Treating Periodontal Diseases with Laser Therapy
While several types of lasers are available to oral health professionals, the evidence supporting their use in treating periodontal diseases is mixed.
This course was published in the June 2014 issue and expires June 30, 2017. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify the types of lasers used in dentistry.
- Discuss the available evidence on the efficacy of laser therapy in dentistry.
- Explain the American Dental Association and American Academy of Periodontology statements on laser use in dentistry.
The word laser is an acronym for “light amplification by stimulated emission of radiation.” Lasers work by focusing a beam of light, or a single wavelength of photons, at a target. When the laser light contacts human tissue, it vaporizes the water content within the cell and creates a char layer. Lasers, depending on their wavelengths of light, can penetrate deep into human tissues. Used in medicine since the early 1960s,1 lasers were first applied in vivo to human teeth in 1965.2 Modern lasers are used in dentistry to cut and ablate tissue, and occasionally to “bio-stimulate” diseased tissues. The use of lasers to treat periodontal diseases has become an important topic in dentistry and periodontics, and much debate remains regarding the efficacy of lasers in this arena. The ability of certain lasers to efficiently cut soft tissue or ablate soft tissue lesions, however, is generally undisputed. This article will explore the types of lasers used by oral health professionals; the evidence-based research regarding laser therapy in the dental setting; and the American Dental Association’s (ADA) and American Academy of Periodontology’s (AAP) recommendations regarding their use in the treatment of periodontal diseases.
TYPES OF LASERS AND THEIR USES
The lasers with the longest track record in dentistry are diode, carbon dioxide (CO2), Nd:YAG, and Er:YAG lasers. Each type uses different materials in the laser medium to produce varying wavelengths of light. Diode lasers typically operate at a wavelength between 810 nm and 940 nm; CO2 lasers produce a wavelength of approximately 10,600 nm; Nd:YAG lasers operate at a wavelength around 1,064 nm; and Er:YAG lasers typically create a wavelength of 2,940 nm. Selecting an appropriate laser for the dental practice is based on the hard tissue and soft tissue applications most often performed.
The diode laser is most commonly used by general dentists to displace tissue around crown preparations (in place of packing retraction cord) and for hemostasis and excision of tissue. It is an alternative to electrosurgery and radiosurgery units in many dental practices.3 One advantage is the control the diode laser provides during tissue removal. The laser enables a precise application of light (heat) to the soft tissue. The resulting penetration is three-cell layers to five-cell layers thick.3 Diode lasers are typically less expensive and smaller than CO2 or Nd:YAG lasers. The diode laser energy can penetrate deeper into the tissue than a CO2 laser and is attracted to pigmentation (eg, melanin), which can be advantageous depending on the procedure. Lacking the power of the Nd:YAG and CO2 lasers, diode lasers are less efficient for certain soft tissue applications. Due to its wavelength and target molecules (eg, melanin), the diode laser is not effective at cutting hard tissues, such as teeth or bone. Overall, the diode laser is a cost-effective option for dentists who need a soft tissue laser for a variety of applications.
Another frequently used dental laser is the CO2, which is primarily utilized for cutting and coagulating soft tissue. The CO2 laser has relatively low surface penetration compared to the diode and Nd:YAG lasers. Its wavelength is highly absorbed by water, making it a good choice for the vaporization of superficial cells without damaging deeper tissues.
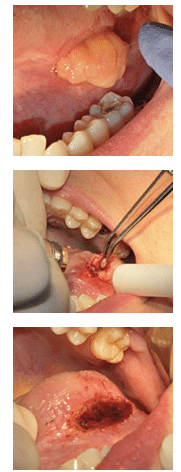
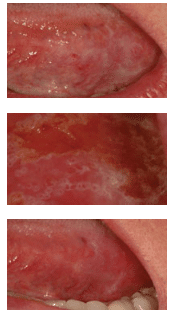
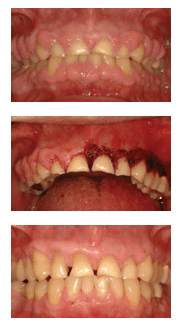
The CO2 laser can be used to excise various types of pathology (Figure 1A to Figure 1C). In addition to removing lesions, the CO2 laser can also be used on a low-power setting to remove the surface epithelial layer and ablate various dysplastic lesions (Figure 2A to Figure 2C). The ability to remove the surface epithelial layer may support the guided tissue regeneration (GTR) process by eliminating or blocking the epithelial downgrowth into the defect following periodontal surgery or scaling and root planing.4,5 Other uses for the CO2 laser include gingivectomy (Figure 3A to Figure 3C), crown lengthening, and implant exposure and uncovery. The CO2 laser is typically a much bigger unit than a diode laser and can accommodate different tips for various applications (eg, cutting vs sulcular debridement).
