
How to Encourage Change
Motivational interviewing can help patients improve their oral health habits.
This course was published in the September 2010 issue and expires 9/30/13. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Understand the guiding principles of motivational interviewing.
- Discuss how the principles of motivational interviewing impact oral health education.
- Identify the five stages of change and how each stage relates to behavior change.
- Critically assess how motivational interviewing and traditional oral health education approaches differ.
The Traditional Approach
Traditional oral health education is based on the dispensing of advice. The dental professional serves as the expert and may use an authoritarian approach.2,3 Frequently, education is provided while patients undergo clinical procedures in order to maximize the appointment time, even though headphones and other distractions can preoccupy patients. Dental professionals may follow up by asking, “Do you have any questions?” and briefly reinforce positive oral health habits.
Another traditional approach is to persuade patients to change behaviors.1 For example, a dental hygienist trying to convince a patient to floss might mention tooth loss or higher dental bills to persuade a patient to make a behavior change. Although this approach has a positive impact on knowledge, it has a small and temporary effect on plaque accumulation and oral health outcomes.4 Accurate information is necessary for patients to make decisions about behavior change, but information alone does not motivate most people to change their behavior.5 Individuals barraged by health information know they are at risk when choosing unhealthy foods, inactive lifestyles, and harmful substances, but still find it difficult to make healthy lifestyle changes.
Motivational Interviewing
MI, a counseling technique relatively new to dentistry, is a patient-centered alternative to persuasion and advice-giving.6 Originally designed to positively alter addictive behaviors, MI is typically used as an intervention for diseases that are influenced by lifestyle changes such as diabetes, obesity, heart disease, and early childhood caries.6-9 When treating chronic diseases, patient-centered interactions are more effective than doctor-centered interactions.9
Recently, Jönsson et al used MI in two experimental case studies to evaluate knowledge, oral hygiene habits, and individual oral health behavior goals to improve oral hygiene self-care in patients with chronic periodontitis.10 They found that MI was useful in designing interventions for the participants who needed to improve their periodontal health, but that additional, larger controlled clinical trials are required to support their findings. Alomomani et al found that a brief MI session (15 minutes to 20 minutes) before oral health education enhanced the education effect in individuals with severe mental illness.11
MI is based on the idea that when people verbally justify behavior change, they are more likely to follow through with it.12 The technique supports the patient’s autonomy and examines individual values, behaviors, and future goals to guide the process. MI also explores how a person feels about the status quo and change by exploring the patient’s perceptions and intrinsic motivation for change.2,3
Basic Principles
In order for MI to be effective, the patient must voice the argument for change rather than the health care professional.12 MI is both a counseling style and a set of clinical strategies that encourages patients to verbally express a desire for change and then to defuse resistance when it arises.2,12
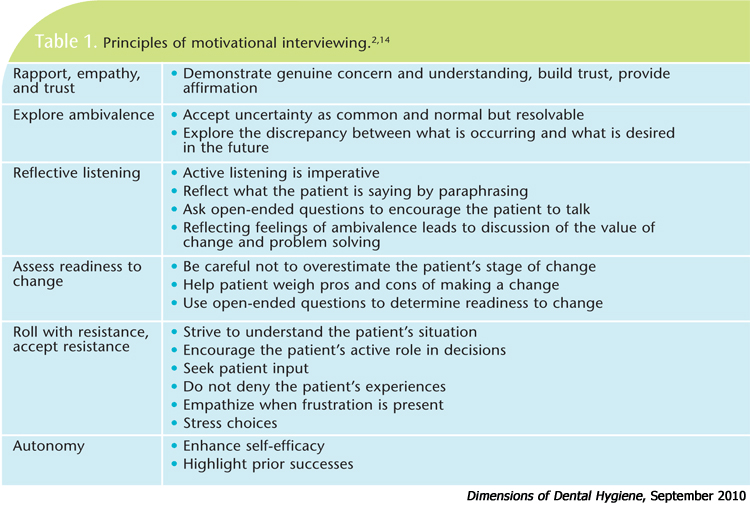
MI uses encouragement to resolve ambivalence about behavior change in a supportive environment without offering opinions for or against change.9 The guiding principles of MI include: 1) establishing rapport, 2) exploring ambivalence, 3) listening with reflection, 4) assessing readiness, 5) accepting resistance or reinforcing positive choices, and 6) allowing patient autonomy in decision-making (Table 1).13,14
Rapport. MI is based on establishing a relationship, showing empathy, and getting to know patients and their concerns. The interviewer asks open-ended questions encouraging patients to verbalize and discuss personal experiences, needs, and goals for oral health. For example, a clinician may ask a patient how she feels about her oral health and/or past dental experiences, or inquire about long-term goals for her child’s oral health.
