
The Relationship Between Obesity and Periodontitis
Addressing this possible link in the treatment of overweight and obese patients.
This course was published in the July 2009 issue and expires July 31, 2012. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the relationship between obesity and periodontitis.
- Describe the effects of periodontal therapy among patients who have diabetes.
- Discuss the association between measures of obesity and periodontitis.
- Identify clinical strategies that can be used to reduce the risk of periodontal diseases for obese patients.
In part one of this series, the role of cytokine production and inflammation associated with obesity was explored. Emerging research proposes an association between obesity and periodontitis, although the exact nature of this relationship is not known. It is thought that cytokines secreted by adipose tissue, known as adipokines, play an important role in modulating periodontal disease.1 Periodontitis is a chronic inflammatory condition, and individuals who have the disease may experience as high as a 10-fold increase in the expression of both local and systemic pro-inflammatory cytokines including tumor necrosis factor alpha (TNF?) and interleukin-6 (IL-6).2 Pathogens and their endotoxins, notably lipopolysaccharides (LPS), as well as inflammatory cytokines, trigger the synthesis of acute phase proteins, which help maintain the inflammatory state.
In the obese individual, inflammation associated with bacterial challenge and adipose tissue combined with the production of acute phase proteins results in altered metabolic processes, including elevated triglycerides and cholesterol, insulin resistance (IR), and metabolic syndrome (MS). These outcomes predispose the obese individual who has periodontitis to cardiovascular disease and type 2 diabetes.3,4 Conversely, by-products from altered metabolism, known as advanced glycation endproducts (AGE) observed in individuals who have IR and type 2 diabetes, trigger cytokine production. This may promote periodontitis in susceptible patients and/or make control of diabetes more difficult.5,6
RESEARCH RESULTS
Ongoing research is examining the effect of periodontal therapy on reducing circulating cytokines and systemic disease. Periodontal treatment has been shown to improve glycemic control among patients who have type 2 diabetes.7-9 In one study, weekly administration of locally applied minocycline into periodontal pockets during a 1-month period improved glycemic control and reduced serum TNF? for patients who had type 2 diabetes.10 In another small trial, no differences in clinical periodontal outcomes or glycemic control were observed at 3 months among patients who had diabetes following full mouth scaling and root planing.11 In a 5-year longitudinal trial monitoring periodontitis recurrence, results revealed that subjects who had diabetes as well as those who did not have diabetes were able to maintain a healthy periodontal status after receiving nonsurgical treatment for moderate to advanced forms of periodontitis, and that frequency of disease recurrence was similar for both groups.12
Among obese subjects aged 13 years to 24 years who had a body mass index (BMI) ?40, a statistically significant correlation existed between the level of TNF? in gingival crevicular fluid (GCF) and BMI, compared to subjects who had a BMI <40. This positive correlation was also found among obese subjects (BMI >40) who had no periodontal pockets, which suggests that TNF? in GCF is associated with a systemic effect of obesity.13 Systemic effects have also been observed in mice. The presence of periodontitis accelerated the onset of severe IR and impaired glucose control, and infection with Porphyromonas gingivalis in diet-induced obesity produced a significantly higher level of alveolar bone loss.14,15
| Glossary of Terms |
| Advanced glycation end-products: The result of a chain of chemical reactions after an initial glycation reaction.
