The Complexity of Addiction
How to address the oral health needs of patients experiencing drug abuse and addiction problems.
This course was published in the April 2011 issue and expires April 2014. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the principles of drug addiction and treatment.
- List the most common physical signs of drug abuse and addiction.
- Detail the typical oral manifestations of drug abuse and addiction.
- Identify the most frequently abused illicit drugs, their route of administration, and their resulting effects.
More than 19 million Americans over the age of 12 years have engaged in illicit drug use, according to the Department of Health and Human Services.1 Drug abuse and “addiction” for defining the overall behavioral syndrome and applies the same criteria to all types of substances regardless of their classification.6 It is important for dental health providers to be aware of the principles regarding drug addiction and treatment. These principles have been established by the National Institute of Drug Abuse and are presented in Table 1.7
THEORY OF ADDICTION
Drug addiction is neither a weakness in character nor a moral issue. The most widely accepted theory of drug addiction is the disease model, which defines drug addiction as a brain disease over which the individual has no control.2,4,5 Some psychoactive drugs of abuse (marijuana, cocaine, and methamphetamine) change the structures and/or functions of the brain.2,4
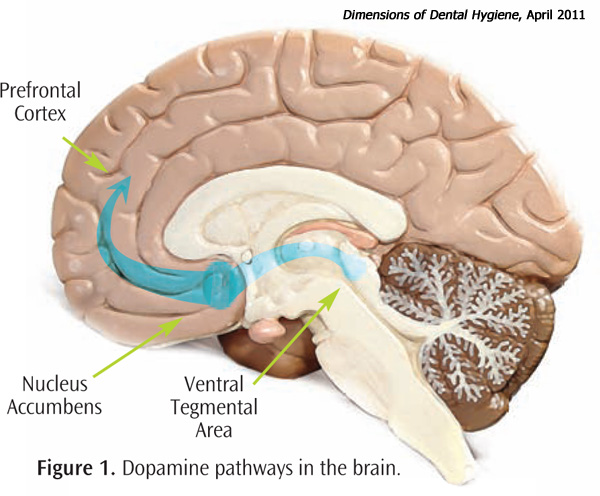 Addictive drugs directly or indirectly activate the brain’s reward system by markedly increasing the release of dopamine. Dopamine is a neurotransmitter that regulates emotion, cognition, movement, motivation, and pleasure. Overstimulation of the brain reward pathway with dopamine produces intense euphoric effects and sensations that are further reinforced or strengthened by continued drug use.3,4,5 Figure 1 illustrates the pathways of dopamine in the brain.
Addictive drugs directly or indirectly activate the brain’s reward system by markedly increasing the release of dopamine. Dopamine is a neurotransmitter that regulates emotion, cognition, movement, motivation, and pleasure. Overstimulation of the brain reward pathway with dopamine produces intense euphoric effects and sensations that are further reinforced or strengthened by continued drug use.3,4,5 Figure 1 illustrates the pathways of dopamine in the brain.
