Help for Tension Headaches
Follow these strategies for effective prevention and treatment of this common ailment.
Tension-type headache (TTH) is the most common type of headache experienced worldwide.1 As a result, TTH significantly impacts disability rates, employee absenteeism, and, ultimately, socioeconomics. Research shows that the prevalence rates of TTH are astoundingly high. In a study of 1,000 participants, 78% reported experiencing TTH.2 Another study reported that 38% of adult participants had experienced a TTH at least once over the course of 1 year.3 TTH is most common among adults between the ages of 30 and 39; prevalence declines somewhat with advancing age. TTH is more common among women than men.3 Besides causing pain, TTH may also negatively affect quality of life and normal daily functioning. For example, one study of adult workers in Denmark demonstrated that TTH accounted for more than 10% of all reported absenteeism due to illness.4 The frequency of TTH, rather than severity of pain, has a greater impact on disability and quality of life.5
DENTAL HYGIENE CONNECTION
Dental hygienists may be especially susceptible to TTH due to the nature of their work. Sustained static postures of the shoulder and neck muscles may lead to dysfunctional myofascial trigger points (hyperirritable areas of a muscle that are tight and painful to palpation). Although it is still unclear what causes TTH, research points to a relationship between TTH and myofascial dysfunction. One study found that patients with TTH had more myofascial pain trigger points than a control group of healthy individuals.6 According to Fumal and Schoenen, the head pain experienced by patients with TTH is set off by active myofascial trigger points in the head, neck, and shoulder muscles.7 Increased firmness to palpation of the musculature surrounding the head and neck is also associated with chronic sufferers of TTH.8 The normal increase in blood flow that occurs in healthy muscle during exercise is limited among chronic sufferers of TTH, particularly in the upper shoulder muscle (trapezius).9 Collectively, these findings suggest that dental hygienists should take special care to maintain healthy upper body musculature in order to prevent TTH.
Musculoskeletal pain and dysfunction are not uncommon among dental professionals. In a study of 359 Swedish dentists, 72% reported pain and discomfort in the neck, shoulders, or head.10 Research also suggests that female dental professionals experience a higher rate of pain and discomfort in the neck and shoulder areas than males.11 In addition, 58.3% of 2,000 dentists surveyed in the United Kingdom said they experienced headaches. In these same subjects, 60% reported being nervous, tense, depressed, or experiencing sleeping difficulties, all of which were related to work stress.12
Emotional disturbances, stress, and mental health may be related to TTH. One study of individuals experiencing TTH demonstrated high levels of both anxiety and depression.13 Similarly, Gorter has reported a possible relationship between stress, job burnout, and physical symptoms among dental hygienists.14 In addition, a study of Australian and Swedish dental hygienists found that work stress was related to musculoskeletal pain, long working hours, and working with demanding and difficult patients.15 It seems plausible that the mental and physical stress of clinical practice may also contribute to TTH in dental hygienists.
TABLE 1. SYMPTOMS OF EPISODIC TENSION-TYPE HEADACHE
- Headache lasting from 30 minutes to 7 days
- At least two of the following pain characteristics: Bilateral location Pressing or tightening (nonpulsating) quality Mild or moderate intensity Not aggravated by routine physical activity, such as walking or climbing stairs
- Both of the following: No nausea or vomiting No more than one photophobia (abnormal intolerance to visual perception of light) or phonophobia (fear of loud sounds)
- Not attributed to another disorder
SYMPTOMS
According to the International Classification of Headache Disorders,16 there are three types of TTH based on frequency of attack: infrequent episodic TTH, frequent episodic TTH, and chronic TTH. Infrequent episodic TTH occurs 1 day or less per month, while frequent episodic TTH occurs between 1 day to 14 days per month for at least 3 months. Chronic TTH occurs 15 or more days per month. (See Table 1 and Table 2 for symptoms of episodic and chronic TTH.)
