
Instrument Selection for Premolar Teeth
This is key to effective nonsurgical periodontal therapy and periodontal maintenance.
The mechanical removal of deposits—from plaque biofilm to calculus —is key to effectively caring for patients with different oral health statuses, including those with a healthy periodontium, gingival inflammation, or impaired junctional epithelium and alveolar bone. However, the complex root anatomy of premolar teeth makes instrumentation challenging. The use of both ultrasonic and hand instrumentation is the typical course of action, as both are effective and complement each other.1,2 In the final installment of this series, the focus will be on instrument selection for nonsurgical periodontal therapy and periodontal maintenance with an emphasis on premolar teeth.
NONSURGICAL PERIODONTAL THERAPY
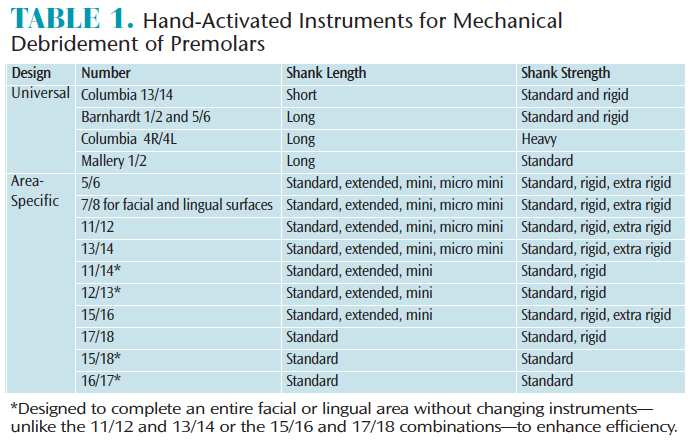
The instrumentation used in nonsurgical periodontal therapy (NSPT) is an extension of that used for prophylaxis and scaling, and a wide variety of instruments can be used for premolars (Table 1). During initial NSPT, large deposits will likely be present, accompanied by significant subgingival oral biofilm. Consequently, ultrasonic instrumentation with large edged tips/inserts and hand-activated working files are indicated.3–7
Traditional universal and area-specific hand instruments are used in scaling and root planing to reach difficult areas and remove calculus deposits (Figure 1). For heavier calculus removal, clinicians might consider shanks that are more rigid, such as the Columbia 4R/4L and the Gracey area-specific 7/8, 11/12, or 13/14 with rigid or extra-rigid shanks.
Other choices for NSPT include the area-specific double Gracey design where the operator can move from mesial to distal without “flipping” the instrument for different ends. They are manufactured in anterior and posterior options with standard or mini designs. Also, the Langer series is made in extended shank and mini versions.
Diamond file hand instruments are indicated for finishing root surfaces, particularly in depressions and furcations. They are double ended and used with multidirectional strokes. Some designs have a 360° diamond coating while others have a 180° coating, so the noncoated, smooth surface is placed against the gingiva.
PERIODONTAL MAINTENANCE

Hand instruments used in periodontal maintenance are selected based on the data collected at the recare visit and root surface characteristics. For patients with good self-care and who adhere to 2-month to 4-month periodontal maintenance schedules, the root structure should be relatively smooth. As such, flexible shanks are an option. If deep periodontal pockets exist, extended shank instruments are excellent choices. Specifically, new periodontal maintenance curets designed for tight tissue are available. They have small blades and are honed at a 60° angle with a modified rigid shank to facilitate access.
During periodontal maintenance, a smooth premolar root in a deep pocket surrounded by healthy gingiva might warrant biofilm disruption with debridement curets, a mini- or micro-mini area-specific instrument with a flexible shank, or periodontal maintenance curets. However, a seemingly smooth root in a deep pocket with adjacent gingival inflammation clearly calls for different instrumentation in regard to extent and thoroughness to aid in reversing the inflammation. The micro designs and periodontal maintenance curets will be particularly useful in narrow deep pockets. As periodontal maintenance visits continue over time, the need for root surface instrumentation should remain static or decrease.
CONCLUSION
A combination of ultrasonic and hand instrumentation is the typical approach in root debridement, followed by root planing with hand instruments.2 Premolar teeth are challenging to instrument due to their complex root anatomy. The use of extended shank, area-specific curets and mini- and micro-bladed instruments should be considered for concavities, grooves, and exposed furcations on premolars. The addition of diamond-coated files may also help clinicians achieve adequate root debridement.
REFERENCES
- Mann N. The blended approach to instrumentation. Dimensions of Dental Hygiene. 2016;14(11):45–50.
- Krishna R, de Stefano JA. Ultrasonic vs. hand instrumentation in periodontal therapy: clinical outcomes. Periodontol 2000. 2016;71:113–127.
- Hodges KO. The use of files. Dimensions of Dental Hygiene. 2004;2(11):16–20.
- Pattison AM. Keys to effective calculus removal. Dimensions of Dental Hygiene. 2011;9(10):50–53.
- Hodges KO. Strategies for selecting ultrasonic inserts/tips. Dimensions of Dental Hygiene. 2014.12(10):26–31.
- Matsuda S. Strategies for success. Dimensions of Dental Hygiene. 2016;14(10):24–26.
- Matsuda S. Decision making in ultrasonic instrumentation. Dimensions of Dental Hygiene. 2017;15(1):2426.
Featured photo by LEEZSNOW/ISTOCK/GETTY IMAGES PLUS
From Dimensions of Dental Hygiene. November 2017;15(11):30,32.

{kind=link}