PHYSICAL AND ORAL MANIFESTATIONS
Abuse occurs with legal drugs, such as alcohol, nicotine, and prescription drugs, as well as illicit drugs, such as marijuana, cocaine, heroin, and hallucinogens.2 Table 2 provides information about some of the most commonly abused illicit drugs.8 Drug abusers often present with telltale signs of their addiction. Some symptoms will not be determinable during a dental appointment, such as loss of appetite and sleeplessness, but others may be quite noticeable even during routine examinations. Table 3 lists the most obvious physical signs of drug abuse.4,9-11
 |
 |
Oral problems of drug abuse are complex and include not only the direct effects of the drug but also the results of poor dietary and oral hygiene habits.11-14 Table 4 lists some common oral manifestations of drug abuse. Drug abuse may cause suppression of the immune system, making patients more susceptible to other health problems. Diminished self-esteem, depression, and lack of motivation are also signs of drug abuse and may negatively affect patients’ ability to adequately perform oral hygiene and regularly visit their dental provider.15
Diminished financial status may preclude dental treatment. When treatment becomes possible, the only financially viable alternative may be tooth extraction. Addicts may also use dental pain as a way to legally obtain pain-relieving narcotic prescriptions or their use of mood-altering altering substances may diminish the pain of their oral health problems.15
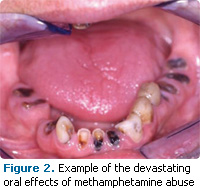
Xerostomia is often a side effect of opiates, amphetamines, barbiturates, hallucinogens, marijuana, and alcohol. The resulting decreased salivary flow makes users much more susceptible to dental caries and periodontal diseases. Furthermore, chemically dependent patients often crave sugar, which leads to the consumption of large quantities of sweetened carbonated beverages, thereby increasing enamel erosion by decreasing salivary pH (Figure 2).16,17 Drug addicts may also be at a higher risk of bruxism, dentin hypersensitivity, and necrotizing ulcerative gingivitis.18-20
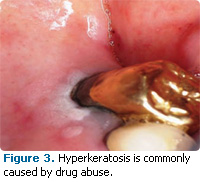
Drug and alcohol/tobacco users have a higher incidence of oral lesions, oral candidiasis, oral ulcerations, and gingival laceration. Leukoplakia, leukoedema, hyperkeratosis (Figure 3), angular cheilitis, and stomatitis are more common among users. The use and abuse of alcohol and tobacco also greatly increases the risk of oral cancer.17,21
 |
 |
 |
DENTAL HYGIENE CARE
Past and present drug use history should be included on all patient medical history forms. For those in treatment, tandem treatment planning should be conducted with appropriate medical providers. For patients suspected of drug abuse or addiction, dental professionals should encourage patients to see their primary physicians or refer to addiction treatment specialists. It is imperative that patients receive treatment due to the degenerative effects of continued drug use in addition to increased risk of hepatitis and human immunodeficiency virus infection, and infective endocarditis.15
Due to the development of cross tolerance (defined as decreased pharmacological effects of a drug due to previous exposure to other similar drugs), chemically-dependent patients may show a reduced response to local anesthetics.2,22 Therefore, the patient may require more local anesthesia during a dental procedure, though the maximum amount of local anesthesia that can be administered remains unchanged.23 Since chemically dependent patients are at increased risk of cardiovascular complications with epinephrine, a local anesthetic preparation without a vasoconstrictor, such as 3% mepivacaine, can be used. Nitrous oxide analgesia should be avoided in chemically-dependent patients because it is a mood-altering drug and may increase the potential for further drug abuse by creating the same or similar pleasurable sensations.4,7 Post-operative pain strategies should only include aspirin, acetaminophen, or nonsteroidal anti-inflammatory agents.15 However, these medications are contraindicated in patients with liver dysfunction, gastrointestinal disorders, or blood dyscrasia.15
TABLE 4. ORAL MANIFESTATIONS OF SUBSTANCE ABUSE.
- Angular cheilitis
- Bruxism
- Gingival laceration
- Glossitis
- Leukoplakia
- Missing teeth
- Oral candidiasis
- Oral lesions
- Oral ulcerations
- Periodontal diseases
- Rampant dental caries
- Squamous cell carcinoma
In patients with identified drug use or addiction, strategies for dental disease treatment and prevention can be determined. For patients experiencing xerostomia, mouthrinses containing alcohol should be avoided and saliva substitutes and oral lubricant sprays can be recommended. Effective oral hygiene must be stressed as well as consistent exposure to fluoride to reduce caries risk. The topical application of fluoride via varnish may be indicated. For those at high risk of xerostomia, high doses of fluoride or the use of chlorhexidine mouthrinses may be the best treatment options.24
Likewise, diet modification is another strategy to assist chemically-dependent patients. Dietary changes such as eliminating carbonated beverages, avoiding highly acidic foods, and limiting overall sugar consumption will improve oral health. Dental hygienists can assist patients in identifying healthy food and beverages.
