 ELITSA DEYKOVA/E+/GETTY IMAGES PLUS
ELITSA DEYKOVA/E+/GETTY IMAGES PLUS
Preventing the Spread of Herpes Simplex Type 1
The dental team should be knowledgeable about the clinical presentations, distinguishing features, and treatment protocols of this virus to reduce the risk of transmission.
This course was published in the October 2020 issue and expires October 2023. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define herpes simplex virus type 1 and known risk factors for this infection.
- Discuss the clinical presentation, diagnosis, and treatment of this virus.
- Describe the role of oral health professionals in preventing the spread of herpetic infections among patients and dental team members.
There are more than 100 known herpes viruses, and herpes simplex virus type 1, or HSV-1, is one among the eight known to infect humans.1 The word “herpes” is a Greek word meaning “to creep or crawl” and its use is in reference to the spreading nature of the symptomatic lesions. HSV-1 causes infections in the mucocutaneous areas of the orofacial region, such as the lips, referred to as herpes labialis but commonly known as “cold sores” or “fever blisters.”2 Intraoral herpetic lesions may be confused with other ulcerative conditions. Further, uncertainty may exist concerning when to treat patients who present with viral infections such as HSV-1. Therefore, the focus of this paper is to describe the pathogenesis, diagnosis, clinical presentation, and treatment of HSV-1 as oral health professionals will most likely encounter patients seeking treatment while presenting with this condition.
Epidemiology and Risk Factors
HSV-1 infections are quite common and most often acquired during childhood.3–5 Among United States adults, almost 90% are exposed to HSV-1 by the time they are 50.6 Between 2005 and 2010, the percentage of HSV-1 seroprevalence in the US was 53.9, which is more than three times higher than the seroprevalence of HSV-2.7 HSV-1 prevalence among women (50.9%) is higher than for men (45.2%).8
An inverse relationship exists between seroprevalence of HSV-1 infections and an individual’s socioeconomic background.9 Lower socioeconomic populations have HSV-1 infections occurring early in life, before the age of 5. Also, HSV-1 infections are generally higher among immunocompromised individuals due to reduced systemic resistance.10
HSV-1 infections are often thought of as “above the belt;” however, genital herpes may also be caused by HSV-1.11,12 The known risk factor for initial infection of HSV-1 is generally contact with infected saliva and oral lesion secretions from another already infected individual. The primary transmission mode is asymptomatic shedding of the virus, compared to lesion shedding. Risk factors for recurrent HSV-1 include trauma such as diffuse axonal injury, stress (physical or emotional), reduced cellular immunity, fever, sunlight, and ultraviolet radiation exposure.4,5,11,13
Pathogenicity
HSV-1 belongs to the alpha (α) herpesvirus subfamily, which also includes other neurotropic viruses such as HSV -2 or genital herpes, and the varicella-zoster virus, which causes chickenpox and shingles (Figure 1).1,14
HSV-1 uses the human host for survival and replication. Its typical cellular level life cycle steps are adsorption, penetration, uncoating, replication, assembly, and release. HSV-1 stages can vary among the infected cells wherein the virus can be in latency in some cells and in the replication stage in other infected cells.15
