
Help Older Adults Maintain Their Oral Health
By promoting healthy behaviors and encouraging prevention, dental hygienists can make a difference in both the oral and systemic health of this patient population.
This course was published in the March 2013 issue and expires March 2016. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the effects of aging on the appearance and structure of the teeth.
- Identify the most common oral problems seen in older adults.
- List relevant treatment strategies for addressing these issues in older patients.
The fact that the fastest growing segment of the United States population is adults age 65 and older is changing dental patient demographics.1,2 As such, oral health professionals must remain up to date on the specifics of providing care to older adults in order to help them maintain their oral health. Age alone is not a major factor in impaired dental health, although systemic diseases commonly experienced by older adults, as well as their treatments, can affect oral health and function. Another important determinant of oral health is a patient’s level of independence, which greatly affects his or her ability to maintain oral hygiene. Institutionalized older adults, as well as those of lower socioeconomic status, are at greater risk of oral disease than the general population.3
More of today’s older adults retain their original dentition compared to generations past. The rate of edentulism in the US has declined from 20.3% in 1972 to 13.9% in 2001.4 As a result, oral care for older adults now includes periodontal and restorative procedures, as well as esthetic treatment and implant therapy.5 Aging populations are at increased risk of oral diseases, including caries, periodontitis, tooth loss, xerostomia, fungal infections, benign soft tissue lesions, and malignant oral lesions, and dental professionals must be prepared to provide both effective treatment and prevention education.6
APPEARANCE AND STRUCTURE
The most common dental issues among older adults are those affecting the appearance and structure of teeth. The teeth become darker with age because of changes in the thickness of the underlying dentin. Enamel undergoes staining, chipping, and cracking, making it more susceptible to fractures. Abnormal wear in the form of attrition and abrasion also contributes to altered appearance of teeth.1,6 Older people are also at risk of developing new and recurrent coronal caries, as well as root caries (Figure 1). The incidence of root caries in patients older than 60 is twice that of 30-year-olds, and more than 64% of people older than 80 have root caries.6 This is due to factors such as increased gingival recession, inadequate saliva, less effective oral hygiene, and diminished motor skills, which are common among older adults. Improperly maintained prosthetic appliances are also detrimental to oral health. Many older adults have difficulty chewing and thus shift their diet from complex to simple sugars, which profoundly affects caries risk.
Treatment of caries among older adults is similar to other patient populations. Regular oral hygiene; professional dental care; consistent fluoride exposure, both in-office and at home applications; use of calcium phosphate technologies; and application of fluoride releasing restorative materials, such as glass ionomer, are all helpful.7 Patients with limited dexterity may benefit from oral health aids such as an power toothbrushes and floss holding devices.6
PERIODONTAL HEALTH
Periodontal health is affected by multiple factors such as systemic health, medication use, and poor oral hygiene.1 Since these are more common in the aging population, older adults typically present with gingival recession and loss of periodontal attachment and bony support (Figure 2). Medications, such as antihypertensive calcium channel blockers, phenytoin (antiseizure medicine), and cyclosporine (immunosuppressant), are frequently associated with gingival enlargement.
Besides its association with systemic health conditions, periodontitis can also cause localized problems like breath malodor and tooth loss, which can lead to difficulty eating and swallowing. Most older adults have mild to moderate periodontitis, and only a fraction experience attachment loss greater than 8 mm, making periodontal treatment possible for most.3

Periodontal treatment includes consistent and effective oral hygiene and regular, professional dental care. Since periodontal infection and inflammation interact with other systemic ailments, maintaining oral hygiene is imperative. Medical conditions, such as arthritis, can inhibit plaque control efforts, therefore, dental professionals should provide patients with individualized oral hygiene instructions on a regular basis, including demonstrating the use of appropriate aids and involving patients’ caregivers.3
XEROSTOMIA
Reduced levels or absence of saliva can significantly affect patients’ quality of life.8 Xerostomia is estimated to affect millions of people in the US and is most common in women. Ship et al estimated that approximately 30% of Americans age 65 and older experience dry mouth,9 although aging in itself is not the cause.10 Complaints of dry mouth are most often the result of systemic diseases, such as Sjögren’s syndrome, and medication use.
Xerostomia is a common side effect of as many as 80% of frequently-prescribed medications. Many anticholinergics, antidepressants, antipsychotic agents, diuretics, antihypertensives, sedatives, anxiolytics, muscle relaxants, certain analgesics, antihistamines, cytotoxic drugs, as well as drugs prescribed for smoking cessation, Parkinson’s disease, and incontinence, can cause xerostomia.8,10 Radiation therapy for the treatment of head and neck cancer can injure the salivary glands and result in transient or permanent xerostomia. In addition, patients with poorly managed diabetes are more likely to experience xerostomia.

