
Making the Principles of Ergonomics Work for you
Preventive strategies can keep practice pain-free and ensure a long career in clinical dental hygiene.
Upon graduation, most dental hygienists anticipate a long career in clinical dental hygiene practice. This goal is unachievable without ergonomics. Defined as “the study of the problems of people in adjusting to their work environment, especially the science that seeks to adapt work to suit the worker,”1 the principles of ergonomics are key to avoiding the physical and financial challenges common in dental hygiene.
Dental hygiene practice has a myriad of ergonomic risk factors, including repetition of wrist and arm movements, restricted hand movements, forceful exertions, uncomfortable body posture held for extended periods of time, and vibrations transmitted by dental handpieces or mechanical scalers.2-5 In short, dental hygienists experience daily activities that involve frequency, duration, and force.6 Other work-related factors that predispose hygienists to cumulative traumatic disorders (CTDs) involve the number of hours worked per related factors that predispose hygienists to cumulative traumatic disorders (CTDs) involve the number of hours worked per week, the number of difficult patients treated per day and per hour, and the number of years employed as a dental hygienist. In addition, mechanical stress due to instrument design and the type of treatment gloves, ie, ambidextrous, worn by the clinician may affect the physical well-being of the hygienist.8,9
![]() Cumulative Traumatic Disorders
Cumulative Traumatic Disorders
 Cumulative Traumatic Disorders
Cumulative Traumatic DisordersThe most common of type of CTD is carpal tunnel syndrome. The occurrence of carpal tunnel syndrome in the general public is substantially lower than that reported by dental hygienists.10,11 CTDs include all disorders affecting the musculoskeletal, autonomic, and peripheral nervous system caused by repetition, force, and unusual body movements.12,13 Some musculoskeletal and nerve disorders that affect dental hygienists include:
- Ulnar and radial nerve entrapment
- Pronator syndrome
- Tendinitis of the shoulder, elbow, wrist, or hand
- Tenosynovitis
- Extensor wad strain
- Thoracic outlet syndrome, and muscle pain and cramping.7,10
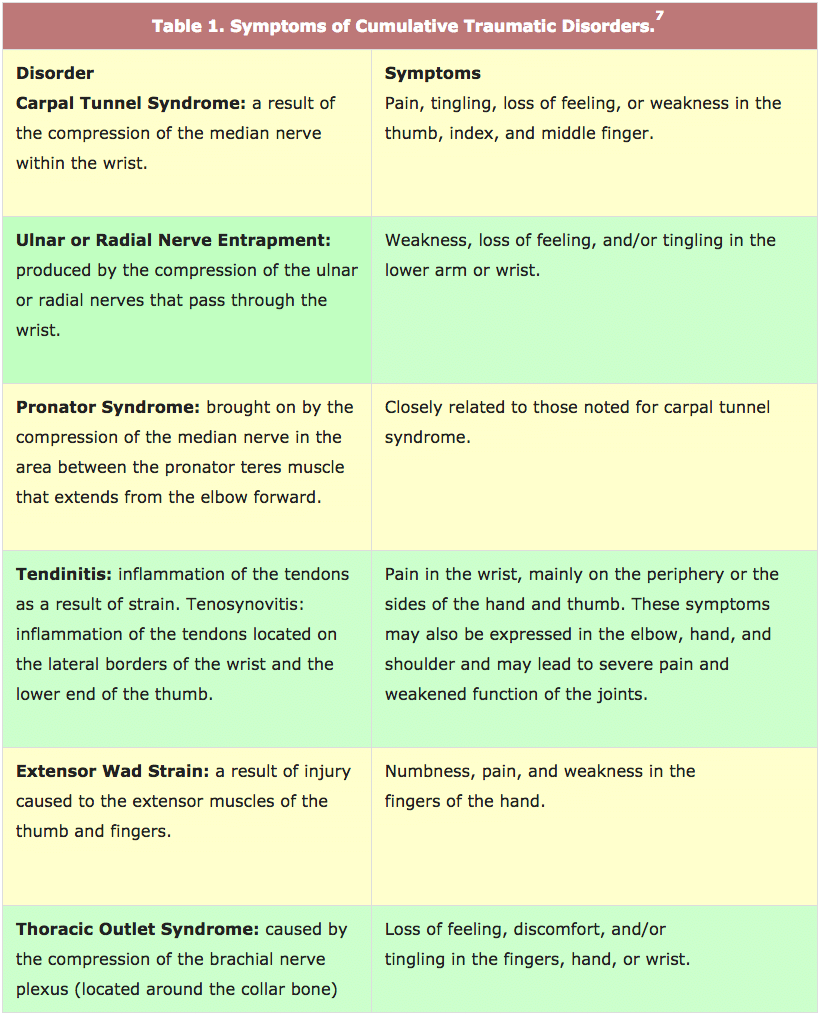
These disorders are often precipitated by various postural-related problems such as repetitive hand movements, hand twisting and bending, intense gripping of instruments, separation of the fingers during instrumentation, raised shoulders, continuous reaching, prolonged forward tilting of the head, and raised elbows and arms.7 In general, symptoms of CTDs have been reported as pain, numbness, or tingling in either the neck, back, arm, hand, wrist, or fingers.14 Specific manifestations of each disorder are shown in Table 1.