A popular soft tissue laser also used for the treatment of periodontal diseases is the Nd:YAG laser. It is able to penetrate more deeply into the tissue (2 mm to 3 mm) than the CO2 laser. A suggested protocol for using the Nd:YAG laser to treat periodontal defects involves administering local anesthesia, followed by passing the laser fiber-optic tip from the gingival margin to the base of the pocket to remove the diseased pocket epithelium and decontaminate the pocket. The teeth are then aggressively scaled and root planed with ultrasonic and hand instrumentation. An attempt is made to bluntly dissect any remaining periodontal fibers in order to stimulate vascular access to the periodontal wound. A second pass with the laser is performed from the apical extent of the periodontal defect to the gingival margin to form a fibrin coagulum and seal the pocket. No suturing is required. Adjusting any occlusal discrepancies is an important part of the protocol.6
The Er:YAG laser is primarily used in dentistry for hard tissue applications (eg, calculus removal, cavity preparation). This laser is not as popular as the other types because of its limited range of dental applications. In addition to removing calculus from roots of teeth, some clinicians use the Er:YAG laser to remove caries, perform cavity preparations, and etch teeth prior to placing composite restorations. One advantage of using the Er:YAG laser to remove caries lesions is that local anesthesia may not be required. Many clinicians have been reluctant to switch to Er:YAG lasers for cavity preparations because they can’t remove gold, amalgam, and ceramic restorations. The delivery system is more cumbersome than a traditional handpiece, and the laser therapy requires more time than conventional techniques.
LASER STUDIES
Beginning in the early 1990s, dentists began extensively evaluating the use of lasers to treat periodontal diseases. The first dental laser studies primarily looked at the efficacy of the CO2 laser. In 1992, a study by Rossmann et al4 looked at the possibility of using a CO2 laser to retard epithelial migration in monkeys through de-epithelialization of the gingival epithelium. On the test side, the oral epithelium was removed by CO2 laser irradiation. Sulcular epithelium was first seen on the test side at 14 days compared to epithelium becoming immediately present on the control side. For all specimens, there was a trend to less sulcular epithelium and more connective tissue attachment on the test side than on the control side. The authors concluded that the CO2 laser may be useful in retarding epithelial downgrowth compared to conventional flap surgery, and thereby enhance new connective tissue attachment. This was the first study to show that a laser could enhance connective tissue attachment when combined with a surgical procedure.4
Gold et al7 examined the effects of the Nd:YAG laser in removing diseased pocket lining epithelium in humans with moderate periodontitis. Twenty-four specimens of gingival tissue from six patients were examined histologically following irradiation with the Nd:YAG laser. Most sections (83%) exhibited complete removal of epithelium. The underlying connective tissue demonstrated no evidence of necrosis or carbonization. Morphologic features showed minimal change other than removal of pocket lining epithelium, compared to control sites. The authors concluded that the Nd:YAG laser can remove pocket lining epithelium in moderately deep pockets without damaging the underlying connective tissue.7
Neill and Mellonig8 combined scaling and root planing with epithelial elimination via the Nd:YAG laser. The authors reported on a double-blind, split-mouth study design that involved 10 human subjects randomly assigned to one of three treatments—scaling and root planing alone; Nd:YAG laser plus scaling and root planing; and control only (no scaling and root planing or laser treatment). The authors evaluated probing depths and clinical attachment levels, as well as several other parameters. The authors also performed microbial sampling at baseline, 1 week, 1 month, and 3 months post-scaling. The authors concluded that the laser therapy exerted longer lasting effects in altering the subgingival microflora than scaling and root planing alone. The clinical significance of these findings suggested that mechanical scaling and root planing alone may not be the most effective method of treatment in patients infected with Porphyromonas gingivalis or Prevotella intermedia. They also stated that there are several areas where the adjunctive use of the Nd:YAG laser may be more beneficial than scaling and root planing alone in nonsurgical therapy. These include the analgesic effect of the Nd:YAG laser, hemostatic effect, and antibacterial potential of laser energy.8