The most common symptoms associated with a reduction in saliva are dry mouth, sore or burning sensation in the oral cavity, altered taste, and the need to take sips of water when swallowing foods. Reduced saliva increases the risk of cervical and root caries and opportunistic infections like candida. Xerostomia can also impact the stability of dental prosthetics. Affected patients often complain of dry lips, breath malodor, masticatory problems, and difficulty sleeping and speaking.10,11 The impact of low salivary flow on gingival bleeding, calculus, and attachment loss, however, is minimal.11,12
The general approach to treating patients with xerostomia is to offer symptomatic relief and prevent oral complications. If the symptoms are caused by medication use, the patient’s primary physician may be consulted to see if the drug or dosage can be modified.
Maintaining hydration by drinking frequent sips of water or holding ice chips in the mouth benefits some patients. Food and beverages that dehydrate the oral mucosa, such as alcohol, should be avoided. A variety of over-the-counter saliva substitute products, such as sugarless chewing gum, mouthrinses, and sprays, can help alleviate symptoms. Cholinergic agents may also benefit patients.

Maintaining exceptional oral hygiene and avoiding cariogenic foods can help prevent dental complications. The topical application of fluoride and calcium phosphate technologies can help prevent dental decay.7,8,10 Alternative treatments, such as acupuncture, also have shown some success in the treatment of xerostomia.11
CANDIDIASIS
Candida is a common microflora found in the oral cavity of as many as 60% of healthy adults.13 Certain conditions result in overgrowth of these organisms and lead to an infection called candidiasis. The most common causes of candidiasis are xerostomia, denture irritation, tobacco use, and steroid inhaler use. Many systemic factors increase the probability of this infection, including systemic corticosteroid use, chemotherapy, radiation therapy, endocrine disorders, malabsorption,
malnutrition, and antibiotic use.13,14 The clinical presentation of oral candidiasis varies and may manifest as white, red, or mixed white and red surface changes (Figure 3). The clinical symptoms can range from no symptoms, to a burning sensation, to altered taste. The most common presentation is whitish, curd-like plaques that can be wiped off with gauze, known as pseudomembranous candidiasis or thrush.14 In patients who wear dentures, candidiasis may appear as a flat or pebbly red lesion underneath the denture, which is called denture stomatitis. Fissures on the corners of the mouth, known as angular cheilitis or perlèche, are most often manifestations of Candida albicans. Median rhomboid glossitis, a form of erythematous candidiasis, is an asymptomatic lesion affecting the posterior dorsal surface of tongue13 (Figure 4).

Candidiasis can usually be diagnosed based on the patient’s history and clinical presentation. If needed, a cytologic smear of the lesion can be performed to confirm the diagnosis. A tissue biopsy and culture may also aid in yielding a diagnosis. Treatment for candidiasis involves topical or systemic antifungals. Typically, topical agents, such as nystatin oral suspension or clotrimazole troche, are effective. For patients with denture stomatitis, a topical antifungal can be applied on the mucosa covered by the denture and the denture base. Additionally, the patient should be referred to his or her dentist for evaluation of the denture. Denture wearers must be reminded to remove their dental prosthesis at night and clean it regularly.6,13
VESICULOEROSIVE DISEASES
Vesiculoerosive diseases are a group of blistering conditions that affect the oral mucosa, and may be immune-mediated inflammatory lesions. Lichen planus, erythema multiforme, and mucous membrane pemphigoid are most commonly seen in the mouth.14 Of these, lichen planus is most likely to affect the oral mucosa.