HSV-1 is characterized by several unique properties including neurovirulence, latency, and reactivation.16,17 The virus has the capacity to invade and replicate in the nervous system (neurovirulence). In latency, the replicated virions travel in an anterograde fashion in nerve cell ganglion, and remain in a nonreplicative state until they are reactivated. The trigeminal ganglia are most commonly involved for HSV-1. Reactivation and replication of latent HSV result in overt or covert recurrent infection and shedding of the virus.15 In approximately one-third of infected individuals, once infected, the virus remains lifelong.18
Clinical Presentation
HSV-1 can cause either primary or reactivation infections. The clinical course of this oral infection depends on age, immune status of the host, and anatomic site of involvement.11,16 Primary HSV-1 is manifested in children usually between the ages of 6 months and 5 years as acute (or primary) herpetic gingivostomatitis. Adolescents and adults may also develop acute gingivostomatitis, but it can be less severe, and is more often associated with posterior pharyngitis. HSV infections (primary and recurrent) occurring in immunocompromised individuals tend to be more severe, prolonged, widespread, and more likely to recur.11,16,19
Clinical features of primary herpetic gingivostomatitis include, but are not limited to, fever; anorexia; malaise; lymphadenopathy; headache; nausea; vomiting; gingivitis (markedly swollen, erythematous, friable tissue); and vesicular lesions. Vesicles can occur on the oral mucosa, palate, tongue, and lips, which rupture and coalesce into painful ulcers.10,11,16,20,21 Oral lesions tend to occur within 1 day to 2 days of systemic symptoms. Acute herpetic gingivostomatitis lasts approximately 5 days to 7 days; symptoms resolve within 2 weeks. However, viral shedding from the saliva may continue for 3 weeks or longer.11,16
In adults, primary HSV-1 causes pharyngitis and tonsillitis more often than herpetic gingivostomatitis, and is referred to as acute herpetic pharyngotonsillitis. This condition is accompanied by fever, headache, malaise, and sore throat with pharyngeal erythema or exudate. Herpetic oral and labial lesions occur in less than 10% of patients who experience acute herpetic pharyngotonsillitis.16,22
Reactivation of HSV-1 is usually manifested as recurrent herpes labialis.23 Prodromal symptoms of tingling, pain, itching, and burning are common at the affected site followed by the development of vesicles that become pustular, ulcerate, and form a crust. Reactivated herpes infection can also occur intraorally on the hard palate and gingiva, beginning as a cluster of vesicles that then coalesce into ulcerations.21,24,25 HSV-1 recurrence is estimated to occur in one-third to 40% of individuals.19,27 The number of recurrences can range from once per year to once per month.25 The duration of recurrent symptoms tends to be shorter and the symptoms are often less severe. Further, recurrences can be subclinical or clinically unrecognizable, therefore, transmission to susceptible individuals can occur in the absence of overt lesions.16,21,27
![human herpes virus family tree]() Differential Diagnosis
Differential Diagnosis

The diagnosis of oral HSV-1 is typically made by the appearance and location of lesions and patient history.21,25,28 However, not all lesions are readily apparent. The differential diagnosis for primary symptoms includes impetigo, streptococcal pharyngitis, erythema multiforme, acute necrotizing ulcerative gingivitis, Behcet syndrome, herpangina, pemphigus vulgaris, candidiasis, hand-foot-and-mouth disease, herpes zoster, and syphilis.10,11,16,19,21,24,25 The differential diagnosis for intraoral recurrent herpes is aphthous ulcers. Herpetic lesions tend to have prodromal symptoms, multiple lesions, vesicles precede ulcers, and the location of the lesions are the palate and gingiva. Aphthous stomatitis, in contrast, tends to be single vs coalescing, larger, and almost exclusively on nonkeratinized mucosa such as the buccal mucosa, alveolar mucosa, or floor of the mouth.24,25
