
Recognize the Signs
Oral health professionals are in an ideal position to identify and report suspected cases of child abuse and neglect.
This course was published in the February 2014 issue and expires 2/28/17. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the incidence and etiology of child abuse and
neglect. - Define the four types of child abuse and neglect.
- Identify the signs and symptoms manifesting in the four types of abuse and neglect.
- Discuss the protocol for reporting incidents of suspected child abuse.
Most cases of physical abuse present with injuries to the head, neck, and facial regions.2 Moreover, intraoral injuries are prevalent in many child abuse cases,2 most of which can be readily identified by intraoral and extraoral examination.2,4,5 Oralhealth professionals are well positioned to identify and report suspected cases of child abuse and neglect, and to act on behalf of children affected by such situations.
MANDATORY REPORTERS
Dentists in all 50 states are mandated to report suspected maltreatment.6–8 In all but a few states, dental hygienists are also required to report suspected child abuse and neglect.8 Each state has its own laws on reporting abuse and neglect involving children and older adults, as well as laws on who is mandated to report them.9 In general, mandatory reporters of abuse include those who, in their professional capacity, suspect a child is being abused or neglected.8 A professional is anyone who comes in contact with the alleged victim during the course of his or her job (eg, nurses, teachers, dental hygienists).3 The Child Welfare Information Gateway has the complete list of each state’s mandatory reporting requirements.8
Reporters of child abuse and neglect are immune from criminal liability, provided they have acted in accordance with state law and in good faith to protect the child.1,9,10 Dental professionals are not required to prove abuse or neglect, just to report suspected cases.4,9
INCIDENCE
Child abuse occurs at every socioeconomic level, across ethnic and cultural lines, within all religions, and at all levels of education.1 In 2012, Child Protective Services received 3.8 million referrals alleging maltreatment.3 Of these referrals, 20% were substantiated as victims of abuse or neglect.3 In 2012, a nationally estimated 1,640 children died from abuse and neglect3—an average of four fatalities each day. Children younger than 3 account for 70% of all child fatalities.11 The majority of victims are white (44.0%), Hispanic (21.8%), and black (21.0%).3 While research findings indicate that approximately 65% of physical injury resulting from abuse involves the head and neck region,12 only a small number of cases are reported by oral health professionals.6,9
ETIOLOGY
The National Child Abuse and Neglect Data System defines an abuser as “a person who has been determined to have caused or knowingly allowed the maltreatment of a child.”3 Most perpetrators are between 20 and 40, and approximately 80% of child abusers are parents.3
TYPES OF ABUSE
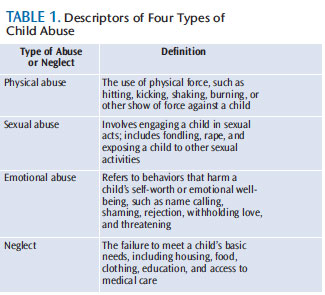
Child abuse and types of maltreatment are defined by each state via statute and policy, and apply to children younger than 18. There are four types of abuse: physical, sexual, emotional, and neglect (Table 1).1,13 While some physical signs are readily identified, others are assessed by looking at patterns. A bilateral injury to the face, for instance, is unlikely to be accidental. Referred to as a pathognomonic,a bilateral facial injury is seen as an automatic indicator of abuse.4,5 Patterned injuries (from a hand or in the patterned shape of an object used in injury) should also encourage oral health professionals to further investigate the possibility of abuse.4
PHYSICAL ABUSE
Oral health professionals may be the first to identify signs of abuse specific to the head, neck, and facial regions.8 Each type of abuse presents with a unique set of signs and symptoms. Therefore, clinicians must be knowledgeable of the types of abuse and neglect, and familiar with the presenting signs and symptoms.
The orofacial complex is the most common site of physical injury resulting from child abuse.2 Oral manifestations of physical abuse include contusions (bruises), ecchymoses, abrasions, lacerations, fractures, burns, bites, hematoma, retinal hemorrhage, dental trauma, and fractures.1,2,5,12 Bruising is the most common manifestation in physical abuse. The following bruises are rarely accidental: bilateral bruising, which may indicate grabbing, shaking, or restraining; wraparound bruising (encircling the arms, legs, or torso), which may suggest restraint; and multicolored bruises, which may be a sign of varying degrees of healing and an indication of injuries occurring over time.10,14
When delivering dental care, clinicians should be alert to injuries to the lips, mouth, teeth, and maxilla and mandible. Injuries to the lips suggestive of abuse include abrasions; lacerations; chemical, thermal, or electrical burns (may be due to chemical substances, hot foods, or cigarettes); bruising; erosion; and scarring (from persistent trauma or the use of a gag when present in the labial commissure). Injuries to the upper lip and maxillary labial frenum may be a characteristic lesion in the severely abused young child.5,14 Tears of the labial or lingual frenum (due to a blow to the mouthor forced feeding), and burns or lacerations to the oral mucosa, hard palate, soft palate, tongue, or floor of the mouth are consistent with abuse.5,14 Teeth that are mobile or avulsed, displaced, fractured, darkened, or have multiple residual roots with no rational explanation of injury are indicative of maltreatment.