Body mass index: A measure of body fat that is the ratio of the weight of the body in kilograms to the square of its height in meters; also called the Quetelet index. Cytokines: Immunoregulatory proteins, such as interleukin (IL-6), tumor necrosis factor (TNF?), and interferon, that are secreted by cells. Insulin resistance: Reduced sensitivity to insulin by the body’s insulin-dependent processes (as glucose uptake, lipolysis, and inhibition of glucose production by the liver) that results in lowered activity of these processes or an increase in insulin production or both, and that is typical of type 2 diabetes but often occurs in the absence of diabetes. Lipopolysaccharide: A large molecule consisting of lipids and sugars joined by chemical bonds. Metabolic syndrome: A syndrome marked by the presence of usually three or more of a group of factors (such as high blood pressure, abdominal obesity, high triglyceride levels, low HDL levels, and high fasting levels of blood sugar) that are linked to an increased risk of cardiovascular disease and type 2 diabetes—also called insulin resistance syndrome, syndrome X. Porphyromonas gingivalis: a non motile, gramnegative, rod-shaped, anaerobic pathogenic bacterium found in the oral cavity, where it is implicated in certain forms of periodontal disease as well as the upper gastrointestinal tract, respiratory tract, and in the colon. Merriam-Webster Online Medical Dictionary. Available at: www.merriam-webster.com. Accessed June 11, 2009. |
PERIODONTAL RISK FACTORS AND OBESITY
Numerous studies show that BMI, waist circumference (WC), and waist to hip ratio (WHR) are significantly associated with periodontitis.16-22 Abdominal obesity is also positively associated with periodontal pocketing and clinical attachment loss.20 Risk for periodontitis increases with increased BMI and WC.21,22 While high BMI early in life did not predict periodontitis later in life, subjects who experienced large increases in weight during adulthood were at increased risk for poor periodontal condition.22
Smoking and obesity are independent risk factors for periodontitis, and both show a doseresponse relationship to periodontal disease risk.23 Radiographic periodontal bone loss is strongly associated with obesity among females and among nonsmokers.24 Obese female nonsmokers are 3.4 times more likely to have periodontitis than those who have a normal BMI.25 BMI and periodontitis are positively associated among the nonsmoking, nondiabetic population aged 30 years to 49 years.26 This relationship may be bidirectional. Nonsmokers who have elevated periodontal screening and recording (PSR) codes are at a significantly higher risk for being overweight or obese.27
A national study of adults aged 65 years and older in Great Britain found that edentulous individuals were more likely to be underweight, and dentate individuals who had less than 21 natural teeth were more than three times more likely to be obese compared to those who had 21 to 32 teeth. The study concluded that people who had 20 or more teeth were more likely to have a normal BMI.28 Conversely, in a study of predominantly older male veterans, functional edentulism and obesity were both significantly associated with type 2 diabetes.29 Additional research is needed to assess how the number of teeth influences diet and function and the relationship to obesity.
IMPLICATIONS FOR PRACTICE
 Dental professionals will encounter more overweight and obese patients who require additional assessment of risks associated with their metabolic condition. A careful review of the medical history is warranted, including assessment of changes in weight, cardiovascular status, IR, MS, diabetes status, and the presence of chronic inflammatory conditions. A careful and thorough periodontal assessment should be performed at each visit, recognizing that overweight/ obese patients may present with increased risk for periodontitis, and may benefit from nonsurgical periodontal therapy and frequent maintenance intervals to reduce this risk. A consultation with a periodontist may be indicated.