TABLE 2. SYMPTOMS OF CHRONIC TENSION-TYPE HEADACHE
- Headache that lasts hours or may be continuous
- Both of the following: No more than one of these symptoms: photophobia, phonophobia, or mild nausea
- No moderate or severe nausea or vomiting
TREATMENT AND PREVENTION
Proper treatment of any health problem involves an accurate diagnosis. Those experiencing any type of headache should first seek out a qualified physician to determine the cause of the pain. Headache can be a symptom of serious pathology. Once the diagnosis of TTH is given, several treatment options are available, including traditional pharmacological remedies, as well as nonpharmacological approaches.
TABLE 3. COMMON TRIGGERS FOR TENSION-TYPE HEADACHE
- Mental and physical stress
- Irregular or non-nutritious meal
- High intake of coffee/caffeine
- Dehydration
- Sleep disorders
- Too much or too little sleep
- Too much or too little physical exercise
- Psychological problems
- Variations in the menstrual cycle
- Hormonal substitution

Pharmacotherapy is effective in managing the symptoms of TTH, with acetaminophen remaining the drug of choice because it is typically less irritating on the gastrointestinal tract.17 Ibuprofen is the next pharmacological step, as nonsteroidal anti-inflammatory drugs (NSAIDS) are also effective in the treatment of TTH.18
Effective prevention of TTH involves avoiding factors that trigger the onset of pain. These triggers may include mental and physical stress and inappropriate physical exercise (Table 3).19,20
Most of these triggers can be successfully managed by living a healthy lifestyle. Simply eating a healthy diet and getting the proper amount of sleep may
reduce the incidence of TTH. Spierling reported that the most common precipitating factors for both migraine and TTH were lack of sleep, fatigue, not eating on time, and stress/tension.21 Controlling stress is key to any health and wellness plan. Though stress management can be a complicated process, simple techniques can be used to ease stress and enhance well-being.
Meditation is another stress management technique. Harvard cardiologist Herbert Benson, MD, developed a simple meditation technique ”the relaxation response” based on his study of the physiological changes that occur in Buddhist monks during their routine meditation practices. Benson describes the relaxation response as “a physical state of deep rest that changes the physical and emotional responses to stress… the opposite of the fight or flight response.”22 (Table 4 lists the steps to practicing this type of meditation.)
Yoga is a mind-body practice that also relieves tension in muscles and promotes stress relief. One study of subjects with chronic TTH looked at the effects of a yoga lifestyle program compared to pharmacological treatment using NSAIDS, and a third treatment group who received botulinum toxin injections into the temporalis—an important cranial muscle. The researchers found chronic TTH patients, compared with controls, had muscular hyperactivity in the temporalis muscle as measured through electromyography. The yoga-based intervention group showed the most significant reduction in temporalis muscle activity of the three treatment groups, indicating the muscle was more relaxed after this intervention. The yoga group also showed the greatest reduction in pain, dropping from an average of seven to two on a 10-point scale.23
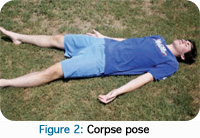
Yoga’s mountain pose is demonstrated in Figure 1. The corpse pose, perhaps the most relaxing of all yoga poses, is typically the last pose performed during a yoga routine (Figure 2). For both mountain and corpse poses, individuals should focus on the breath, and allow the body to relax completely. These are good yoga poses for the beginner because they do not involve strenuous physical positions and can be therapeutic both mentally and physically.
TABLE 4. STEPS TO ELICIT THE RELAXATION RESPONSE
- Sit comfortably in a quiet location with your eyes closed.
- Relax your body.
- Breathe through your nose.
- As you exhale, silently say to yourself the word “one.”
- Maintain a passive attitude (ie, don’t worry about reaching your goal of relaxation).
- Practice for 10 minutes to 20 minutes.
• Do not practice until 2 hours after eating a meal.
• Repeat once or twice a day.
CONCLUSION
TTH is the most prevalent type of headache and can cause significant disability. Dental hygienists are at risk of TTH due to prolonged static postures, and the mental and physical stress involved in professional dental hygiene practice. An accurate diagnosis is required by a physician who is experienced in TTH, and multiple treatment strategies may be effective. Dental hygienists should maintain a healthy lifestyle, including a nutritious diet, adequate sleep, stress management, and appropriate levels of physical activity, to avoid the pain associated with TTH.