Israel et al9 published a case series describing an epithelial exclusion technique using the CO2 laser for the treatment of periodontal defects in humans. This paper presented three cases in which vertical bony defects were treated with flap reflection, debridement, grafting with demineralized freeze-dried bone allograft, and de-epithelialization of the outer aspect of the gingiva around the defect site. The patients were seen every 10 days for a repeat of the laser de-epithelialization procedure, for a total of four treatments. In all cases, significant osseous fill was obtained. The authors concluded that these cases demonstrate the ability to obtain clinical new attachment with bone fill among previously diseased sites, and that the concept of laser de-epithelialization as an adjunct to regenerative periodontal procedures may show better results than those obtained through conventional osseous grafting alone. The authors also stated that their results appear to be comparable to the results reported for GTR procedures with barrier membranes.9
The effectiveness of the Er:YAG laser in scaling and root planing compared to ultrasonic instrumentation was evaluated by Aoki et al10 in 2000. The authors evaluated 53 periodontally involved human extracted teeth with a band of subgingival calculus. The teeth were divided randomly into two groups for laser scaling and ultrasonic scaling. The features of the scaled surfaces were examined by histological and scanning electron microscope observations. The authors concluded that the Er:YAG laser provided calculus removal on a level equivalent to that provided by the ultrasonic scaler, without major thermal elevation. Macroscopically, the laser-treated root surface was somewhat rougher than the ultrasonically scaled root. However, the efficiency of the laser scaling was lower than that of the ultrasonic scaling.10 Additional studies by Frentzen et al11 and Schwarz et al12 support the Aoki study regarding the removal of calculus utilizing the Er:YAG laser.
Gregg and McCarthy13 published a case series that discussed the laser periodontal therapy (LPT) procedure developed specifically for the treatment of moderate to severe periodontitis. The end point of LPT was debridement of inflamed connective tissue, as well as removal of plaque and calculus adherent to the root surface. In addition, the bactericidal effects of the pulsed Nd:YAG laser was designed for reducing microbial pathogens within the periodontal pocket and surrounding tissues. In LPT, the tip of the Nd:YAG laser was used to trough around the tooth. This provided relaxation of the tissues for improved access and visualization of the diseased root surface and hemorrhage control. Following removal of the diseased soft tissue, a piezoelectric scaler, small curets, and root files were used to remove root surface accretions. A second pass with the laser finished debriding the pocket, provided hemostasis, and created a “soft clot.” The tissue was compressed against the root surface to close the pocket and stabilize the fibrin clot. If occlusal trauma was present, it was adjusted with a high-speed handpiece. The authors saw pocket reductions of approximately 70%. The authors concluded that it was possible to achieve similar results using other techniques, but the results in this case series were accomplished using a “closed” noninvasive method. This study helped generate additional interest for the treatment of severe periodontal diseases using a nonsurgical approach in combination with laser therapy.13
Yukna et al6 published histologic results in humans following a laser-assisted new attachment procedure (LANAP®) for the treatment of periodontal pockets. Six pairs of single-rooted teeth with advanced chronic periodontitis associated with subgingival calculus deposits were treated. A bur notch was placed within the pocket at the clinically and radiographically measured apical extent of the calculus. All teeth were scaled and root planed with ultrasonic and hand instrumentation. One of each pair of teeth received treatment of the inner pocket wall with the Nd:YAG laser to remove the pocket epithelium, and the test pockets were lased a second time to seal the pocket. After 3 months, all treated teeth were removed en bloc (meaning the tooth, surrounding soft tissue, and bone) for histologic evaluation. The results showed that the LANAP-treated teeth exhibited greater probing depth reductions and increased clinical probing attachment level gains than the control teeth. All LANAP-treated specimens showed new cementum and connective tissue attachment in and occasionally coronally to the notch, whereas five of the six control teeth had a long-junctional epithelium with no evidence of attachment or regeneration. The authors concluded that the concept of LANAP may be associated with cementum-mediated new connective tissue attachment and apparent periodontal regeneration of diseased root surfaces in humans.6