SUMMARY
Patients experiencing drug addiction can be treated in the general dental office. Understanding the symptoms of drug addiction and resulting health effects in addition to cooperation with other medical team members can ensure the smooth and successful provision of oral health services.
REFERENCES
- Results from the 2007 National Survey on Drug Use and Health: National Findings. Rockville, Md: Department of Health and Human Services; 2008.
- Hart CL, Ksir C, Ray Oakley. Drugs, Society, and Human Behavior. 13th ed. New York: McGraw- Hill Companies Inc; 2009.
- Fung EY, Giannini P. Implications of drug dependence on dental patient management. Gen Dent. 2010;58:236-241.
- National Institute on Drug Abuse. Drugs, Brains, and Behavior—the Science of Addiction. Washington, DC: National Institutes of Health; 2010:236-241.
- Nestler EJ, Malenka RC. The addicted brain. Sci Am. 2004;290:78-85.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed. Washington DC: American Psychiatric Association; 2000.
- National Institute on Drug Abuse. Principles of Drug Addiction Treatment. Washington, DC: National Institutes of Health; 2009:09-4180.
- National Institute on Drug Abuse. Commonly Abused Drugs. Available at: www.drugabuse.gov/DrugPages/DrugsofAbuse.html. Accessed March 17, 2011.
- Helms RA, Quan DJ, Herfindal ET, Gourley DR. Textbook of Therapeutics Drug and Disease Management. 8th ed. Philadelphia: Lippincott Williams and Wilkins; 2006.
- Byrd PB. Do you know if your patients, coworkers, friends, family, or you have an addiction? J Dent Hyg. 2001;75:65-75.
- American Council for Drug Education. Signs and Symptoms of Drug Abuse. Available at: www.acde.org/parent/signs.htm. Accessed March 17, 2011.
- Lee CY, Mohammadi H, Dixon RA. Medical and dental implications of cocaine abuse. J Oral Maxillofac Surg. 1991;49:290-293.
- Pallasch TJ, Joseph CE. Oral manifestations of drug abuse. J Psychoactive Drugs. 1987;19:375- 377.
- Curtis E. Meth mouth: a review of methamphetamine abuse and its oral manifestations. Gen Dent. 2006;54:125-129.
- Rees TD. Oral effects of drug abuse. Crit Rev Oral Biol Med. 1992;3:163-184.
- Morio KA, Marshall TA, Qian F, Organ TA. Comparing diet, oral hygiene, and caries status of adult methamphetamine users and nonusers: a pilot study. J Am Dent Assoc. 2008;139:171-176.
- Bassiouny MA, Yang J. Influence of drinking patterns of carbonated beverages on dental erosion. Gen Dent. 2005;53:205-210.
- McGrath C, Chan B. Oral health sensations associated with illicit drug abuse. Br Dent J. 2005;198:159-162.
- Chi D, Milgrom P. The oral health of homeless adolescents and young adults and determinants of oral health: preliminary findings. Spec Care Dentist. 2008;28:237-242.
- Boyce N. Health warnings for people who use heroin. Lancet. 2011;377:193-194.
- Shetty V, Mooney LJ, Zigler CM, Belin TR, Murphy D, Rawson R. The relationship between methamphetamine use and increased dental disease. J Am Dent Assoc. 2010;141:307-318.
- Friedlander AH, Mills MJ. The dental management of the drug-dependent patient. Oral Surg Oral Med Oral Pathol. 1985;60:489- 492.
- The ADA/PDR Guide to Dental Therapeutics. 4th ed. Chicago: American Dental Association; 2006.
- Friedman PK, Isfeld D. Tips for treating xerostomia. Dimensions of Dental Hygiene. 2011;9(1):50-53.
From Dimensions of Dental Hygiene. April 2011; 9(4): 76-81.