REFERENCES
- Crystal SC, Robbins MS. Epidemiology of tension-type headache. Curr Pain Headache Rep. 2010;14:449-454.
- Rasmussen BK, Jensen R, Schroll M, Olesen J. Epidemiology of headache in a general population: a prevalence study. J Clin Epidemiol. 1991;44:1147-1157.
- Schwartz BS, Stewart WF, Simon D, Lipton RB: Epidemiology of tension-type headache. JAMA. 1998;279:381-383.
- Jensen R, Stovner LJ. Epidemiology and comorbidity of headache. Lancet Neurol. 2008;7:354-361.
- Cassidy EM, Tomkins E, Hardiman O, O’Keane V. Factors associated with burden of primary headache in a specialty clinic. Headache. 2003;43:638-64.
- Marcus DA, Scharff L, Mercer S, Turk DC. Musculoskeletal abnormalities in chronic headache: a controlled comparison of headache diagnostic groups. Headache. 1999;39:21-27.
- Fumal A, Schoenen J. Tension-type headache: current research and clinical management. Lancet. 2008;7:70-83.
- Ashina M, Bendtsen L, Jensen R, Sakai F, Olesen J. Muscle hardness in patients with chronic tension-type headache: relation to actual headache state. Pain. 1999;79:201-205.
- Fernandez-de-las-Penas C, Bueno A, Ferrando J, Elliott JM, Cuadrado ML, Pareja JA. Magnetic resonance imaging study of the morphometry of cervical extensor muscles in chronic tension-type headache.Cephalalgia. 2007;26:355-362.
- Rundcrantz BL, Johnsson B, Moritz U. Cervical pain and discomfort among dentists. Epidemiological, clinical and therapeutic aspects. Part 1. A survey of pain and discomfort. Swed Dent J. 1990;14:71-80.
- Rundcrantz BL, Johnsson B, Moritz U. Pain and discomfort in the musculoskeletal system among dentists. A prospective study. Swed Dent J. 1991;15:219-228.
- Myers HL, Myers LB. It’s difficult being a dentist: stress and health in the general dental practitioner. Br Dent J. 2004;197:89-93.
- Matta AP, Moreira Filho, PF. Depressive symptoms and anxiety in patients with chronic and episodic tension-type headache. Arq Neuropsiquiatr. 2003;61:991-994.
- Gorter RC. Work stress and burnout among dental hygienists. Int J Dent Hyg. 2005;3:88-92.
- Ylipaa V, Szuster F, Spencer J, Preber H, Sandelin Benko S, Arnetz BB. Health, mental well-being, and musculoskeletal disorders: a comparison between Swedish and Australian dental hygienists. J Dent Hyg. 2002;76:47-58.
- International Headache Society. The International Classification of Headache Disorders: 2nd edition. (ICHD-II). Cephalalgia. 2004;24:9-160.
- Langman MJ, Weil J, Wainwright P. Risks of bleeding peptic ulcer associated with individual non-steroidal anti- inflammatory drugs. Lancet. 1994;343:1075-1078.
- Ashina S, Ashina M. Current and potential future drug therapies for tension-type headache. Curr Pain Headache Rep. 2008;7:466-474.
- Rasmussen BK, Jensen R, Schroll M. Interrelations between migraine and tension-type headache in the general population. Arch Neurol. 1992;49:914-918.
- Ulrich V, Russell MB, Jensen R. A comparison of tension-type headache in migraineurs and in non-migraineurs: a population-based study. Pain. 1996;67:501-506.
- Spiering EL, Ranke AH, Honkoop PC. Precipitating and aggravation factors of migraine versus tension-type headache. Headache. 2001;41:554-558.
- Relaxation Response. Available at: http://relaxationresponse.org. Accessed August 25, 2011.
- Bhatia R, Dureja GP, Tripathi M, Bhattacharjee M, Bijlani RL, Mathur R. Role of temporalis muscle over activity in chronic tension type headache: Effect of yoga based management. Indian J Physiol Pharmacol. 2007;51:333-344.
From Dimensions of Dental Hygiene. September 2011; 9(9): 74, 76-77.

{kind=link}