Dental professionals will encounter more overweight and obese patients who require additional assessment of risks associated with their metabolic condition. A careful review of the medical history is warranted, including assessment of changes in weight, cardiovascular status, IR, MS, diabetes status, and the presence of chronic inflammatory conditions. A careful and thorough periodontal assessment should be performed at each visit, recognizing that overweight/ obese patients may present with increased risk for periodontitis, and may benefit from nonsurgical periodontal therapy and frequent maintenance intervals to reduce this risk. A consultation with a periodontist may be indicated.
Nutritional counseling is an essential component of the oral health treatment plan, including careful assessment of food choices, snacking behaviors, and frequency of exposure to carbohydrates. A study of 402 subjects found that overweight and obese adolescents had greater interproximal caries compared to adolescents who had normal or low weight. The same study found that snacking behaviors that occur as early as 1 year of age can influence caries prevalence at age 15. One-year-old subjects who ate more than three servings per day of high sugar foods, including sweets and soft drinks, had significantly more caries at age 15 than those who consumed fewer than three of these snacks per day.30 Referral to a registered dietician should be considered for overweight/ obese individuals who present with higher risk for oral diseases.
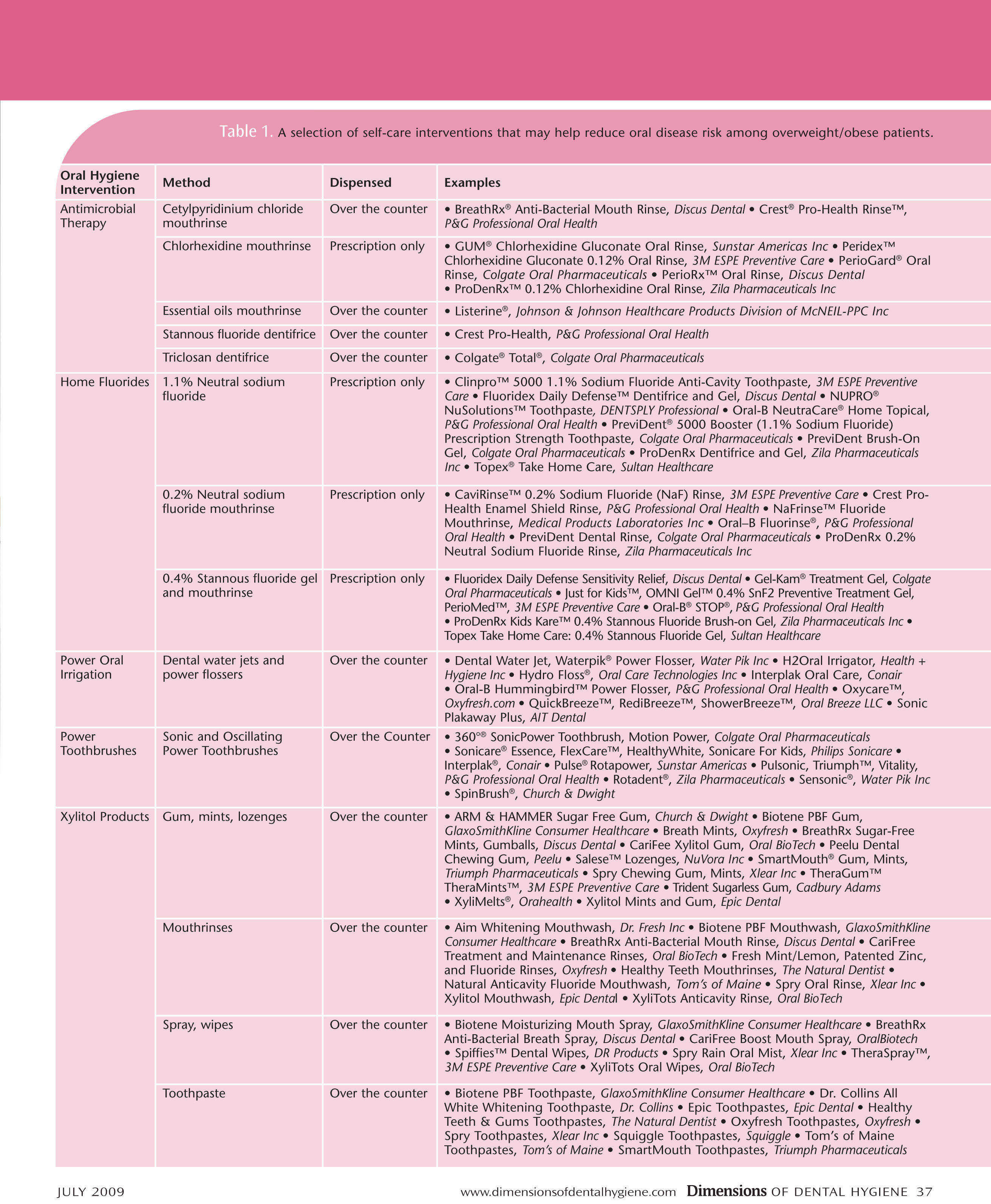
Clinicians should counsel their patients about oral hygiene products and practices that can reduce the bacterial challenge and resultant inflammation of the periodontal tissues, including antimicrobial therapy. Table 1 lists some strategies for patients to reduce the bacterial challenge.
Patient education should include a discussion about the health risks associated with overweight and obesity. Patient education should include a discussion about the health risks associated with overweight and obesity, advocating proactive recommendations for lifestyle modification and behavioral changes that are realistic for the patient to achieve. Dental professionals can partner with their patients for goal-setting and monitoring progress, and serve as important resources for information, guidance, encouragement, and support.
REFERENCES
- Kershaw EE, Flier JS. Adipose tissue as an endocrine organ. J Clin Endocrinol Metab. 2004;89:2548-2556.
- Beck J, Garcia R, Heiss G, Vokonas PS, Offenbacher S. Periodontal disease and cardiovascular disease. J Periodontol. 1996;67 (10 Suppl):1123-1137.
- Beck JD, Offenbacher S. Systemic effects of periodontitis: epidemiology of periodontal disease and cardiovascular disease. J Periodontol. 2005;76(11 Suppl):2089-2100.
- Saito T, Shimazaki Y, Koga T, Tsuzuki M, Ohshima A. Relationship between upper body obesity and periodontitis. J Dent Res. 2001;80:1631-1636.
- Genco RJ, Grossi SG, Ho A, Nishimura F, Murayama Y. A proposed model linking inflammation to obesity, diabetes, and periodontal infections. J Periodontol. 2005;76(11 Suppl):2075-2084.
- Grossi SG, Genco RJ. Periodontal disease and diabetes mellitus: a two-way relationship. Ann Periodontol. 1998;3:51-61.
- Kiran M, Arpak N, Unsal E, Erdo?an MF. The effect of improved periodontal health on metabolic control in type 2 diabetes mellitus. J Clin Periodontol. 2005;32:266-272.
- Makiura N, Ojima M, Kou Y, et al. Relationship of Porphyromonas gingivalis with glycemic level in patients with type 2 diabetes following periodontal treatment. Oral Microbiol Immunol. 2008;23:348-351.