Exploring ambivalence. MI allows individuals to explore problems in a supportive environment and discuss challenges and barriers from their perspective without influence. Reflecting a patient’s feelings of ambivalence can lead to a discussion of the value of change, potential barriers, and problem solving. For example, when a patient expresses concern about the time required for daily oral hygiene methods, the dental hygienist expresses empathy and verbally recognizes how busy and challenging the patient’s life is.
Reflective listening. Reflection is key to comprehending the patient’s needs and concerns. The dental hygienist simply summarizes or restates what the patient says, resisting the temptation to add what he or she thinks the patient “should” do. An important component of MI is facilitating behavior change by eliciting patient change talk. Hettema J et al note, “People change when they hear themselves talk about the need to change.”15
Readiness to change. Identifying a patient’s stage of change allows the practitioner to more accurately assist in promoting healthy changes or reinforcing maintenance behaviors. Table 2 provides information on the Stages of Change Model.
Rolling with resistance. Accepting resistance to change reduces negative emotions or defensiveness and promotes support and acceptance. A patient who is not ready to quit smoking will most likely resist smoking cessation suggestions. Trying to persuade the person to quit can create negative feelings and is often unsuccessful. Empathizing with the struggle and waiting until the patient is ready for cessation information is aligned with the principles of MI.
Autonomy. The last principle focuses on improving the patient’s confidence about behavior change.14 Once an individual states a desire to change, the clinician endorses the decision even if it is not ideal. The patient might suggest the possibility of reducing the number of cigarettes smoked each day rather than quitting. The dental hygienist then supports the patient in that goal and provides assurance that he will be successful even though this goal is not the desired outcome.
If a desired behavior change is identified, the interviewer asks permission prior to offering advice or information. Following permission or when information is requested, the clinician may provide choices that best suit each situation. For example, a patient who is a nonflosser and is extremely busy states she would like to keep her teeth. The clinician then asks, “Would you like me to show you an aid (or brush) that you might find easier to use and takes less time than using dental floss?” If permission is given, the dental hygienist can introduce the aid. Problem solving and identifying barriers can be accomplished by stating, “The aid still requires some time, but most people find it simple to use. Using it daily may help you reach your goal of keeping your teeth by slowing or arresting the progression of your periodontal disease. Would you like to try it? Do you foresee problems with using the aid?” If the patient declines, roll with resistance, strive to understand her situation, and stress the idea that she has choices.
Emphasizing the patient’s ability to make decisions and choose behaviors is imperative to the success of MI. Evidence indicates patient-centered approaches to health education have more profound results than traditional advice giving, especially when lifestyle changes are important.13
Weinstein et al successfully used MI in a community setting to decrease the number of new carious lesions in a group of children in Surrey, British Columbia.6 Two studies involving dental hygiene and dental students found MI had a positive effect on behavior change.16,17 Dental hygiene students learning MI-adherent behaviors demonstrated improvements in the use of MI in a pretest and post-test design over two patient education sessions.17 Koerber et al found clinically and statistically significant improvements in the MI skills of dental students who used an MI approach after 12 hours of training. Their skill improvement related to increased patient involvement in the counseling sessions.16
Stages of Change Model
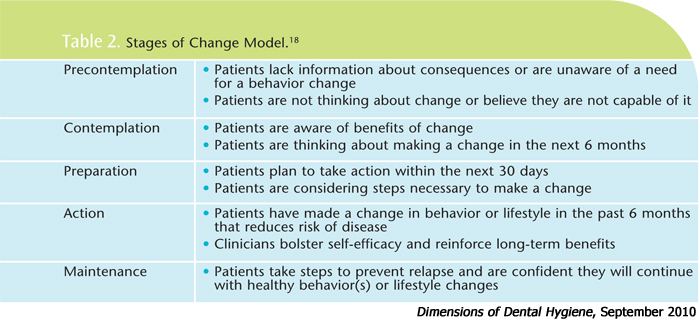
People vary in their readiness to change, therefore, practitioners should adapt their approach accordingly. The Stages of Change Model (Transtheoretical Model) asserts behavior change exists as a process rather than an event.6 This model proposes individuals move between five distinct stages: precontemplation, contemplation, preparation, action, and maintenance (Table 2).18 Any movement on the continuum of readiness to change is viewed as a positive short-term outcome. Movement is influenced by people’s confidence in their ability to change behaviors.14 At any time, individuals can relapse into a previous stage.