Lastly, Crespi et al14 compared, in a 15-year follow-up, the modified Widman flap to coronally advanced flap surgery combined with CO2 laser root conditioning. This is one of the few studies that examined the effects of laser therapy over an extended time period (more than 5 years). Each of the 25 study participants was treated using a split-mouth design. In one quadrant, the teeth received modified Widman flap surgery (control). On the other quadrant, after a full thickness flap was raised, a CO2 laser was used to irradiate the exposed root surfaces and soft tissue. The full-thickness flap was then repositioned coronally and sutured (test). Plaque index and gingival index scores, probing depths, and clinical attachment levels were monitored from baseline to the 15-year benchmark. At 15 years post-surgery, the test group experienced greater probing depth reductions and gains in clinical attachment levels than the control sites. The authors concluded that the CO2 laser therapy resulted in significant improvements compared to the modified Widman flap surgery.14
STATEMENTS ON LASERS IN DENTISTRYS
The most current ADA Council on Scientific Affairs Statement on Lasers in Dentistry reviews sulcular debridement, LANAP, reduction of bacteria levels in periodontal pockets, laser-facilitated wound healing, laser root planing, laser fluorescence, and other hard-tissue applications including endodontics.15
Regarding sulcular debridement, the ADA reports “the dental literature indicates that when used as an adjunct to meticulous root planing, mechanical or chemical curettage, lasers offer no consistent benefit beyond scaling and root planing alone with respect to gain of the periodontal attachment.” The ADA’s opinion regarding the LANAP procedure was mixed: “Although the Council is optimistic regarding the potential for lasers to enhance effectiveness in treating periodontitis, dentists should note that this study6 provides no more than pilot validation for this treatment concept. The Council therefore cautions clinicians to weigh the available evidence for LANAP when considering the options available for the treatment of periodontal diseases.” The ADA also found that “lasers, as a group, have inconsistently demonstrated the ability to reduce microorganisms within a periodontal pocket. It appears from the literature that mechanical root debridement remains a priority to attain improvements in clinical attachment levels.” Finally, the ADA Council on Scientific Affairs “considers the application of laser energy purely for the purpose of improved wound healing to be controversial and not well supported by clinical studies.”
The AAP Statement on the Efficacy of Lasers in the Nonsurgical Treatment of Inflammatory Periodontal Disease is consistent with the ADA’s findings. The AAP states “there is minimal evidence to support the use of lasers for the purpose of subgingival debridement, either as a monotherapy or adjunctive to scaling and root planing.” Additionally, the AAP found that “current evidence shows lasers, as a group, to be unpredictable and inconsistent in their ability to reduce subgingival microbial loads beyond that achieved by scaling and root planing alone.”16
At the current time, neither the ADA nor AAP feel there is sufficient clinical evidence to support the use of lasers as a monotherapy in the treatment of periodontal diseases. More clinical research is required before lasers become the standard of care for treating periodontal defects and disease. Even though many clinical studies cite improvement in periodontal diseases following treatment with either the CO2 or Nd:YAG laser, the sample sizes were small and many lack long-term follow-up. Additional prospective, long-term, randomized, controlled clinical trials are required to ascertain the efficacy of treating periodontal diseases with laser therapy.
In some states, dental hygienists are allowed to use lasers as an adjunct to scaling and root planing, to reduce pocket bacterial loads, and to aid with hemostasis. Dental hygienists should check with their state boards prior to treating patients with lasers to ensure they are abiding by their scope of practice.