Economic Impact
CTDs not only cause pain but also result in lost wages, medical costs, and loss of productivity for the dental office. Each year, carpal tunnel sufferers make over 2 million visits to the physician’s office.15 According to the Bureau of Labor statistics, carpal tunnel syndrome resulted in 22,651 days away from work in 1 year.16
Preventive Strategies
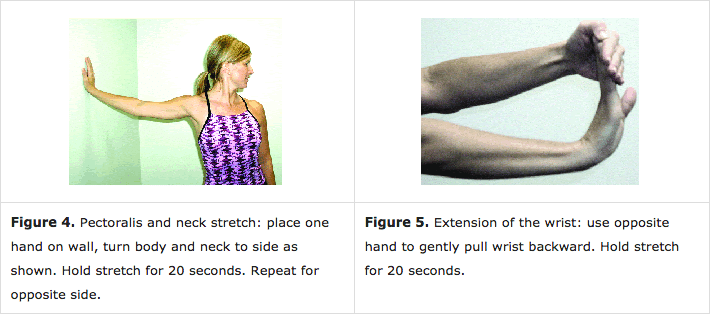
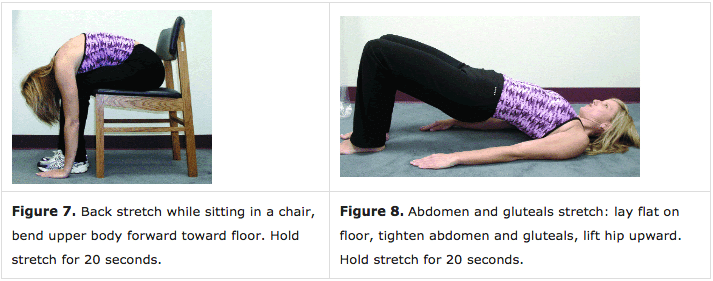
In order to prevent unnecessary pain and to ensure career longevity, dental hygienists must be aware of the signs and symptoms of and the strategies for preventing CTDs. Ongoing research in ergonomics provides practical recommendations in order to enhance the long-term practice of dental hygiene. Table 2 lists several preventive strategies for practicing dental hygienists. The suggestions focus on equipment used, instrumentation techniques, positioning, work schedules, and personal care. Figures 1 through 8 demonstrate recommended stretching exercises to be performed before, during, and after working hours.

Registered dental hygienists may also benefit from seeking medical specialists and other health care providers. This may include chiropractors, physicians, orthopedic surgeons, physical therapists, and occupational therapists. Lastly, registered dental hygienists should consider purchasing quality disability insurance. Many companies and organizations, including the American Dental Hygienists’ Association offer this type of insurance.
Conclusion
Practicing pain-free dental hygiene should be a reality for all oral health care providers. Using ergonomic developments within the dental industry and applying research findings from ergonomic studies should allow dental hygienists to enjoy a satisfying and long-term career. Ignoring ergonomic issues may contribute to the development of CTDs that cost money, result in pain, and increase the possibility of a shortened career. Dental hygienists should stay abreast of the most current findings, share the information with their employers, and incorporate the newest ergonomic research findings into practice.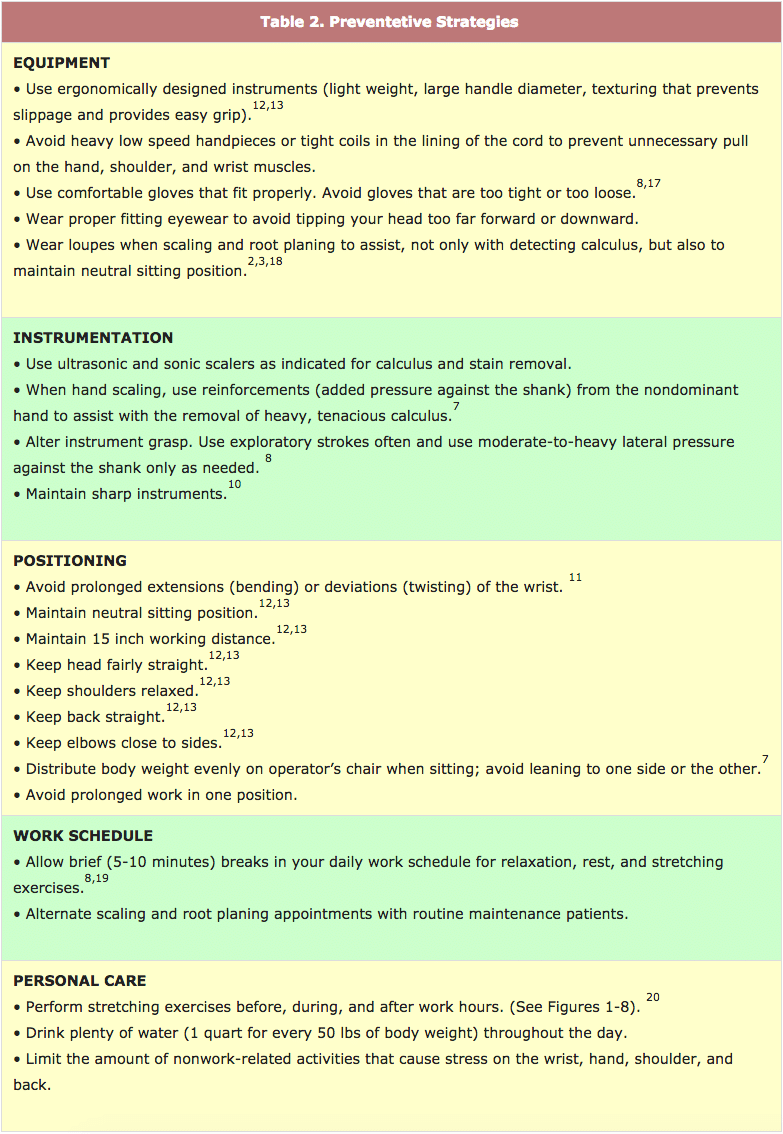
References
- Agnes M, Guralnik DB, eds. Webster’s New World College Dictionary . 4th ed. Foster City, Calif: IDG Books Worldwide Inc; 2001: 482.