Finally, bone fractures (past and present) of the maxilla and mandible may involve the condyles, ramus, or symphysis. Malocclusion may result from these types of injuries.2,12
Bite marks are generally related to physical and sexual abuse.14 A forensic specialist should be consulted with this type of injury. Bite marks may manifest as elliptical- or ovoid-shaped contusions located between the teeth marks due to negative pressure (caused by suction or tongue thrusting) or positive pressure (caused by compression of teeth). A bite mark with an intercanine measurement of more than 3 cm is indicative of an adult human bite.14,15 The most common anatomical locations are the cheeks, back, sides, arms, buttocks, and genitalia.1 Notably, bites produced by dogs and other carnivorous animals tend to tear flesh, whereas human bites compress flesh and can cause abrasions, contusions, and lacerations—but rarely result in tissue tears.6
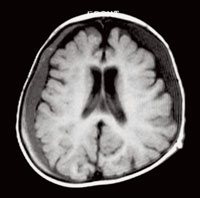
Trauma to the craniofacial complex is present in more than half of child abusecases.5,6 Physical injury may result in skull fractures and/or subdural hematomas (Figure 1). The latter physical injury causes more damage and is responsible for more deaths than any other form of abuse. Extraoral signs to watch for include trauma to the scalp, eyes, and ears. Oral health professionals should observe patients for the absence of hair and/or hemorrhaging beneath the scalp due to trauma from hair pulling; periorbital bruising or retinal hemorrhage of the eyes; and injury to the ears, including bruising, bite marks, or damage to the tympanic membrane.
SEXUAL ABUSE
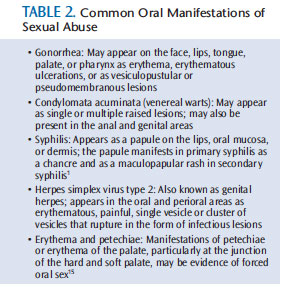
The diagnosis of sexual abuse may require referral to a forensic specialist or laboratory for culture of bodily specimens. Thus, proper diagnosis and treatment are best served through a multidisciplinary approach. Gonorrhea is the most common sexually transmitted disease in children (Table 2).1,7 The diagnosis of oral and perioral gonorrhea (supported with confirming laboratory tests) in prepubertal children is pathognomonic of sexual abuse. Pharyngeal gonorrhea is frequently asymptomatic.15
EMOTIONAL ABUSE
Unlike other types of abuse, the scars of emotional abuse are not physically visible. Watching for the following signs or behaviors may alert the dental professional to possible child neglect:
- Excessively withdrawn, fearful, or anxious about doing something wrong
- Extremes in behavior (extremely compliantor extremely demanding; extremelypassive or extremely aggressive)
- Appears emotionally detached from theparent/caregiver
- Acts either inappropriately mature (taking care of other children) or inappropriately infantile (rocking, thumb-sucking, throwing tantrums)
NEGLECT
Neglect is defined as “the failure of a parent or other person with responsibility for the child to provide needed food, clothing, shelter, medical care, or supervision to the degree that the child’s health, safety, and well-being are threatened with harm.”7 General neglect may present as hunger; poor personal hygiene; lack of adequate clothing; untreated medical conditions; or lack of supervision.
