A ranula is a pseudocyst characterized by the leakage of excess fluid from salivary gland ducts into the surrounding soft tissues. It is a benign soft tissue mass in the floor of the mouth off the midline. The overlying stretched tissue is pale in appearance and bluish-tinted in color because of mucus accumulation. Ranula is derived from the Latin word “rana,” which means frog, and “ula” meaning little. The swelling resembles the air sacs of the frog.1 The lesion generally occurs due to trauma, sialolith, congenital duct obstruction, stenosis, periductal fibrosis, or tumor. Most ranulas originate from the secretions of the sublingual gland, but they can develop from the secretions of the submandibular gland duct or the minor salivary glands on the floor of the mouth.2
Ranulas that involve the major salivary glands are divided into three types: oral or simple ranula, cervical or plunging ranula, and mixed ranula. A simple ranula can be a mucus retention cyst confined to the floor of the mouth (intraoral swelling only). The cervical/ plunging ranula is a mucus extravasation pseudocyst arising from the sublingual gland and presents as a swelling in the neck (submandibular swelling without intraoral and extraoral swelling).3 The mixed ranula is an elevation in the floor of the mouth with intraoral and extraoral swelling.
Simple ranulas occur in two out of 10,000 individuals and only 6% of all oral sialocysts are ranulas.4 Few surgeons will encounter more than one simple ranula per year.4 Cervical/ plunging ranulas are even more rare.
In general, ranulas are most commonly seen in individuals younger than age 30.2 The prevalence of simple ranulas is slightly higher in women. Cervical/plunging ranulas occur more frequently in men who are in their 30s.2 Race does not appear to play a role in the prevalence of any of the ranulas.2
CLINICAL OBSERVATIONS AND FEATURES
Large simple ranulas can interfere with tongue placement. The simple ranula can also produce a deviation of the tongue and cross the midline, interfering with oral functions. An enlarged mass, the simple ranula is asymptomatic, movable, nontender, and may change in size over time. The overlying skin is usually intact.5 In most instances, all types of ranulas are localized to one side of the mouth and are easily identified by their blue color.6
The cervical/plunging ranula is a mucus escape reaction that is caused by a disruption of the sublingual salivary gland excretory duct or an obstruction of salivary flow.3 It has a smooth surface; varies in size; does not blanch or compress; and is soft, painless, and slow-growing.
The cervical/plunging ranula consists of a central cystic space containing mucin and a wall composed of loose, vascularized connective tissue. Histocytes predominate in the pseudocyst wall and, over time, become less prominent. The cervical/plunging ranula develops a dense, fibrous connective tissue pseudocystic capsule. An important feature is the absence of epithelial lining in the pseudocyst/ cavity wall.3 The viscosity of the cystic fluid helps to differentiate between the submandibular and sublingual glands based on the amount of mucus-secreting cells. The submandibular gland consists of mixed mucus and serous cells.7 If the mass is located in the deeper aspect of the floor of the mouth, it loses its bluish color.
DIAGNOSTIC CONSIDERATIONS

A fine-needle aspiration procedure will confirm the diagnosis of a cervical ranula by its high amylase count. In the chemical analysis, the fluid consists of high protein indicating the presence of inflammatory cells with the mucus.4 A simple ranula is identified by the patient’s history; clinical findings, such as appearance and characteristic location; radiographic images; magnetic resonance imaging (MRI); and fine-needle aspiration.
TREATMENT
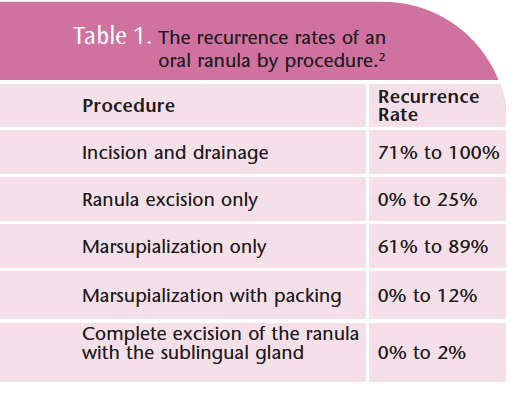
Treatment for a simple ranula involves excision of the lesion. Another method is simple marsupialization or incision of the cyst creating a pouch and suturing of the ranula followed by packing of the entire cyst cavity with gauze for 7 days to 10 days. This technique is not widely accepted because the recurrence rate is high in large lesions. An alternative approach is the complete removal of the ranula and its major salivary gland. Laser ablation and cryo surgery alone or after marsupialization are also used to treat ranulas. See Table 1 for recurrence rates. The cervical/ plunging ranula is best treated by complete surgical excision of the lesion and the sublingual gland.
A CASE REPORT
A 27-year-old Vietnamese-Chinese American woman presented for evaluation of a right swelling on the floor of the mouth to the right of the midline under the tongue. The swelling, gradually enlarging, had been present for approximately 2 weeks. The patient’s history did not indicate any trauma, surgery, or infections on the right side of her face or neck. According to the patient, the swelling fluctuates in size, especially during times of stress with no correlation to meals. At the initial visit to her dentist, the patient was referred to an oral surgeon. The patient was examined then by two oral surgeons. The first oral surgeon recommended a laser procedure. The second surgeon referred the patient to an ear, nose, and throat (ENT) specialist on the basis of the clinical examination. He felt that the area was too sensitive for a laser treatment and excision of the ranula would yield the best results.
Clinical examination of the head and neck region noted no abnormalities. An intraoral examination revealed a small anterior ranula present in the floor of the mouth (Figures 1 and 2). An MRI showed the ranula was nonplunging (Figure 3). Prior to the second appointment with the ENT specialist, the ranula drained spontaneously. The physician suggested that surgery was not absolutely necessary at this time. The patient was asked to return in 6 months for re-evaluation. Since her visit, the patient reported that the swelling fluctuated in size, but at no time completely disappeared and did not affect her speech. Prior to the re-evaluation visit, the patient’s speech began to be affected due to growth of the the lesion. Re-evaluation by the ENT specialist indicated the need for excision of the ranula and sublingual gland. Both were surgically removed. There were no complications.
CONCLUSION
Recommended treatment for simple ranulas is a surgical procedure. The recurrence rate is high for all ranulas if the sublingual gland is not removed. Although the incidence of ranulas is rare, patient education is important. Early recognition of the symptoms of all swellings and lesions in the oral cavity will help in the ranula management process and will hopefully encourage patients to bring these to the attention of a dental professional in case the swelling is indicative of a more serious prognosis such as oral cancer.
REFERENCES
- Baurmash HD. Mucoceles and ranulas. J Oral Maxillofac Surg. 2003;61:369-378.
- Flaitz CM, Hicks JM. Mucocele and ranula: treatment and medication. Available at: http://emedicine.medscape.com/article/1076717-treatment. Accessed October 7, 2009.
- Davison MJ, Morton RP, McIvor NP. Plunging ranula: clinical observations. Head Neck. 1998; 20:63-68.
- McGurk M. Management of the ranula. J Oral Maxillofac Surg. 2007;65:115-116.
- Zhao YF, Jia Y, Chen XM, Zhang WF. Clinical review of 580 ranulas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:281-287
- Louis PJ, Hudson C, Reddi S. Lesion of floor of the mouth. J Oral Maxillofac Surg. 2002;60:804-807.6.
- Baurmash HD. Treating oral ranula: another case against blanket removal of the sublingual gland. Br J Oral Maxillofac Surg. 2001;39:217- 220.
From Dimensions of Dental Hygiene. April 2010; 8(4): 32-34.