- Smith CA, Sommerich CM, Mirka GA, George MC. An investigation of ergonomic interventions in dental hygiene work. Appl Ergon . 2002;33(2):175-184.
- Sunnell S, Maschak L. Positioning for clinical dental hygiene care. Preventing back, neck and shoulder pain. Probe . 1996;30(6):216-219.
- Werner RA, Armstrong TJ. Carpal tunnel syndrome: ergonomic risk factors and intra carpal canal pressure. Phys Med Rehabil Clin N Am . 1997;8(3):555-569.
- Rempel DM, Harrison RJ, Barnhart S. Work-related cumulative trauma disorders of the upper extremity. JAMA . 1992;267:838-842.
- Bramson JB, Smith S, Romagnoli G. Evaluating dental office ergonomic. Risk factors and hazards. J Am Dent Assoc . 1998;129:174-183.
- Nield-Gehrig JS. Fundamentals of Periodontal Instrumentation . 5th ed. Baltimore, Md: Lippiconcott Williams and Wilkins; 2004:12-16, 517-518.
- Gerwatowski LJ, McFall DB, Stach DJ. Carpal tunnel syndrome. Risk factors and preventive strategies for the dental hygienist. J Dent Hyg. 1992;66:89-94.
- Powell BJ, Winkley GP, Brown JO, Etersque S. Evaluating the fit of ambidextrous and fitted gloves: Implications for hand discomfort. J Am Dent Assoc. 1994;125:1232-1242.
- Werner RA, Hamann C, Franzblau A, Rodgers PA. Prevalence of carpal tunnel syndrome and upper extremity tendinitis among dental hygienists. J Dent Hyg . 2002; 76:126-132.
- Lalumandier JA, McPhee SD. Prevalence and risk factors of hand problems and carpal tunnel syndrome among dental hygienists. J Dent Hyg . 2001;75:130-134.
- Wilkins EM. Patient reception and positioning. In: Clinical Practice of the Dental Hygienist . 9th ed. Baltimore, Md: Lippincott Williams and Wilkins; 2005:84-86.
- Matsuda SA. Instruments and principles for instrumentation. In: Clinical Practice of the Dental Hygienist . 9th ed. Baltimore, Md: Lippincott Williams and Wilkins; 2005:,612-613.
- Michalak-Turcotte C. Controlling dental hygiene work-related musculoskeletal disorders: the ergonomic process. J Dent Hyg . 2000;74:41-48.
- What is carpal tunnel syndrome (CTS)? Available at: http://yourmedicalsource.com /library/carpaltunnel/CT_whatis.html. Accessed December 13, 2004.
- US Department of Labor. Bureau of Labor Statistics. Available at: www.bls.gov/iif/oshwc/osh/case/ostb1265.pdf. Accessed December 13, 2004.
- Liskiewicz ST, Kerschbaum WE. Cumulative trauma disorders: an ergonomic approach for prevention. J Dent Hyg . 1997;71:162-167.
- Syme SE, Fried JL, Strassler HE. Enhanced visualization using magnification systems. J Dent Hyg . 1997;71:202-206.
- Oberg T, Karsznia A, Sandsjo L, Kadefors R. Work load, fatigue, and pause patterns in clinical dental hygiene. J Dent Hyg . 1995;69:223-229.
- Daniel SJ, Harfst SA. Mosby’s Dental Hygiene Concepts, Cases and Competencies . St Louis: Mosby Elsevier Science; 2002:132.
From Dimensions of Dental Hygiene. January 2005;3(1):16-18, 20-21.

{kind=link}