Dental neglect is defined as “willful failure of parent or guardian to seek and follow through with treatment necessary to ensure a level of oral heath essential for adequate function and freedom from pain and infection.”15 Dental neglect manifests as untreated rampant caries, easily detected by a layperson; or as untreated pain, infection, bleeding, or trauma affecting the orofacial region.16
When considering the possibility of neglect, ental professionals need to identify the reasons that the parent/caregiver has not taken care of the child’s oral health needs. Are there circumstances that prevent the parent/caregiver from pursuing care? Finances, lack of insurance, poor oral health literacy, transportation issues, and proximity to care are common barriers in accessing necessary dental care.6 Dental hygienists have the opportunity to listen and watch parents/caregivers and children interact, and further nurture the nonthreatening relationship important to any trusting professional visit.14 Customized patient education and resource information should be given to the parent/caregiver, along with encouragement to pursue care for the child.14
ASSESSING CHILD ABUSE AND NEGLECT
The primary goal in recognizing child abuse is to prevent further injury to the child.5 All patient care appointments should begin with a thorough health history assessment, followed by an intraoral and extraoral examination. Each clinician should employ observational steps during patient care that will decrease the likelihood of missing signs and symptoms of child abuse and maltreatment—which may include looking closely for unexplainable injuries to the head, neck, and oral tissues of each patient.14 Dental hygienists are trained to perform oral cancer exams on all patients, so keeping the signs of physical abuse in mind during a scan of the head, neck, and oral cavity is logical. Performing an intraoral and extraoral examination on each patient also reduces the likelihood that parents/caregivers will be suspicious about the need to conduct an oral cancer exam on young patients.
Oral health professionals should consider the following questions when assessing pediatric patients who present with an injury:5
- Is the clinical presentation of the injuryconsistent with the history as reported by theparent or caregiver? For example, 80% of children who fall out of bed do not sustain injuries.17
- Is there a history or signs of previousor repeated trauma?
- Are multiple bruises present at differentstages of healing, possibly in the pattern orshape of an object?
- Does the parent/caregiver or childexhibit unusual behavior?
- Is there any evidence of neglect or poor supervision of the child?
If an unusual injury or condition is suspected, it may be prudent to separate the child and parent and ask each how the injury occurred.1,2 Differing or inappropriate explanations of how the event occurred may help confirm or eliminate suspicions.9 Child maltreatment can come in many forms. As mentioned above, oral health professionals are not required to prove abuse or neglect; rather, they are expected to report suspected cases of abuse to the proper authorities.4 The dental hygienist’s role is to observe, educate, collect information, document, and refer if child abuse or neglect is suspected. For the sake of the child, the suspected abuse should be reported after a thorough assessment has been completed, treatment rendered, and the parent has been notified of the suspicions.1
DOCUMENTATION
The most important step after recognizing possible abuse is careful documentation. In the dental record, document the location, size, color, and any other factual information about the injury or injuries. Photographs and video can further enhance this process.9,14,18 Any lesions or marks should be photographed in relation to a millimeter measuring device for accurate reference.6,9,14 Document any explanations given by the child and parent about the injury. During any interview, be it with the child or parent/caregiver, ensure that a witness is present.
Any interpreter must be neutral, preferably a professional and not a family member. Documentation should include the names of the witnesses and interpreters. The information should be forwarded to the local child protection agency or law enforcement, depending on which authority was contacted regarding the suspected maltreatment.8
KEEP CURRENT
Continuing education in recognizing child abuse and neglect is important.1,18 Regularly scheduled staff meetings also provide anopportu nity to review the importance of recognizing abuse, developing strategies for communicating suspected abuse with the dentist, and reviewing the reporting resource options. Practice formulating open-ended, nonthreatening questions to ask children who present with injuries.18
Consider asking a local child health expert to assist with this process. Achieving confidence in identifying the signs and symptoms of child abuse and maintaining a list of local resources will reduce the anxiety that inevitably comes with witnessing a possible case of child abuse or neglect.18 This knowledge will also help clinicians identify instances of abuse among adults; individuals with disabilities and older adults are especially vulnerable.6
The role that oral professionals play in combating child abuse and neglect emphasizes the importance of securing a dental home for all children. The American Academy of Pediatric Dentistry recommends that all children establish a dental home by age 1.15
RESOURCES
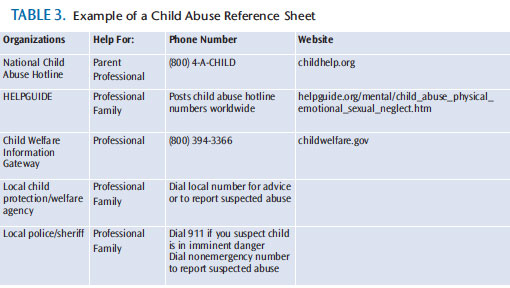
The entire dental team should be aware of the resources available to help vulnerable patient populations affected by suspected abuse, neglect, or maltreatment. A resource guide should be readily available for staff members to access quickly if child maltreatment is suspected (Table 3).19 A complete guide should include the nonemergency phone numbers for the local police department and child protection agency.14,19 These professionals can help answer questions and further assist in reporting. National Child Abuse Hotline counselors are available for advice and assistance for parents and practitioners.
In situations where a child may be in imminent danger if allowed to leave with the parent/caregiver, 911 should be called. A resource guide should also include phone numbers and Web-based resources for the parents to seek help and information.
