 baona / E+
baona / E+
Impact of the Global Pandemic on a University Dental Department
The pandemic that has enveloped the entire globe has become so complete that it is hard to remember that not long ago we were living our “normal” lives.
| Chandni Batra, BDS, MDS, Niloufar Daneshparvar, DDS, and Vanchit John, BDS, MDS, DDS, MSD, share their experience with continuing to educate the next generation of oral health professionals during COVID-19. |
The pandemic that has enveloped the entire globe has become so complete that it is hard to remember that not long ago we were living our “normal” lives. It seemed that one day we heard about this new virus and the next day we were all essentially shut down. In the period that followed, we have stopped all our classroom and clinical activity at the Indiana University School of Dentistry, and have worked overtime to adapt to the new reality of virtual learning. Following is a narrative of the Department of Periodontology at the Indiana University School of Dentistry’s response to COVID-19.
Our Timeline
On January 21, 2020, Periodontology Department Chair, Vanchit John, BDS, MDS, forwarded an article on a new virus from Wuhan, China, to the department and its alumni, with the subject line “something for us to be aware of.” In February, more reports started to come in about how the virus was spreading all over the world along with reports of people testing positive on the West Coast and the East Coast of the United States. This was soon followed with information about the severity of the disease in other countries, primarily Italy and Spain. Leaders of academic institutions soon realized they would need to make significant changes to their programs as understanding of how the virus spread became more clear. News about the shutting down of patient care clinics, clinical facilities, and academic institutions soon. At Indiana University, we were first notified that spring break was extended by another week, and soon after it was determined that face to face contact was prohibited.
Major Issues Facing the Department and the School
Once it became clear that the best way to flatten the curve (Figure 1) was through social distancing and sheltering in place, swift action followed.1
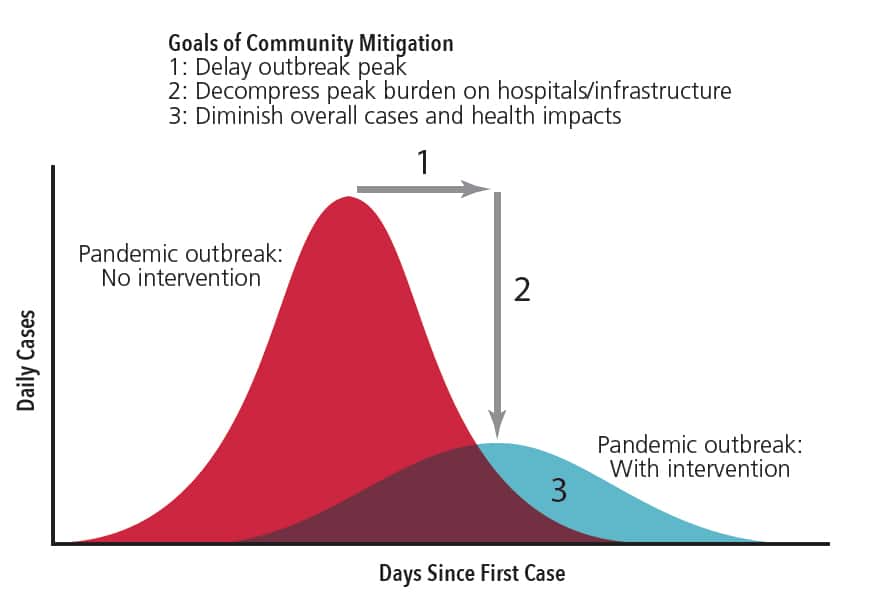
The logic behind flattening in the curve is if we as citizens aid in reducing the number of people who get sick by reinforcing routine steps like washing our hands, staying home if we felt sick and implementing social distancing, then we could all help slow the number of new cases. This would allow better use of the finite resources of our healthcare system. Many state governments issued shelter in place or stay at home orders. Following this. many professional organizations, namely, the Centers for Disease Control and Prevention, American Dental Association, and American Academy of Periodontology, began recommending that only emergency patient care be provided2 Accordingly, the majority of general dental and specialty offices shut down or had very limited scope of patient care. At the School of Dentistry and in the Department of Periodontology, similar mandates led to an almost complete cessation of routine and surgical patient care. Personnel were advised to avoid campus and to start developing plans to work and teach virtually or remotely.
We came up with the following list of our immediate concerns:
- How would we handle emergency patient care?
- How were we going to handle ongoing research projects if we were not allowed access to labs?
- How would we teach virtually if most of our teaching material was on our computers in our offices at the school?
- How were we going to quickly learn the technology for remote teaching and how would we rearrange all our schedules to account for this new reality?
- Would this apply similarly for large group (dental students) and small groups (residents)?
- How would we compensate for the clinical time that the residents were missing?