Oral lichen planus (OLP) is a relatively common, chronic immune-mediated condition usually affecting middle-aged women.15 The etiology of OLP remains obscure,16 however, it constitutes 9% of all white lesions affecting the oral cavity.17 The majority of patients with OLP have no associated skin or mucosal lichen planus, so this disease process is often referred to as isolated OLP. The oral clinical presentation is nearly always in a bilateral, more or less symmetrical pattern. The buccal mucosa (bilaterally) is the most typical site of involvement, however other panoral mucosal sites and the lips can also be involved.18 OLP is confined to the gingiva in about 10% of patients.19
Clinically, OLP may present as reticular, erosive, and plaque-like lesions, and these variants can co-exist within the same patient.16 The most common presentation includes pin-point white papules that gradually enlarge and come together to form a reticular or plaque-like pattern called Wickham’s striae. The erosive form of OLP may present with erythema caused by inflammation or epithelial thinning, or both, and ulceration/pseudomembrane formation with periphery of the lesion surrounded by reticular keratotic white striae18 (Figure 5). Gingival lesions frequently present with erythema and ulceration affecting the marginal and attached gingiva, as a manifestation of erosive lichen planus (Figure 6). The plaque form of OLP mimics leukoplakia in that it appears as a white, homogenous, slightly elevated, multifocal, smooth lesion.18
Patients with OLP may be asymptomatic or experience mucosal sensitivity, burning, and debilitating pain. Approximately two thirds of patients affected with OLP experience oral discomfort. Since OLP has periods of relapse and remission, during a period of exacerbation, there may be an increase in symptoms and clinical signs. An association between OLP and xerostomia has been established.20
The primary goal of OLP management is to alleviate symptoms on a long- and short term basis and to prevent and screen for malignant transformation.16 Although the World Health Organization currently regards OLP as a disease that may evolve into cancer, this theory is still controversial. Asymptomatic reticular lesions may require simple observation without any medical intervention. The most widely prescribed treatment for OLP is the use of topical steroids, which are often indicated for a prolonged period due to multiple symptomatic episodes.16
PROVIDING THE BEST CARE
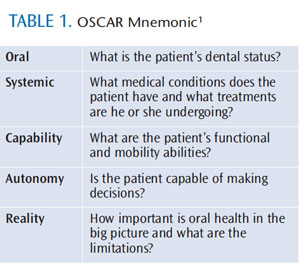
When treating older adults, certain critical factors need to be addressed before formulating a treatment plan and providing recommendations. The mnemonic “OSCAR” provides a helpful reference tool (Table 1).1 Older individuals may be more sensitive to trauma and pain, so local anesthesia should be considered during treatment. Maintaining communication with the patient’s primary physician and relevant specialists is also important to providing effective oral health care.
Dental diseases of the soft and hard tissue are largely preventable and can be reversible. Oral health professionals can make a significant difference in the oral health of older adults by helping them reduce risk factors, promoting a healthy lifestyle, advocating a noncariogenic diet, enhancing saliva production, and emphasizing the importance of routine oral hygiene and professional dental care.2
REFERENCES
- Laudenbach JM, Ship JA. In Laudenbach JM, ed. Clinician’s Guide Oral Health in Geriatric Patients. 3rd ed. Edmonds, Wash: American Academy of Oral Medicine; 2009.
- Dounis G, Ditmyer MM, McClain MA, Cappelli DP, Mobley CC. Preparing the dental workforce for oral disease prevention in an aging population. J Dent Educ. 2010;74:1086–1094.
- Boehm TK, Scannapieco FA. The epidemiology, consequences and management of periodontal disease in older adults. J Am Dent Assoc. 2007;138(Suppl):26S–33S.
- Cunha-Cruz J, Hujoel PP, Nadanovsky P. Secular trends in socio-economic disparities in edentulism: USA, 1972-2001. J Dent Res. 2007;86:131–136.
- Ettinger RL. Oral health and the aging population. J Am Dent Assoc. 2007;138(Suppl):5S–6S.
- Gonsalves WC, Wrightson AS, Henry RG. Common oral conditions in older persons. Am Fam Physician. 2008;78:845–852.
- Peters MC. Strategies for noninvasive demineralized tissue repair. Dent Clin North Am. 2010;54:507–525.
- Guggenheimer J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc. 2003;134:61–69.
- Ship JA, Pillemer SR, Baum BJ. Xerostomia and the geriatric patient. J Am Geriatr Soc. 2002;50:535–543.
- Turner MD, Ship JA. Dry mouth and its effects on the oral health of elderly people. J Am Dent Assoc. 2007;138(Suppl):15S–20S.
- Diaz-Arnold AM, Marek CA. The impact of saliva on patient care: A literature review. J Prosthet Dent. 2002;88:337–343.
- Crow HC, Ship JA. Are gingival and periodontal conditions related to salivary gland flow rates in healthy individuals? J Am Dent Assoc. 1995;126:1514–1520.
- Gonsalves WC, Chi AC, Neville BW. Common oral lesions: Part I. Superficial mucosal lesions. Am Fam Physician. 2007;75:501–507.
- Silverman S Jr. Mucosal lesions in older adults. J Am Dent Assoc. 2007;138(Suppl):41S–46S
- Nagao T, Ikeda N, Fukano H, Hashimoto S, Shimozato K, Warnakulasuriya S. Incidence rates for oral leukoplakia and lichen planus in a Japanese population. J Oral Pathol Med. 2005;34:532–539.
- Parashar P. Oral lichen planus. Otolaryngol Clin North Am. 2011;44:89–107.
- Greer RO, McDowell JD, Hoernig G. Oral lichen planus: a premalignant disease? Pro Pathol Case Rev. 1999;4:28–34
- Ismail SB, Kumar SK, Zain RB. Oral lichen planus and lichenoid reactions: etiopathogenesis, diagnosis, management and malignant transformation. J Oral Sci. 2007;49: 89–106.
- Mignogna MD, Lo Russo L, Fedele S. Gingival involvement of oral lichen planus in a series of 700 patients. J Clin Periodontol. 2005;32: 1029–1033.
- Colquhoun AN, Ferguson MM. An association between oral lichen planus and a persistently dry mouth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98:60–68.
From Dimensions of Dental Hygiene. March 2013; 11(3): 60–63.
