 STANDRET / ISTOCK / GETTY IMAGES PLUS
STANDRET / ISTOCK / GETTY IMAGES PLUS
Importance of Micronutrients in Both Systemic and Oral Health
Remaining up to date on the important role vitamins and minerals play in a functioning immune system as well as how they relate to oral health is part of providing patient-centered care.
This course was published in the April 2022 issue and expires April 2025. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the important roles specific vitamins and minerals play in keeping the immune system strong.
- Explain how certain deficiencies negatively affect the immune system and the oral cavity.
- Discuss supplementation and the recommended daily dose of certain micronutrients.
Interest in vitamins, immune-boosting foods, and healthy lifestyle choices has grown significantly. Besides protecting against disease, a healthy immune system also helps support good oral health. On the other hand, deficiencies in micronutrients can cause negative oral health effects and worsen oral diseases. Dental hygienists should remain current on the important role vitamins and minerals play in a healthy immune system as well as how they relate to oral health.
The Immune System
The immune system consists of two major processes that protect the body from undesirable invaders: innate immunity and adaptive immunity.1,2 Innate immunity is when the body rapidly recognizes invaders via immune cells—such as neutrophils, cytokines, macrophages, leukocytes, and complement proteins—to destroy pathogens.2 Part of the innate immunity, physical anatomical barriers, such as skin, mucous membranes, and cilia, act as natural barriers to microorganisms. T-lymphocytes (T-cells) and B-lymphocytes (B-cells) are components of adaptive immunity. Adaptive immunity is how the body remembers pathogens it may encounter at a later date. This is accomplished by producing antibodies that specifically target and destroy the foreign invader.1 The process develops over time either from exposure to a pathogen or through immunization.2 Regardless of which process fends off pathogens, each stage of the immune system requires the support of certain micronutrients.3
The use of supplements, especially vitamin C, vitamin D, and zinc, has shown efficacy in supporting the immune system.1,2,4 Additionally, deficiencies in micronutrients impair the immune system’s ability to protect health.1,2,4 These deficiencies hinder the body’s ability to fight off infection and weaken adaptive immunity, leading to immunodeficiency.5 For example, vitamin C deficiency can lead to impaired wound healing, vitamin D deficiency may reduce the number of lymphocytes and impair macrophages, and zinc deficiency can impair the body’s antibody response to T cell-dependent antigens.3,6,7
Many factors can contribute to micronutrient deficiency including low intake of nutrition-rich foods, exposure to environmental toxins, and presence of chronic diseases.6
Vitamin C
Considerable research has been conducted that looks at the connection between vitamins/minerals and oral health. A recent systematic review and meta-analysis revealed overall weak evidence supporting the association between vitamin supplementation and oral pathological processes.8 However, many of these studies have limitations, such as poor design and inconsistency in dosage and formulation of the micronutrient being studied. For example, a study may research vitamin C and its effect on periodontal diseases while using a multivitamin instead of a vitamin C supplement. However, research does demonstrate a strong correlation between micronutrient deficiency and oral health problems.8–15

Photo credit: Published with permission from Gicchino MF, Romano A, Cioffi S, et al. Oral manifestations in scurvy pediatric patients: a systematic review and a case report. Applied Sciences. 2021;11(18):8323.
