okuji DM, Lichty GC II, et al. A review of pediatric obstructive sleep apnea and the role of the dentist. J Dent Sleep Med. 2018;5:111-130.
- Kanney M, Harford KL, Raol N, Leu RM. Obstructive sleep apnea in pediatric obesity and the effects of sleeve gastrectomy. Semin Pediatr Surg. 2020;29:150887.
- Chidambaram AG, Jhawar S, McDonald CM, Nandalike K. Sleep disordered breathing in children with neuromuscular disease. Children. 2023;10(:1675.
- Cielo CM, Marcus CL. Obstructive sleep apnoea in children with craniofacial syndromes. Paediatr Respir Rev. 2015;16:189-196.
- Durán-Cantolla J, Alkhraisat MH, Martínez-Null C, Aguirre JJ, Rubio Guinea E, Anitua E. Frequency of obstructive sleep apnea syndrome in dental patients with tooth wear. J Clin Sleep Med. 2015;11:445-450.
- Huang YS, Quo S, Berkowski JA, Guilleminault C. Short lingual frenulum and obstructive sleep apnea in children. Int J Pediatr Res. 2015;1:273.
- Stevens, D, Title, M, Spurr, K, Morrison, D. Positive airway pressure therapy adherence and outcomes in obstructive sleep apnea: an exploratory longitudinal retrospective randomized chart review. Can J Respir Ther. 2024;60:28-36.
- Bariani, RCB, Guimaraes, TM, Cappellette Jr, M, Moreira, G, Fujita, RR. The impact of positive airway pressure on midface growth: a literature review. Braz J Otorhinolaryngol. 2020;86:647-653.
- Carmody JK, Duraccio KM, Krietsch KN, Simmons DM, Byars KC. Factors affecting pediatric adherence to positive airway pressure: Patient and caregiver reported treatment barriers and sleep difficulties. Sleep Med. 2023;101:58-65.
- Bandyopadhyay A, Kaneshiro K, Camacho M. Effect of myofunctional therapy on children with obstructive sleep apnea: a meta-analysis. Sleep Med. 2020;75:210-217.
- Salzano G, Maglitto F, Bisogno A, et al. Obstructive sleep apnoea/hypopnoea syndrome: relationship with obesity and management in obese patients. Acta Otorhinolaryngol Ital. 2021;41:120-130.
- Fagundes NCF, Flores-Mir C. Pediatric obstructive sleep apnea—dental professionals can play a crucial role. Pediatr Pulmonol. 2022;57:1860-1868.
- O’Brien SM. Understanding the Mallampati score. Available at clinicaladvisor.com/features/understanding-the-mallampati-score. Accessed April 3, 2026.
From Dimensions of Dental Hygiene. May/June 2026; 24(3):40-45