Adjunctive diagnostic testing is available to confirm HSV infection and is required to diagnose atypical presentations. Examples of laboratory studies include tissue culture, Tzank smear, polymerase chain reaction, direct fluorescent antigen, and antibody testing.16,20,25 Detection of HSV DNA through polymerase chain reaction techniques is the preferred testing modality and can be used to detect asymptomatic viral shedding.16
![]() Treatment and Prognosis
Treatment and Prognosis
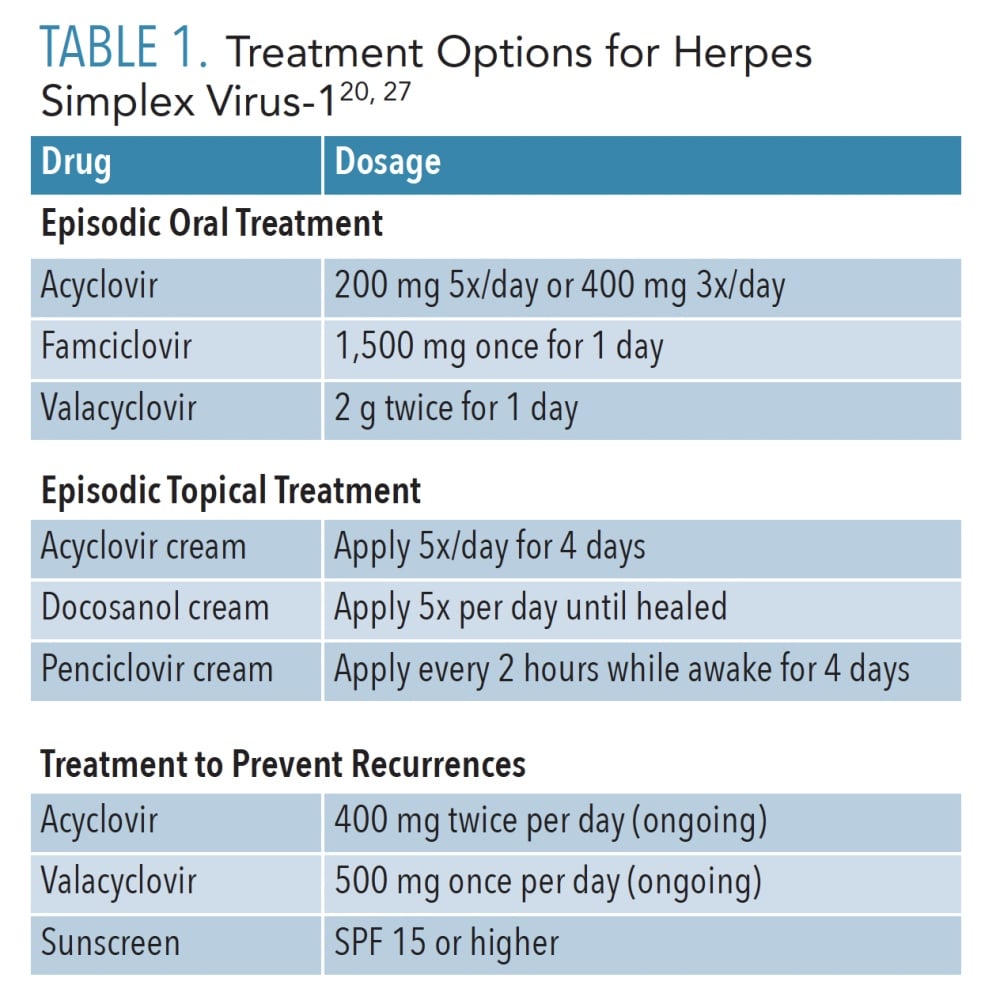
Most HSV-1 infections are self-limiting and resolve within 7 days to 14 days.24 Treatment consists of over-the-counter products and prescription antiviral medications (Table 1). These therapies are most beneficial if provided during the prodromal stage within 24 hours to 48 hours of lesion onset.20 These medications shorten the duration and severity of the infection, but do not eliminate the virus from the body. Supportive therapy, including fluids, rest, and analgesics, are important adjuncts for individuals experiencing primary HSV-1.
In addition, patients should be counseled to use a lip balm with sunscreen of at least SPF15 and to avoid know triggers for outbreaks. When lesions are present and patients are applying creams or ointments, instruct them to use a cotton applicator or rubber glove to prevent autoinoculation or transmission of the virus to other parts of the body or to other people.24, 25
Oral Health Considerations
Most dental histories include a section that asks about a history of sores or ulcers in the mouth. If a patient answers positively to this question or presents with lesions that appear to be herpetic in nature, oral health professionals should document the location, frequency, and duration of lesions; symptoms associated with those lesions; known triggers; disease course; treatment rendered; complications associated with the lesions and/or treatment; and overall medical history that might correlate with the oral condition. If atypical lesions are found or recurrent intraoral herpes is present in an immunocompromised patient, further diagnostic investigation is warranted using laboratory analysis, and the patient should be referred to an appropriate dental or medical specialist with expertise in this area.28
In some cases, individuals who are unfamiliar with the contagious nature of HSV-1 present with a primary or recurrent lesion, and expect oral healthcare to be performed. This unique situation is the perfect opportunity to provide education regarding the nature of this viral condition. Patients need to understand they are contagious and pose a risk to themselves and the dental team. Advise patients their appointment can be rescheduled once the lesion is completely healed.26,28 During the time of an active lesion, individuals should limit personal contact, especially as there is shedding of the virus in their saliva.28 Meticulous hygiene is important, and individuals must use caution as they can spread the virus through autoinoculation. Oral health professionals should educate patients to avoid sharing utensils and food, limit touching the lesions, and wash hands frequently with soap and water to prevent the risk of cross-infection.