Crucial to the structural integrity of such innate barriers as mucosal cells, vitamin C promotes collagen synthesis and provides protection from free radicals. Vitamin C is necessary for innate immune cell function and is integral in the clearing and apoptosis of immune cells ready to be cleared by macrophages. Furthermore, vitamin C aids in the generation of antibodies and T-cell production and proliferation, and is a vital antioxidant.3,6,12 Studies indicate a daily intake between 100 mg and 400 mg of vitamin C is enough to ensure adequate plasma levels that meet the body’s needs.3,6 A recent study of vitamin C supplementation in older adults showed improvement in immune cell function.16
Vitamin C provides an antiviral effect and may reduce the severity and duration of colds and flu.3,5,12,13,14 Additionally, the administration of high-dose intravenous vitamin C may reduce the inflammatory cytokine storm and potentially improve outcomes and reduce morbidity in severe COVID-19 cases. Clinical studies are currently in progress to understand this further.13,14
Vitamin C plays a crucial role in the synthesis of collagen, therefore, vitamin C deficiency is evident in collagen-rich tissue such as the gingiva.3,6,15 Modest evidence suggests vitamin C helps reduce periodontal disease risk and may decrease bleeding on probing among patients with chronic periodontitis.8,15 One study demonstrated that individuals with chronic periodontitis ate fewer fruits and vegetables rich in vitamin C.8
Though rare, scurvy—caused by extreme vitamin C deficiency—still occurs in individuals with highly selective dietary habits and neurodevelopmental disorders. Gicchino et al17 provided a case study of a child with an exceptionally limited diet who presented with extremely swollen and painful gingival tissue as a result of vitamin C deficiency (Figure 1). Figure 2 shows the gingival improvement 4 weeks after supplementation began. Vitamin C deficiency can also result in gingival edema, friable and erythematous papilla, petechia on interdental papilla, and aphthous ulcers.9,10
Studies indicate statistical associations between chewing ascorbic acid or vitamin C tablets and developing tooth erosion.18,19 Dental erosion occurs when the oral environment’s pH falls below 5.5 pH, resulting in loss of enamel’s surface layers. Dental hygienists should educate patients on the potential harm of chewable vitamin C tablets if used in excess or for prolonged periods of time. Providing nutritional counseling on ways to add vitamin C to the diet may also be helpful. Additionally, individuals could opt for a supplement that is swallowed as opposed to chewed. When chewable vitamin C tablets are used per the manufacturer’s instructions, no obvious harm to the dentition appears to occur.18,19

Photo credit: Published with permission from Gicchino MF, Romano A, Cioffi S, et al. Oral manifestations in scurvy pediatric patients: a systematic review and a case report. Applied Sciences. 2021;11(18):8323.
Zinc and Immunity
Zinc, a metal, is essential to numerous processes in the human body, especially the immune system.20 Zinc is responsible for maintaining the integrity of skin and mucosal membranes; enhancing natural killer cells that are important for the growth and differentiation of immune cells that rapidly turnover; and modulating cytokine release.3 Zinc has strong antiviral properties, and has been shown to hinder the replication of viruses responsible for the common cold and upper respiratory infections. The recommended daily amount of zinc is 11 mg for adult men and 8 mg for adult women.
Studies reveal that supplementing daily with zinc significantly reduces the duration of the common cold.20,21 A randomized, double-blind, placebo-controlled clinical trial revealed that participants who took a zinc gluconate lozenge containing 13.3 mg of zinc experienced a significant reduction in the duration of cold symptoms.21
Zinc deficiency is the main clinical sign of immunodeficiency. Specifically, zinc deficiency leads to an increased risk of excessive inflammation, resulting from impaired neutrophil granulocytes, monocytes, macrophages, and natural killer cell function, as well as reduced T and B cell development.7,20 Preterm infants and older adults are most susceptible to zinc deficiency. Preliminary data indicate that ensuring proper zinc levels may help reduce lung inflammation and prevent ventilator-induced lung injury. Further clinical trials are needed to understand the mechanism of action.20
Zinc is key to maintaining periodontal health due to its positive immunological effects on oral tissue, help in the formation of enamel, and its role in preventing the formation of biofilm and calculus.11 Zinc-based salts are used in many dental products, such as toothpastes and mouthrinses, to help control the accumulation of calculus. Studies show adequate zinc levels during pregnancy are linked to lower occurrences of orofacial clefts in newborns.11
Zinc deficiencies can lead to angular cheilitis, impaired wound healing, and burning mouth syndrome. A condition called perioral and periorificial dermatitis, which presents as a u-shaped erythematous rash around the lower lip, can also be observed in infants deficient in zinc.11 Figure 3 shows an infant with acrodermatitis enteropathica, a genetic disorder inhibiting zinc absorption.22 Zinc deficiency from no to low dietary intake can also result in this oral manifestation.23

Photo Credit: Published with permission from Glutsch V, Hamm H, Goebeler M. Zinc and skin: an update. J Dtsch Dermatol Ges. 2019;17:589–596.
