 BRANDYTAYLOR/E+/GETTYIMAGESLUS ACCESS to Care
BRANDYTAYLOR/E+/GETTYIMAGESLUS ACCESS to Care
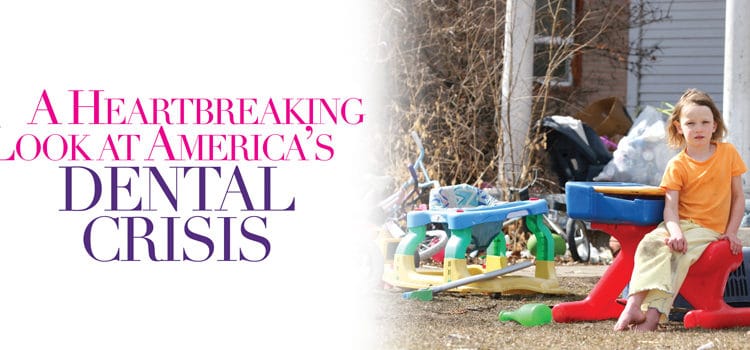
A Heartbreaking Look at Americas Dental Crisis
Author Mary Otto shares her insight on the status of oral health care delivery in the United States and the radical change it needs to better serve disadvantaged populations.
In March 2017, Mary Otto’s book Teeth: The Story of Beauty, Inequality, and the Struggle for Oral Health in America took the public health arena by storm. It investigates the status of the oral health care delivery system in the United States and provides an intimate look at the lives of those individuals most significantly impacted by the nation’s access-to-care problem. Otto not only reports the facts, but she shares truly heartbreaking stories of the most vulnerable in our society who suffer greatly within the confines of a broken system. The New York Times Book Review commented, “[Teeth is] . . . more than an exploration of a two-tiered system―it is a call for sweeping, radical change.”
Perspectives on the Midlevel Practitioner invited Otto to share her thoughts regarding Teeth and its impact on the efforts to create a more equitable and efficient oral health care delivery system.
 Q What inspired you to write this book?
Q What inspired you to write this book?
A I got started covering oral health in 2007, as a staff writer for the Washington Post, reporting the story of Deamonte Driver, a 12-year-old Maryland boy who died after suffering complications from tooth decay. Doctors said that bacteria from an abscessed tooth had spread to his brain. As I continued to follow the issue, I began to see this child’s sickness and death as part of a much larger story. Inexpensive, routine preventive care might have saved Deamonte if he had received it throughout his childhood. But he was a poor Medicaid child and most Medicaid children in Maryland and throughout the country were not—and still are not—receiving routine care. They are among the more than one-third of Americans who experience significant barriers in accessing dental care. Deamonte and his brothers, like the vast majority of children covered by Medicaid, received medical services, such as the immunizations they needed for school. But in our system, dental care has historically been provided separately from other kinds of health care and for tens of millions of Americans, it is much harder to find.
Q What did you discover were the most significant drivers behind the US’s access-to-care problems?
A One problem is money. Millions of Americans don’t seek care because they cannot afford to pay for it, federal studies show. Private dental benefits can help pay for care but it has been estimated that approximately 114 million Americans are dentally uninsured. In addition, out-of-pocket costs for dental care have continued to rise. The cost barrier is the hardest for the elderly and the poor. Medicare, which covers more than 55 million retired and disabled Americans, has never included routine dental benefits. Medicaid, the federal program that covers approximately 72 million poor Americans, does not entitle adults to dental benefits. Medicaid leaves dental coverage up to the states and in some states, benefits are scant or even nonexistent. Poor children are entitled to dental benefits under the program but often do not receive care. Fewer than half of dentists participate in Medicaid, so it can be difficult to find a provider. Then too, dental providers are scarce in some places. Affluent metropolitan areas tend to have plenty of dentists but there is a chronic lack of dental providers in many poor, rural, urban, and minority communities, according to federal data. Roughly 49 million Americans live in federally designated dental professional shortage areas.
Q What roles do expanded scope for dental hygienists and the introduction of midlevel practitioners play in solving these problems?
A These workers are being used to broaden access to routine care in communities that have lacked it. As the result of efforts by dental hygienists’ groups along with public health, grassroots, and tribal organizations, dental hygienists in some states can now bill Medicaid directly for their services and provide care in schools and other settings to patients who have not first been examined by dentists. In tribal areas of Alaska, Washington, and Oregon, and throughout Minnesota, dental therapists are now offering needed dental services to patients who have long lacked care. But, as I learned in my reporting, some of these steps have been very hard-won due to strong resistance from state and national dental organizations. I talked with South Carolina dental hygienist Tammi Byrd, RDH, for example, whose school-based hygiene initiative was nearly shut down by the state dental board. I interviewed dental therapists in Alaska who were sued by dental organizations who hoped to stop their program. Yet in these and in other cases, the work of these providers was ultimately allowed to go forward in the interest of improved access to care.
Q What was the most shocking thing you discovered during your research?
A It has to have been the depth and intensity of America’s dental suffering. My reporting work took me from Florida to Alaska; I talked with families who had lost loved ones to dental infections; people sleeping in their cars with excruciating toothaches, hoping and praying for care at free clinics; I met people who had pulled out their own teeth in desperation; children who cried in fear of dental visits. On the hopeful side, though, I also met oral health professionals, researchers, policy experts, public officials, and lawmakers passionately devoted to getting care to people who need it; to better understanding the factors that contribute to health and disease; to promoting oral health literacy and to re-thinking the system; and to finding ways to address what former Surgeon General David Satcher, MD, PhD, called this country’s “silent epidemic” of oral disease.
Q Is there hope that the delivery system for dental care can be fixed so it reaches more people?
A I think there is. There seems to be a growing biological and political understanding of the importance of oral health. There is also an increasing awareness of the collective and personal cost of allowing oral disease to go unprevented and untreated: the millions of dollars spent on emergency department visits for toothaches, the dim job prospects for people who are missing teeth, and the work and school days lost due to oral pain. In his landmark Oral Health in America report, Satcher called for an American health care system that “meets the oral health care needs of all Americans and integrates oral health effectively into overall health.” He called for wider prevention efforts, workforce diversity, and interdisciplinary care. In my reporting, I had a chance to see all of these things at work, though sometimes on a small scale: dental hygienists delivering preventive services to children in poor schools; dental therapists bringing care to Alaskan tundra villages; and a federally qualified health center where dental, medical, and mental health providers were working collaboratively, offering “whole-patient care.” Still, far more work lies ahead if we really intend to bring dental services to the tens of millions of Americans who are currently going without them.
From Perspectives on the Midlevel Practitioner, a supplement to Dimensions of Dental Hygiene. October 2017;4(10):49-51.