- What about the upcoming graduation times and dental licensing for graduates to practice dentistry and the specialty of periodontology in the community?
Everything was unfolding in a rapid fashion and we were faced with the task of quickly adapting to the situation without having many answers
What We Had Going In Our Favor
While it felt like everything was falling apart around us, it was important that we quickly regrouped and assessed what we had going in our favor
- We were blessed with a group of colleagues, staff and residents who were nimble and were quickly willing to change and adapt to the new reality
- Our parent university extended spring break by an extra week. This meant that we had an extra week to prepare.
- Most travel was being cancelled and this allowed us to get together remotely to discuss how we wanted to go about restructuring our curriculum.
- The full-time faculty met in one group, the staff and the department chairperson met at another time point, and then faculty and residents met to discuss how we were going to move forward, while testing out some of the nuances of the new virtual portal that we were going to use.
- We had a practice run to see how virtual learning worked for us.
- Then we rescheduled each week to fit in slots of virtual learning. These slots took the place of in-person seminars and the time spent in clinical care for our patients.
- We sought feedback from our residents and faculty and discussed concerns during the extra week. This preparation allowed the first full week of virtual learning to proceed almost flawlessly.
Working with the Dental Students
The Department of Periodontology and the School of Dentistry had a much bigger issue when it came to dealing with the dental students and reworking the curriculum in this arena. First, we were working with a much larger cohort of students as class sizes were 120 strong. Second, all in-person contact had ceased and this meant all pre-clinical labs and clinical activity had ground to a halt. This was a particularly critical time as the end of the semester was rapidly approaching and with it came project deadlines, patient work that had been started but not completed, and graduation.
The Department of Periodontology took stock of its situation as it applied to the dental students.
- The first-year lecture classes had been completed. However, the labs for scaling and root planing had not begun. Neither was the “Adult Prophylaxis Clinic” completed nor the final exam for the course. Since no contact was permitted, the plan was to reschedule the labs and the clinic activity for this cohort to later in the summer or early in the fall.
- There was no formal contact with the second-year dental students and periodontology in the regular curriculum, so this cohort of students were not affected.
- Year 3 students were to be given their remaining lecture information virtually.
- For the graduating class of students, we still had a small cohort remaining that needed to complete their patient experiences. Since no contact was permitted, an Objective Structured Clinical Exam (OSCE) was constructed, which served a surrogate for the clinical experiences. Imperfect as it was, it was the best option available.
Week 1
There was much excitement and trepidation as we began our first week of virtual learning. Would the technology work like we hoped? What were some of the unknowns that we were going to face? Would we have issues with internet connectivity that would limit what we could do during sessions?
We were very clear from the beginning that we needed to try to compensate for the clinical time that our residents were going to miss. Accordingly, we planned to include all of the clinical times missed into our weekly virtual learning schedules. We began the week with all of these concerns in the back of our minds. We were pleased with how efficiently Week 1 turned out. Everyone was enthusiastic and participated fully. Our plan to compensate for missing clinical time included having case-based learning and using break-out rooms for groups of residents to discuss assigned clinical situations and to come back to report to the larger group.
Week 2
The sophomore slump was real.3 There was a bit of a letdown with Week 2. The energy was a bit stagnant and, overall, it took a bit more participation from several people to get the group excited again. While we did manage to overcome the inertia, there was also a sense that maybe 6 to 8 hours a day of virtual learning was challenging.
We decided to conduct a survey to assess how everyone was handling the emotional, mental, and physical aspects of the change to virtual learning. We anonymously surveyed members of our department, upper administration, and dental students to get their feedback. Table 1 demonstrates the results.

Survey
Results: A total of 106 participants composed of upper administration, full-time and adjunct faculty, staff, students, and residents in the department of periodontology responded to the survey (Figure 2).
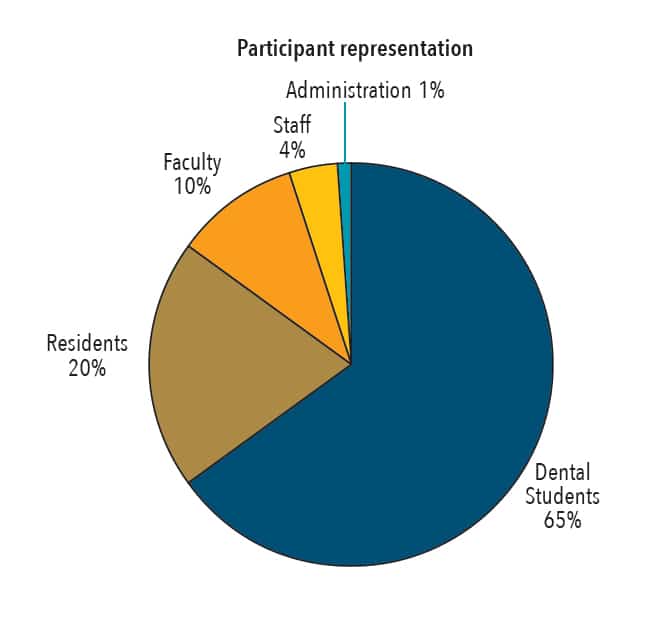
Question 1: identified respondents. The majority were dental students (65%) followed by residents (20%), faculty (10%), staff (4%), and administration (1%).