Vitamin D
Vitamin D plays a crucial role in supporting the skeletal system, and receptors for it are found in cell types throughout the body. The importance of vitamin D is just beginning to be understood. More studies are emerging that discuss the relevance of vitamin D in connection to disease development and severity.24–34
Humans acquire vitamin D through dietary consumption, which typically makes up around 20% of what the body needs, and by skin synthesis, which provides roughly 80% of the body requires.24 When first introduced into the body, vitamin D is in an inactive form until it is converted to the active form vitamin D3 (cholecalciferol).25 Evidence suggests that vitamin D is synthesized by cells that contribute to innate immunity such as macrophages, monocytes, and epithelial cells.24–26 Specifically, pulmonary epithelial cells can synthesize the inactive form of vitamin D to produce active vitamin D locally, which then provides protection against respiratory infections.25 Once this synthesis takes place, vitamin D binds to the numerous vitamin D receptors throughout the body and functions similar to a hormone.24,26
Vitamin D plays an important role in adaptive immunity as well. It reduces inflammation by decreasing pro-inflammatory cytokines, and increasing regulatory T cells and anti-inflammatory type 2 cytokines.25,26
Serum levels of vitamin D need to be maintained within a specific range for optimum health. Testing serum levels is considered the most accurate method of measuring vitamin D status.26 However, measuring free, unbound vitamin D can be challenging if it occurs in naturally low levels. Free, unbound vitamin D may be more physiologically relevant than the total concentration of vitamin D in understanding deficiency.26 A normal range of vitamin D is a level equal to or greater than 30 ng/ml, between 20 ng/ml and 29 ng/ml is considered insufficient, and less than 20 ng/ml is deficient.24,25,27
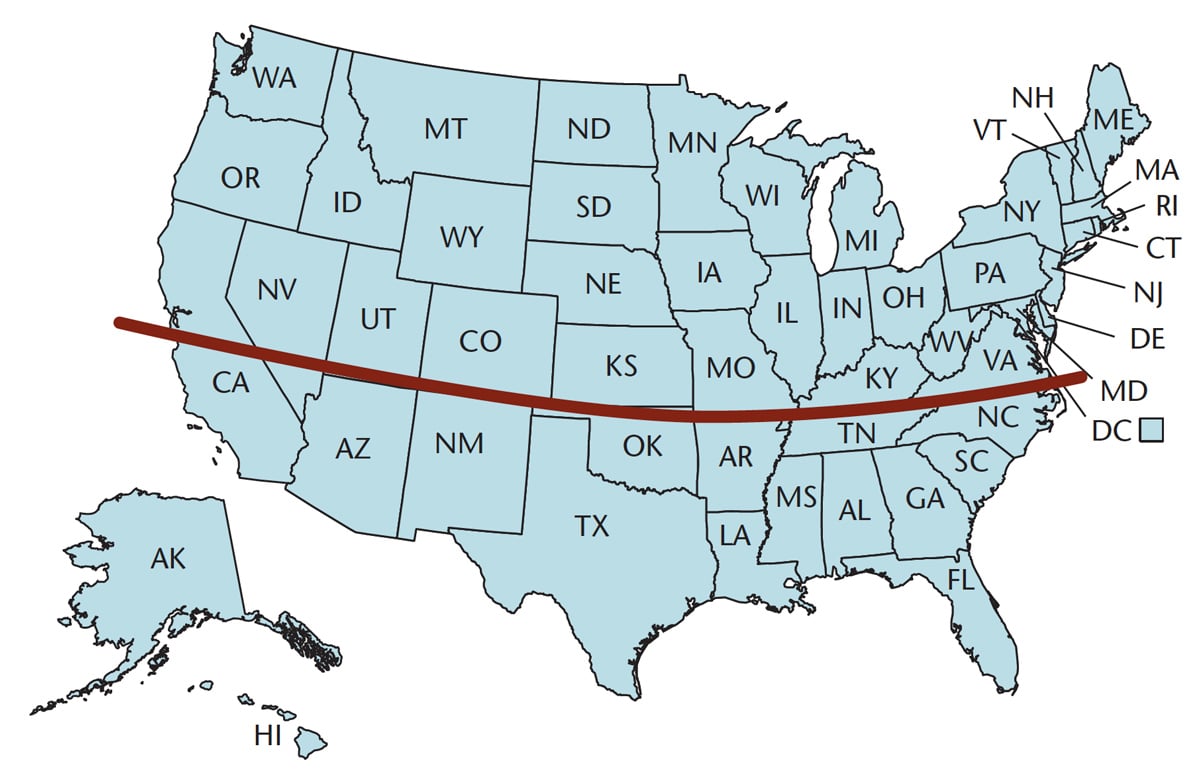
Several factors impact whether one has sufficient vitamin D levels, including how much time is spent outdoors, whether sunscreen is used, and diet. Individuals living in countries below 35° latitude on either side of the equator are exposed to adequate UVB radiation year-round to support vitamin D synthesis.26 Figure 4 shows the line approximating 35°, with those living in states above the red line experiencing difficulty synthesizing enough vitamin D in the winter. Eighty percent of vitamin D is gained via exposure to the sun, so those living in northern parts of the world will need to find other ways to ensure they are getting enough vitamin D. For example, in Northern Europe, sunlight does not contain sufficient UVB levels to initiate vitamin D synthesis until late May, early June.26,28 A retrospective epidemiological study of 148,821 Americans living in the northern latitude demonstrated that the highest rates of vitamin D deficiency occurred during the winter months.29 Older individuals and people with more melanin in their skin do not synthesize vitamin D through their skin as easily as do younger people or those with lighter skin tones. Therefore, the incidence of deficiency tends to be higher in these populations.24,26,28