The Child Welfare Information Gateway and helpguide.org contain links to help clinicians report abuse. As each state has different reporting criteria and restrictions, oral health professionals need to understand the reporting laws in their states. For instance, in most states, the provider-patient communication privilege does not supersede the mandate to report suspected abuse.8,20
Partnering with Delta Dental and state dental associations, Prevent Abuse and Neglect through Dental Awareness is an organization that educates oral health professionals on recognizing child maltreatment through seminars, and provides resources for professionals and families of victims.6 Clinicians can contact their state dental association or Delta Dental for more information on local continuing education programs.
CONCLUSION
Dental hygienists play an important role in the detection of child abuse, as most cases involve injury to the head, neck, and facial regions. Bringing the cycle of abuse and neglect to an end and preventing further injury requires that oral health professionals are knowledgeable about the types of abuse and neglect, can recognize the manifestations of abuse and neglect, and understand the mandatory reporting process in their state.
References
- Dentalcare.com. Child abuse and neglect: Implications for the dental professional. Available at: dentalcare.com/en-US/dental-education/continuing-education/ce49/ce49.aspx. Accessed January 19,2014.
- Ghosn J. The dentist’s role in detecting child abuse. Ontario Dentist. 2008;July/Aug:25–27.
- Children’s Bureau. Child Maltreatment. Available at: acf.hhs.gov/programs/cb/research-datatechnology/statistics-research/child-maltreatment. Accessed January 19, 2014.
- Oral Health America. April 2011 E-News. Available at: oralhealthamerica.org/presscenter/enewsletters/april-2011-e-news/. Accessed January 19, 2014.
- Needleman HL. Orofacial trauma in child abuse: types, prevalence, management, and the dental profession’s involvement. Pediatr Dent. 1986;8:71–80.
- American Dental Association. Report of the Council on Ethics, Bylaws and Judicial Affairs on Advisory Opinion 3.E.1. Reporting Abuse and Neglect. Available at: ada.org/sections/about/pdfs/final_report_on_3e1.pdf. Accessed January 19, 2014.
- Kellogg N, American Academy of Pediatrics Committee on Child Abuse and Neglect. Oral and dental aspects of child abuse and neglect. Pediatrics. 2005;116:1565–1568.
- Child Welfare Information Gateway, US Department of Health and Human Services. Mandatory Reporters of Child Abuse and Neglect. Available at: childwelfare.gov/systemwide/laws_policies/statutes/manda.cfm. Accessed January 19, 2014.
- Katner DR, Brown CE. Mandatory reporting of oral injuries indicating possible child abuse. J Am Dent Assoc. 2012;143:1087–1092.
- Sujatha G, Sivakumar G, Saraswathi TR. Role of a dentist in discrimination of abuse from accident. J Forensic Dent Sci. 2010;2:2?4.
- Childhelp. National Child Abuse Statistics. Available at: childhelp.org/pages/statistics. Accessed January 19, 2014.
- Jessee SA. Orofacial manifestations of child abuse and neglect. Am Fam Physician.1995;52: 1829?1834.
- Centers for Disease Control and Prevention. Child Maltreatment Prevention. Available at: cdc.gov/violenceprevention/childmaltreatment/index.html. Accessed January 19, 2014.
- Nuzzolese E, Lepore M, Montagna F, et al. Child abuse and dental neglect: the dental team’s role in identification and prevention. Int J Dent Hyg. 2009;7:96?101.
- American Academy of Pediatric Dentistry. Policy on the Dental Home. Available at: aapd.org/media/Policies_Guidelines/P_DentalHome.pdf. Accessed January 19, 2014.
- Delta Dental of Kansas. P.A.N.D.A.® Program. Available at: deltadentalks.com/Dentists/PANDAProgramDentists. Accessed January 19, 2014.
- Helfer RE, Slovis TL, Black M. Injuries resulting when small children fall out of bed. Pediatrics. 1977;60:533?535.
- Datta P, Datta S. Sensitization of dental team towards management of child abuse and dental neglect. Indian Journal of Forensic Odontology. 2012;5(3):97?104.
- Thomas JE, Straffon L, Inglehart MR. Knowledge and professional experiences concerning child abuse: an analysis of provider and student responses. Pediatr Dent. 2006;28:438?444.
- HELPGUIDE.org. Child abuse and neglect. Available at: helpguide.org/mental/child_abuse_physical_emotional_sexual_neglect.htm. Accessed January 19, 2014.
From Dimensions of Dental Hygiene. February 2014;12(2):48–52.