A multitude of options were explored in Question 2 “Has the global pandemic affected you personally?” The majority of the respondents (92.5%) felt that the quarantine was providing them time for personal growth and development. They also indicated that they were able to spend more time with family and friends either physically or virtually. Psychological stress due to travel and activity restriction, health risks, and loneliness impacted 47.5% of the participants to a little extent, while 30% felt they were affected a lot. Of those who responded, 60% were experiencing financial stress to some extent, while the majority indicated they were not affected by childcare issues. Approximately 80% of individuals were not finding themselves to be as productive as they wished to be and there was an almost equal distribution between those that had lost enthusiasm to a little extent (50%), and those who were not affected at all (47.5%). The majority of the participants (72%) expressed that their personal goals had been modified to some extent.
Various options were provided with Question 3, “Has the global pandemic affected you professionally?” Most of the participants were a little worried about job security and financial situations (32.5%), while 27% were not affected by this at all. However, 40% of the respondents were skeptical about graduating into an unstable economy and not having enough of a patient pool to hone their skills in the future. A large number of individuals (87%) were also concerned about future guidelines for infection control and lack of enough personal protective equipment. Some participants were finding virtual teaching and learning challenging to a little extent (45%), while for some (32%), it was very challenging.
Questions 4 and 5 were open ended. When asked about the personal changes they would want to make once the quarantine ends, most stated they would like to maintain a balance between work and family and spending more time taking care of themselves by exercising, cooking homemade meals, and finding time to do things they enjoy. Some also mentioned they would like to adapt to the uncertain times ahead and incorporate the “new normal” to their lives as soon as possible. As many participants were worried about the clinical time they had lost during this quarantine period, the changes they would like to incorporate at a professional level included gaining enough clinical experience, completing graduating requirements, learning from faculty, and becoming more responsible and organized. Many respondents indicated they would be more careful about infection control protocol and would more judiciously use the available personal protective equipment in the future. Some indicated a desire to use the knowledge learned during this quarantine time, such as the use of virtual platforms to schedule and attend meetings that were more difficult to schedule otherwise.
Week 3
Going into Week 3, we realized that a boost in the energy level or a reboot was going to be needed. Spending 6 to 8 hours every day in virtual learning sessions led to some virtual learning fatigue. Fortunately, we were able to have four presentations by colleagues not associated with the program and this really brought a well-needed boost to the overall level of enthusiasm. In addition, we were more cognizant of taking breaks and checking in with everyone. If we noticed a lag in the responses from the residents, we veered off topic for a minute or two to allow for resets to take place naturally. We also had a feedback session with the chief resident who had spoken to all his fellow residents about how they were doing and what they felt about the past three weeks of virtual learning.
Week 4
Week 4 turned out to be a very productive week of learning and debating. There seemed to be a renewal of the group enthusiasm that was facilitated by some excellent teaching. This was an area in which there was a lot of development from all of the faculty. As we watched each other closely over the course of 4 weeks, it was apparent that everyone was becoming more innovative with their use of visuals, adding more small group breakout sessions, posing several questions that made everyone search for the answers, and engaging in vigorous debate. In addition, the residents who participated in the sessions exhibited immense growth in their learning and in their use of virtual learning.
This was also apparent in the small group sessions with the dental students as the “chat” option in the virtual learning platform led students to pose many more questions than had been asked in sessions past. This was one of the silver linings in our education over the past 4 weeks at our dental school.
Lessons Learned Going into the Future
The global pandemic has changed our personal and professional lives forever. How are we going to move forward professionally? Here are some thoughts for us to ponder:
Is virtual learning going to replace classroom learning or will it become an equal partner?
We need to revisit our curriculum and find ways to increase our curricular efficiency. How do we make sure every learning hour is conducted in the most efficient manner possible?
If virtual learning is here to stay, how do we capture this technology to become a more focused educational methodology?
Time management: Dental curricula occupy a 4-year timeline and the residency programs are 2 to 3 years. Is there a need to restructure learning sessions as they currently exist to use virtual learning more effectively?
While our experiences with virtual learning were mainly positive, we did have one instance of interruption. 4,5 Virtual learning has problems that we need to be prepared to address as they arise.