Experts suggest that exposure to the sun on bare arms, legs, and face for 5 minutes to 30 minutes a day between the hours of 10 am and 4 pm should be enough to synthesize adequate vitamin D from UVB light.24 The recommended dietary allowance for vitamin D is 600 IU daily for those younger than 70 and 800 IU for individuals older than 70.24 However, a 120-month study of Dutch athletes revealed that supplementing with 2,200 IU/day resulted in adequate active vitamin D concentrations in 80% of the participants.30 A daily regimen of vitamin D seems to be more beneficial for sustaining serum levels than intermittent high doses of vitamin D. In the US, vitamin D is added to a variety of foods including milk, orange juice, cereals, bread, and yogurt.28
Modest evidence supports a relationship between low plasma vitamin D levels and periodontal diseases as measured by gingival index and attachment loss.31 A systematic review found 65% of cross-sectional studies showed periodontal disease progression could be attributed to vitamin D levels, but further research is needed.32 Studies have shown an association between low vitamin D and oral cancer.33 A comprehensive review by Botelho et al34 revealed vitamin D deficiencies were associated with enamel and dentin defects in children, a higher prevalence of periodontal diseases and gingival inflammation, and certain oral cancers and osteonecrosis. Additionally, loss of periodontal attachment and permanent dentition changes, such as enamel pitting and hypoplasia, are associated with rickets.9
Conclusion
Evidence clearly shows the importance of maintaining adequate levels of micronutrients.2,3 Dental hygienists and their patients will benefit from a knowledge of how micronutrients strengthen the immune system and benefit the oral environment.
References
- Pecora F, Persico F, Argentiero A, Neglia C, Esposito S. The role of micronutrients in support of the immune response against viral infections. Nutrients. 2020;12:3198.
- Rondanelli M, Miccono A, Lamburghini S, et al. Self-care for common colds: the pivotal role of vitamin D, vitamin C, zinc, and echinacea in three main immune interactive clusters (physical barriers, innate and adaptive immunity) involved during an episode of common colds—practical advice on dosages and on the time to take these nutrients/botanicals in order to prevent or treat common colds. Evid Based Complement Alternat Med. 2018; 2018:5813095.
- Gombart AF, Pierre A, Maggini S. A review of micronutrients and the immune system-working in harmony to reduce the risk of infection. Nutrients. 2020;12:236.
- Cámara M, Sánchez-Mata MC, Fernández-Ruiz V, Cámara RM, Cebadera E, Domínguez L. A review of the role of micronutrients and bioactive compounds on immune system supporting to fight against the COVID-19 disease. Foods. 2021;10:1088.
- Gorji A, Khaleghi Ghadiri M. Potential roles of micronutrient deficiency and immune system dysfunction in the coronavirus disease 2019 (COVID-19) pandemic. Nutrition. 2021;82:111047.
- Schloss J, Lauche R, Harnett J, et al. Efficacy and safety of vitamin C in the management of acute respiratory infection and disease: a rapid review. Adv Integr Med. 2020;7:187–191.
- National Institutes of Health. Zinc Fact Sheet for Health Professionals. Available at: ods.od.nih.gov/factsheets/Zinc-HealthProfessional/#en68. Accessed March 22, 2022.
- Cagetti MG, Wolf TG, Tennert C, Camoni N, Lingström P, Campus G. The role of vitamins in oral health. a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17:938.
- Tada A, Miura H. The relationship between vitamin c and periodontal diseases: a systematic review. Int J Environ Res Public Health. 2019;16:2472.