SUMMARY
As presented in the previous studies and meta-analysis performed by the ADA and AAP, lasers have not reached the level of efficacy of other traditional periodontal therapies (scaling and root planing or GTR) for the treatment of periodontitis. Most studies show that lasers as a monotherapy are not equivalent to existing techniques and may best be used in the future as an adjunctive aid or in combination with other treatment modalities. More research may lead to lasers becoming a key instrument in the general dentist’s, periodontist’s, and dental hygienist’s armamentarium for the future treatment of periodontal diseases.
While the current statements by the ADA and AAP caution clinicians about the efficacy of laser therapy in the treatment of periodontal diseases, there are many other applications for lasers in dentistry. The ability to precisely cut and coagulate tissues for a variety of soft tissue procedures—including gingivectomy, gingivoplasty, biopsy of soft tissue lesions, ablation of precancerous lesions, crown lengthening, vestibuloplasty, and frenectomies—make the laser an excellent tool for dental surgeons. As more research becomes available, it is likely lasers will play a bigger role in the day-to-day provision of dental care.
REFERENCES
- Maiman TH. Stimulated optical radiation in ruby. Nature. 1960;187:493–494
- Goldman L, Gray JA, Goldman J, Goldman B, Meyer R. Effect of laser beam impacts on teeth. J Am Dent Assoc. 1965;70:601–606
- Christensen GJ. Soft-tissue cutting with laser versus electrosurgery. J Am Dent Assoc. 2008;139:981–984.
- Rossmann J, McQuade M, Turunen DE. Retardation of epithelial migration in monkeys using a carbon dioxide laser: an animal study. J Periodontol. 1992;63:902–907.
- 8Pope JD, Rossmann JA, Kerns DG, Beach MM, Cipher DJ. Use of the carbon dioxide laser as an adjunct to scaling and root planing for clinical new attachment: a case series. Clinical Advances in Periodontics. April 16, 2013. Epub ahead of print.
- Yukna RA, Carr RL, Evans GH. Histologic evaluation of an Nd:YAG laser-assisted new attachment procedure in humans. Int J Periodontics Restorative Dent. 2007;27:577–587.
- Gold SI, Vilardi MA. Pulsed laser beam effects on gingiva. J Clin Periodontol. 1994;21:391–396.
- Neill M, Mellonig JT. Clinical efficacy of the Nd:YAG laser for combination periodontitis therapy. Pract Periodontics Aesthet Dent. 1997;9(Suppl 6):1–5.
- Israel M, Rossmann JA. An epithelial exclusion technique using the CO2 laser for the treatment of periodontal defects. Compend Contin Educ Dent. 1998;19:86–95.
- Aoki A, Miura M, Akiyama F, et al. In vitro evaluation of Er:YAG laser scaling of subgingival calculus in comparison with ultrasonic scaling. J Periodontol Res. 2000;35:266–277.
- Frentzen M, Braun A, Aniol D. Er:YAG laser scaling of diseased root surfaces. J Periodontol. 2002;73:524–530.
- Schwarz F, Sculean A, Berakdar M, Georg T, Reich E, Becker J. Periodontal treatment with an Er:YAG laser or scaling and root planing. A 2-year follow-up split-mouth study. J Periodontol. 2003;74:590–596.
- Gregg RH 2nd, McCarthy D. Laser periodontal therapy for bone regeneration. Dent Today. 2002;21:54–59.
- Crespi R, Gherlone E, Romanos G. Comparison of modified widman and coronally advanced flap surgery combined with CO2 laser root irradiation in periodontal therapy: a 15-year follow-up. Int J Periodontics Restorative Dent. 2011;31:641–651.
- American Dental Association. ADA Council on Scientific Affairs: Statement on Lasers in Dentistry. Available at: ada.org/en/about-the-ada/ada-positions-policies-and-statements/statement-on-lasers-in-dentistry. Accessed May 19, 2014.
- American Academy of Periodontology statement on the efficacy of lasers in the non-surgical treatment of inflammatory periodontal disease. J Periodontol. 2011;82:513–514.
From Dimensions of Dental Hygiene. June 2014;12(6):53–56,59.