Dentistry and periodontology are procedure-driven professions. They require patient care and what is referred to as ”wet fingered work.” Virtual learning will only take us so far.
Residents and dental students need to be allowed to go out into the communities and start their clinical work and earn a living. Currently this is on hold. What impact will this shut down have in the long run?
How are we going to deal with personal protective equipment changes, aerosol infections, antibody testing, and the potential for a second wave of infections?
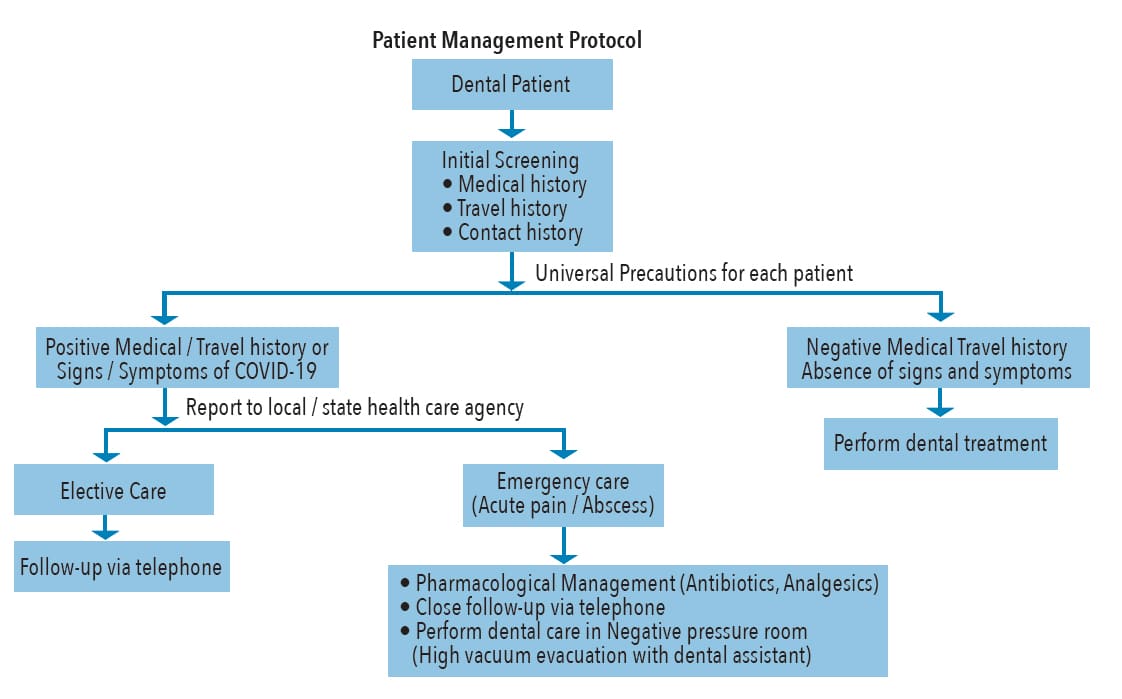
Figure 3 provides a possible protocol for patient management.
If we do have a second wave, are we going to be better prepared if and/or when it arrives? Each institution will need to have its own debriefing sessions.
Finally, we have all experienced a degree of personal sharing and caring that was almost unprecedented. How do we capture the essence of mutual support and take it into the future and not let old habits resurface?
The global pandemic and the subsequent shelter in place that we experienced led to an unprecedent period of activity and creativity in the Department of Periodontology at Indiana School of Dentistry. It was a time that none of us could have imagined at the beginning of the year 2020. However, as the situation presented itself, we quickly adapted and transitioned from in-person learning to virtual learning. The story of how we changed and excelled during this period is a lesson in positivity and one that has filled us with pride. We hope the lessons we learned will serve us well as we move into a future with many questions left to be answered.
References
- United States Centers for Disease Control and Prevention. Interim pre-pandemic planning guidance: community strategy for pandemic influenza mitigation in the United States. Available at: https://www.cdc.gov/flu/pandemic-resources/pdf/community_mitigation-sm.pdf.
- United States Centers for Disease Control and Prevention. CDC Guidance for Providing Dental Care During COVID-19. Available at: https://www.cdc.gov/oralhealth/infectioncontrol/statement-COVID.html.
- Sterling AJ. Student experiences in the second year: Advancing strategies for success beyond the first year of college. Available at: https://onlinelibrary.wiley.com/doi/full/10.1002/sem3.2011.
- Dillenbourg P, Schneider D, Synteta P. Virtual learning environments. Available at: https://pdfs.semanticscholar.org/8837/bf53a027baf2f7630e3a76ac693d4f392a4c.pdf.
—
For even more breaking news, follow us on Facebook.
For positive and inspirational posts during this uncertain time, follow us on Instagram.