- Tolkachjov SN, Bruce AJ. Oral manifestations of nutritional disorders. Clin Dermatol. 2017;35:441-452.
- Maares M, Haase H. Zinc and immunity: an essential interrelation. Arch Biochem Biophys. 2016;611:58–65.
- Bae M, Kim H. Mini-review on the roles of vitamin c, vitamin d, and selenium in the immune system against COVID-19. Molecules. 2020;25:5346.
- Carr AC, Maggini S. Vitamin C and immune function. Nutrients. 2017;9:1211.
- Gasmi A, Tippairote T, Mujawdiya PK, et al. Micronutrients as immunomodulatory tools for COVID-19 management. Clin Immunol. 2020;220:108545–108545.
- Cerullo G, Negro M, Parimbelli M, et al. The long history of vitamin c: from prevention of the common cold to potential aid in the treatment of COVID-19. Front Immunol. 2020;11:574029.
- De la Fuente M, Sánchez C, Vallejo C, Díaz-Del Cerro E, Arnalich F, Hernanz Ángel. Vitamin C and vitamin C plus E improve the immune function in the elderly. Exp Gerontol. 2020;142:111118.
- Gicchino MF, Romano A, Cioffi S, et al. Oral manifestations in scurvy pediatric patients: a systematic review and a case report. Applied Sciences. 2021;11:8323.
- Li H, Zou Y, Ding G. Correction: dietary factors associated with dental erosion: a meta-analysis. PloS One. 2016;11:e0161518.
- Bahal P, Djemal S. Dental erosion from an excess of vitamin C. Case Rep Dent. 2014;2014:485387.
- Fukada T, Hojyo S, Hara T, Takagishi T. Revisiting the old and learning the new of zinc in immunity. Nat Immunol. 2019;20:248–250.
- Skalny A, Rink L, Ajsuvakova O, et al. Zinc and respiratory tract infections: perspectives for COVID 19 (Review). Int J Mol Med. 2020;46:17–26.
- Glutsch V, Hamm H, Goebeler M. Zinc and skin: an update. J Dtsch Dermatol Ges. 2019;17:589–596.
- Uwitonze AM, Ojeh N, Murererehe J, Atfi A, Razzaque MS. Zinc adequacy is essential for the maintenance of optimal oral health. Nutrients. 2020;12:949.
- Siddiqui M, Manansala JS, Abdulrahman HA, et al. Immune modulatory effects of vitamin D on viral infections. Nutrients. 2020;12:2879.
- Rhodes JM, Subramanian S, Laird E, Griffin G, Kenny RA. Perspective: vitamin D deficiency and COVID‐19 severity—plausibly linked by latitude, ethnicity, impacts on cytokines, ACE2 and thrombosis. J Intern Med. 2021;289:97–115.
- Hewison M. An update on vitamin D and human immunity. Clin Endocrinol. 2012;76:315–325.
- Balla M, Merugu GP, Konala VM, et al. Back to basics: review on vitamin D and respiratory viral infections including COVID-19. J Community Hosp Intern Med Perspect. 2020;10:529–536.
- National Institute of Health. Vitamin D Fact Sheet for Health Professionals. Available at: ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/. Accessed March 22, 2022.
- Zdrenghea MT, Makrinioti H, Bagacean C, Bush A, Johnston SL, Stanciu LA. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev Med Virol. 2017;27.
- Huotari A, Herzig KH. Vitamin D and living in northern latitudes-an endemic risk area for vitamin D deficiency. Int J Circumpolar Health. 2008;67:164–178.
- Rosecrans R, Dohnal JC. Seasonal vitamin D changes and the impact on health risk assessment. Clin Biochem. 2014;47:670–672.
- Pinto JPNS, Goergen J, Muniz FWMG, Haas AN. Vitamin D levels and risk for periodontal disease: a systematic review. J Periodontal Res. 2018;53:298–305.
- Fathi N, Ahmadian E, Shahi S, et al. Role of vitamin D and vitamin D receptor (VDR) in oral cancer. Biomed Pharmacother. 2019;109:391–401.
- Botelho J, Machado V, Proença L, Delgado AS, Mendes JJ. Vitamin D deficiency and oral health: a comprehensive review. Nutrients. 2020;12:1471.
From Dimensions of Dental Hygiene. April 2022;20(4):28,31-33.