- Stewart JE, Wager KA, Friedlander AH, Zadeh HH. The effect of periodontal treatment on glycemic control in patients with type 2 diabetes mellitus. J Clin Periodontol. 2001;28:306-310.
- Iwamoto Y, Nishimura F, Nakagawa M, et al. The effect of antimicrobial periodontal treatment on circulating tumor necrosis factor-alpha and glycated hemoglobin level in patients with type 2 diabetes. J Periodontol. 2001;72:774-778.
- da Cruz GA, de Toledo S, Sallum EA, et al. Clinical and laboratory evaluations of non-surgical periodontal treatment in subjects with diabetes mellitus. J Periodontol. 2008;79:1150-1157.
- Westfelt E, Rylander H, Blohmé G, Jonasson P, Lindhe J. The effect of periodontal therapy in diabetics. Results after 5 years. J Clin Periodontol. 1996;23:92-100.
- Lundin M, Yucel-Lindberg T, Dahllöf G, Marcus C, Modéer T. Correlation between TNF alpha in gingival crevicular fluid and body mass index in obese subjects. Acta Odontol Scan. 2004;62:273-277.
- Watanabe K, Petro BJ, Shlimon AE, Unterman TG. Effect of periodontitis on insulin resistance and the onset of type 2 diabetes mellitus in Zucker diabetic fatty rats. J Periodontol. 2008;79:1208-1216.
- Amar S, Zhou Q, Shaik-Dasthagirisaheb Y, Leeman S. Diet-induced obesity in mice causes changes in immune responses and bone loss manifested by bacterial challenge. Proc Natl Acad Sci USA. 2007;104:20466-20471.
- Saito T, Shimazaki Y, Kiyohara Y, et al. Relationship between obesity, glucose tolerance, and periodontal diseases in Japanese women: the Hisayama study. J Periodontal Res. 2005;40:346-353.
- Wood N, Johnson RB, Streckfus CF. Comparison of body composition and periodontal disease using nutritional assessment techniques: Third National Health and Nutrition Examination Survey (NHANES III). J Clin Periodontol. 2003;30:321-327.
- Reeves AF, Rees JM, Schiff M, Hujoel P. Total body weight and waist circumference associated with chronic periodontitis among adolescents in the United States. Arch Pediatr Adolesc Med. 2006;160:894-899.
- Khader YS, Bawadi HA, Haroun TF, Alomari M, Tayyem RF. The association between periodontal disease and obesity among adults in Jordan. J Clin Periodontol. 2009;36:18-24.
- Sarlati F, Akhondi N, Ettehad T, Neyestani T, Kamali Z. Relationship between obesity and periodontal status in a sample of young Iranian adults. Int Dent J. 2008;58:36-40.
- Ekuni D, Yamamoto T, Koyama R, Tsuneishi M, Naito K, Tobe K. Relationship between body mass index and periodontitis in young Japanese adults. J Periodontal Res. 2008;43:417-421.
- Linden G, Patterson C, Evans A, Kee F. Obesity and periodontitis in 60-70-year-old men. J Clin Periodontol. 2007;34:461-466.
- Nishida N, Tanaka M, Hayashi N, et al. Determination of smoking and obesity as periodontitis risks using the classification and regression tree method. J Periodontol. 2005;76:923-928.
- Alabdulkarim M, Bissada N, Al-Zahrani M, Ficara A, Siegel B. Alveolar bone loss in obese subjects. J Int Acad Periodontol. 2005;7:34-38.
- Dalla Vecchia CF, Susin C, Rösing CK, Oppermann RV, Albandar JM. Overweight and obesity as risk indicators for periodontitis in adults. J Periodontol. 2005;76:1721-1728.
- Ylöstalo P, Suominen-Taipale L, Reunanen A, Knuuttila M. Association between body weight and periodontal infection. J Clin Periodontol. 2008;35:297-304.
- Wood N, Johnson RB. The relationship between smoking history, periodontal screening and recording (PSR) codes and overweight/obesity in a Mississippi dental school population. Oral Health Prev Dent. 2008;6:67-74.
- Sheiham A, Steele JG, Marcenes W, Finch S, Walls AW. The relationship between oral health status and Body Mass Index among older people: a national survey of older people in Great Britain. Br Dent J. 2002;192:703-706.
- Cleary TJ, Hutton JE. An assessment of the association between functional edentulism, obesity, and NIDDM. Diabetes Care. 1995;18:1007-1009.
- Alm A, Fahraeus C, Wendt LK, Koch G, Andersson-Gäre B, Birkhed D. Body adiposity status in teenagers and snacking habits in early childhood in relation to approximal caries at 15 years of age. Int J Paediatr Dent. 2008;18:189-196.
From Dimensions of Dental Hygiene. July 2009; 7(7): 36-39.
