Early Detection of Syphilis
The number of syphilis cases has been rising in the United States and worldwide, especially in developing countries.

Rising Issue of Syphilis
The number of syphilis cases has been rising in the United States and worldwide, especially in developing countries. A particular danger of syphilis is transmission during pregnancy and development of congenital disease, resulting in fetal death or varying levels of disability, and the rate of congenital syphilis has also been increasing. Due to the frequent occurrence of syphilitic ulcers in the oral cavity, perioral regions, and head and neck areas, oral health professionals must be knowledgeable about the disease signs and symptoms, diagnosis, transmission, prevention, and treatment protocols.
Photo Credit: jarun011 / iStock / Getty Images Plus

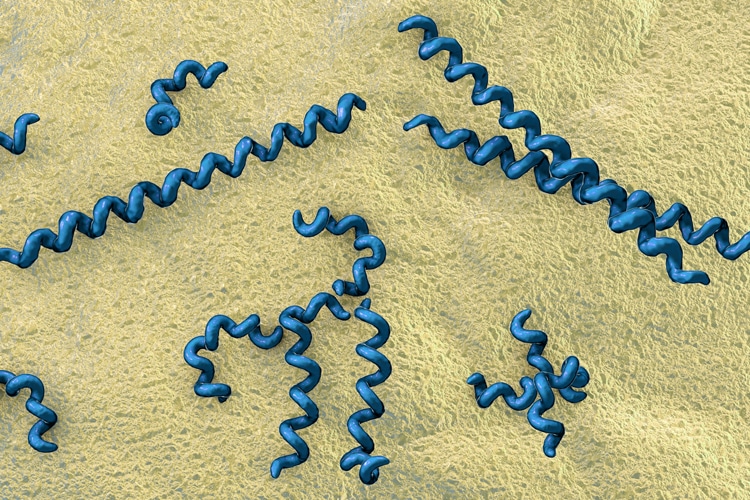
Etiology
Syphilis is caused by Treponema pallidum, a Gram-negative, microaerophilic, highly motile spirochete, characterized by its corkscrew appearance, and invisible by light microscopy due to its size of only 6 μm to 20 μm. Dark-field microscopy is the definitive method for syphilis diagnosis. Syphilis is transmitted by direct contact with primary or secondary lesions or by vertical transmission at any time during pregnancy.
Photo Credit: iLexx / iStock / Getty Images Plus
Clinical Presentation
Following inoculation, syphilis follows a well-described progression from primary to secondary stage of varied duration that can often overlap. Untreated, the disease will progress to the latent stage, which is symptomless, and can relapse to secondary manifestations and become infectious. About 15% to 40% of cases will progress to the tertiary stage years to decades later. Serious organ damage and death can occur in the tertiary stage.
Photo Credit: Shidlovski / iStock / Getty Images Plus
Signs and Symptoms
Syphilis is known as “the great imitator,” as it mimics signs and symptoms of various diseases and conditions, making clinical diagnosis difficult. Primary chancres and secondary oral lesions in primary and secondary syphilis are common and have nonspecific presentations. However, the disease may also follow an asymptomatic course: as many as 60% of patients with confirmed syphilis do not remember having any lesions, which may increase disease progress to the late stages and facilitate sexual and fetal transmission. The chance of developing the infection following exposure is estimated at 50%.
Photo Credit: Dr_Microbe / iStock / Getty Images Plus

Maternal and Fetal Impact
Congenital syphilis is the leading cause of stillbirth worldwide. Untreated maternal infections can result in fetal death (spontaneous abortion, stillbirth) in as many as 40% of cases. In the US, this proportion is much lower (5.5%) but represents missed opportunities for prevention of congenital syphilis. Time and stage of maternal infection during pregnancy influences the rate of fetal transmission and clinical outcomes. Infections earlier in pregnancy have a higher possibility of fetal and perinatal death and congenital infection than later in pregnancy, and disease in earlier stages has higher fetal transmission rates (70% to 100% in primary stage vs 10% in late latent stage). While dangerous, congenital syphilis is also preventable by prenatal screening and antibiotic treatment.
Photo Credit: kjekol / iStock / Getty Images Plus

Diagnosis
Diagnosis of current disease is based on the clinical findings, thorough evaluation of exposure history, and laboratory confirmation by direct or indirect T. pallidum detection methods. Visualization of bacteria in a sample obtained from a chancre or a secondary lesion by dark-field microscopy remains the definitive diagnostic method, although it is rarely performed. Other direct methods include polymerase chain reaction and direct fluorescent antibody assays; however, the diagnosis is most frequently confirmed by indirect serological methods determining the presence of antibodies to T. pallidum. A rapid point-of-care test used by clinicians in-office was approved by the US Food and Drug Administration (FDA) in 2014. Performed in 10 minutes using the patient’s whole blood (fingerstick), this test offers the convenience and speed for screening and initial testing that must be confirmed by a laboratory analysis in case of a positive result.
Photo Credit: Pornpak Khunatorn / iStock / Getty Images Plus
Treatment
Penicillin preparations (benzathine, aqueous procaine, aqueous crystalline) administered parenterally for various duration depending on the stage of the disease are the recommended treatment for syphilis. Selection of the agent depends on the location of bacteria and organs/systems involved, because some forms of penicillin are better at reaching the sequestered sites such as the central nervous system (neurosyphilis) or aqueous humor of the eye (ocular syphilis), or able to pass through the placental barrier to reach the fetus.
Photo Credit: CSA Images / Vetta
Oral Health Indications
Frequent occurrence of syphilitic ulcers in every stage in the oral cavity and perioral regions necessitates clinicians’ alertness. Using all diagnostic criteria for lesion assessment is crucial for differential diagnosis. Nonspecific appearance of primary oral chancres and secondary mucosal lesions can lead to misdiagnosis as fungal infections, aphthous stomatitis, attributed to previously diagnosed HIV infection, or simply blamed on stress. Inappropriate treatment with antifungal, antiretroviral, and steroid anti-inflammatory medications will not benefit the patient, and, in the case of corticosteroid therapy, can trigger exacerbation of infection.

Interesting article and information. However, why aren’t there any pictures of the lesions in this slideshow? I recently had a patient that presented with lesions on her tongue and it was later diagnosed as syphilis. Pictures would be very helpful.