Elective dental and dental hygiene treatment should be deferred for patients who present with active herpetic lesions.16,24,26,28 Treatment may be uncomfortable and the patient is at risk for the spread of infection or re-infection. Treatment should be postponed until the lesions are completely healed. Oral health professionals are at risk of infection through aerosolization of the virus during dental procedures.24,28 Examples of occupational herpetic infections among oral health professionals include herpetic whitlow and herpes keratitis.26
For patients who present with an active HSV-1 infection with need for urgent or emergency dental care, Browning and McCarthy26 recommend the following:
- Use extreme caution and extra personal protective equipment that fully covers the body, eyes, and face
- Wear a National Institute for Occupational Safety and Health N95 rated or higher mask to protect against aerosol
- Avoid instruments and hands touching the lesion as much as possible
- Change gloves frequently if the procedure is lengthy
- Wash hands with soap and water between glove changes
- Provide eye protection for the patient
- Recommend the patient wash hands and face after treatment
- Educate the patient about the nature of the herpes virus
If a member of the dental team has an orofacial herpes infection, limit treatment to those patients who are immunocompetent; cover the lesion area with a suitable mask and use a facial shield; change gloves frequently if the hand is brought anywhere near the team member’s mouth; and inform the patient of the team member’s condition and get his or her consent to treat.26
Herpetic whitlow is highly infectious; therefore, dental team members with this condition should not work until the lesions are healed. In the case of herpes keratitis, viral shedding is high. Protect patients by washing hands with soap and water in between glove changes and following the protocol described above.
Some oral health professionals and patients may consider the above recommendations disruptive to the office schedule, all for a simple “cold sore;” however, negative effects in proceeding with elective treatment must be considered. Browning and McCarthy26 note that the patient-provider relationship could be compromised if the patient later develops active herpetic lesions or worsening of symptoms all of which could have been avoided by postponing treatment during active infection periods. Further, employers have an obligation to follow guidelines and take precautions to protect employees.29 The risk of infection of a dental team member is likely greater than the temporary inconvenience of delaying elective treatment for a patient with an active infection from a herpetic lesion.
Lastly, laser treatment has been used to manage recurrent herpes labialis. A review of the literature examining the efficacy of lasers revealed that laser phototherapy appears to decrease pain and the interval of recurrences. High power lasers may also be beneficial in draining vesicles. Other advantages include the absence of drug interactions and side effects. However, none of the laser therapies completely eliminate the virus or recurrence. Most literature represented are case reports. Additional studies are needed that address efficacy of laser therapy in terms of duration of viral shedding, viral inactivation, and interval of recurrence.30 Oral health professionals must recognize that while the lip lesion may have been lased, the nature of the virus is such that active virus may be present in the saliva, leaving the patient vulnerable to intraoral infection if elective treatment is rendered.
Conclusion
HSV-1 is a ubiquitous viral infection with oral implications. Primary and secondary infections may occur, although, most lesions are self-limiting and will resolve within 1 week to 2 weeks. Oral health professionals should be cognizant of the clinical presentations, distinguishing features, and treatment protocols to prevent the spread of infection among patients and the dental team.
References
- Whitley RJ. Herpesviruses. In: Baron S, ed. Medical Microbiology. Galveston, Texas: University of Texas Medical Branch at Galveston; 1996.
- Baltimore D, Lodish H. Molecular Cell Biology. 7th ed. New York: WH Freeman and Co; 2012:248.
- United States Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2017. Available at: cdc.gov/std/stats17/other.htm. Accessed September 11, 2020.
- Carroll KC, Butel JS, Morse SA. Jawetz Melnick & Adelbergs Medical Microbiology. 27th ed. New York: McGraw-Hill Education; 2015:864.
- Mertz GJ. Asymptomatic shedding of herpes simplex virus 1 and 2: implications for prevention of transmission. J Infect Dis. 2008.;198:1098–1100.
- Johns Hopkins Medicine. Oral Herpes. Available at: hopkinsmedicine.org/health/conditions-and-diseases/herpes-hsv1-and-hsv2/oral-herpes. Accessed September 11, 2020.
- Bradley H, Markowitz LE, Gibson T, McQuillan GM. Seroprevalence of herpes simplex virus types 1 and 2—United States, 1999-2010. J Infect Dis. 2014;209:325–333.
- US Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. Available at: cdc.gov/nchs/nhanes/index.htm. Accessed September 11, 2020.
- Arduino PG, Porter SR. Herpes simplex virus type 1 infection: overview on relevant clinico-pathological features. J Oral Pathol Med. 2008;37:107–121.
- Roizman B, Knipe DM, Whitley RJ. Herpes simplex viruses. In: Knipe DM, Howley P, eds. Fields Virology. Philadelphia: Lippincott Williams & Wilkins; 2013:1823–1897.
- Brown DN, Kollipara R, Tyring S. Oral signs of viral disease. In: Fazel N, ed. Oral Signs of Systemic Disease. Cham, Switzerland: Springer Nature; 2019:145–167.
- Cunningham A, Griffiths P, Leone P, et al. Current management and recommendations for access to antiviral therapy of herpes labialis. J Clin Virol. 2012;53:6–11.
- Kolokotronis A, Doumas S. Herpes simplex virus infection, with particular reference to the progression and complications of primary herpetic gingivostomatitis. Clin Microbiol Infect. 2006; 12:202–211.
- Ananthanarayan R, Paniker CKJ. Ananthanarayan and Paniker’s Textbook of Microbiology. 7th ed. Hyderabad, India: Orient Longman; 2006.
- Pellett PE, Roizman B. Herpesviridae. In: Knipe DM, Howley P, eds. Fields Virology. Philadelphia: Lippincott Williams & Wilkins; 2013:802–1822.
- Medscape. Herpes Simplex. Available at: emedicine.medscape.com/article/218580-overview. Accessed September 11, 2020.
- Schiffer JT, Corey L. Herpes simplex virus. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Philadelphia: Elsevier/Saunders; 2015:1713–1730.
- Li Z, Fang C, Su Y, et al. Visualizing the replicating HSV-1 virus using STED super-resolution microscopy. Virol J. 2016;13:1–13.
- Amir J. Primary herpes simplex gingivostomatitis and recurrent orolabial Infection. In: Studahl M, Cinque C, Bergström T, eds. Herpes Simplex Viruses. Boca Raton, Florida: CRC Press; 2006.
- Stoopler ET, Sollecito TP. Oral mucosal diseases: evaluation and management. Med Clin North Am. 2014l98:1323–1352.
- Usatine RP, Tinitigan R. Nongenital herpes simplex virus. Am Fam Physician. 2010;82:1075–1082.
- McMillan JA, Weiner LB, Higgins AM, Lamparella VJ. Pharyngitis associated with herpes simplex virus in college students. Pediatr Infect Dis J. 1993;12:280–284.
- Ramchandani M, Kong M, Tronstein E, et al. Herpes simplex virus type 1 shedding in tears and nasal and oral mucosa of healthy adults. Sex Transm Dis. 2016;43:756–760.
- DeLong L, Burkhart NW. General and Oral Pathology for the Dental Hygienist. 3rd ed. Philadelphia: Wolters Kluwer; 2019.
- Regezi JA, Sciubba J, Jordan RCK. Oral Pathology: Clinical Pathologic Correlations. 7th ed. St. Louis: Elsevier; 2017.
- Browning WD, McCarthy JP. A case series: herpes simplex virus as an occupational hazard. J Esthet Restor Dent. 2012;24:61–66.
- Opstelten W, Neven AK, Eekhof J. Treatment and prevention of herpes labialis. Can Fam Physician. 2008;54:1683–1687.
- Stoopler ET, Kuperstein AS, Sollecito TP. How do I manage a patient with recurrent herpes simplex? J Can Dent Assoc. 2012;78:154.
- United States Department of Labor. Occupational Safety and Health Standards. United States Code of Federal Regulations; CFR 1910.1030 Bloodborne Pathogens. Available at: osha.gov/pls/oshaweb/owadisp.show_document?p_id=10051&p_table=STANDARDS. Accessed September 11, 2020.
- de Paula Eduardo C, Aranha AC, Simões A, et al. Laser treatment of recurrent herpes labialis: a literature review. Lasers Med Sci. 2014;29:1517–1529.
From Dimensions of Dental Hygiene. October 2020;18(9):36-39.