In the first stage of precontemplation, the person is not planning to make any changes and may not be aware of a need for change in behavior. People may be in precontemplation because they are un(der)informed or disillusioned by former unsuccessful attempts to change a behavior. In the contemplation stage, people are intending to alter an unhealthy behavior within the next 6 months. They are aware of both the pros and cons of making a change, so ambivalence or procrastination can keep them in this stage for a long time.
Those planning to take action or make a change in the next 30 days are in the preparation stage. Many times, a behavior change has been attempted in the past year. The individual has a plan for getting started. The action stage is when a change in behavior or lifestyle has occurred within the past 6 months. In this stage, the action the individual is taking to change a behavior must be adequate to obtain the desired personal or health outcome. In the maintenance stage, individuals are striving to prevent relapse. People tend to become more confident to continue with the change and are less likely to relapse in the maintenance stage.18
Gauging motivation and readiness for change are important considerations before offering suggestions. MI is more about listening than about imparting knowledge.13 Support should be offered and efforts affirmed regardless of the patient’s choices. If changes in oral health practices are selected, they should be discussed and the level of commitment should be determined. Research shows a correlation between the strength of commitment and health outcomes.12 The clinician might offer a menu of options for a mother of children with early childhood caries. Choices may include: using separate eating utensils when tasting or testing the child’s foods, giving the child a cup to use by age 1 year, and cleaning the child’s teeth as soon as they erupt.6 The patient can select one, suggest alternatives, commit to action, or choose not to change any behaviors. Taking the long-term view is important with MI.
Training
Weinstein et al describe MI as an approach that can be mastered with training and practice and that can be implemented by community workers as well as health care professionals.6 The counseling and psychology professions describe MI as a “complex clinical style” using a systematic and collaborative approach that requires therapeutic skill and necessitates training beyond attending a workshop, using a workbook, or reading and/or viewing videos.12,15
A common method for learning and incorporating MI into clinical practice is through brief professional training workshops that last from 1 day to 3 days. Such workshops typically include an introduction to the philosophy and principles of MI, demonstrations of the approach, guided practice in basic therapeutic principles and skills, and information regarding how to integrate the skills into practice. Evidence shows a direct relationship between the practitioner’s style and skills and patient behavior change.12
The skillful, consistent practice of MI leads to positive behavior changes in patients.12 To attain this level of competence, practitioners must continue their training in the technique.12,15 Workbooks and continuing education courses are available for clinicians interested in learning and reinforcing MI-style counseling techniques for oral health education.5,19,20
Conclusion
The spirit of MI is collaborative vs authoritarian, elicits the patient’s motivation, and respects the patient’s autonomy.12 MI requires a clinician to demonstrate genuine empathy and interest in the patient’s needs, and successful outcomes correlate closely with the clinician’s interpersonal skills. MI offers a new and interesting alternative for dental professionals. It is “far more about listening than telling, about evoking rather than instilling.”15 MI communicates not, “I have what you need,” but instead, “you have what you need, and together we will find it.”15
Acknowledgement
The author would like to thank Denise Bowen, RDH, MS, for her help with this manuscript.
References
- Harris N, Garcia-Godoy F, Nathe C. Primary Preventive Dentistry. 7th ed. Upper Saddle River, NJ: Pearson Prentice Hall; 2009:347-361.
- Miller WR, Rollnick S. Motivational Interviewing: Preparing People for Change. 2nd ed. New York: Guilford Press; 2002.
- Erickson SJ, Gerstle BA, Feldstein SW. Brief interventions and motivational interviewing with children, adolescents, and their parents in pediatric health care settings. Arch Pediatr Adolesc Med. 2005;159:1173-1180.
- Kay EJ, Locker D. Is dental health education effective? A systemic review of current evidence. Community Dent Oral Epidemiol. 1996;24: 231-235.
- Weinstein P. Motivate Your Dental Patients: A Workbook. Seattle: University of Washington; 2002.
- Weinstein P, Harrison R, Benton T. Motivating parents to prevent caries in their young children. J Am Dent Assoc. 2004;135:731-738.
- Greaves CJ, Middlebrooke A, O’Loughlin L, et al. Motivational interviewing for modifying diabetes risk: a randomized controlled trial. Br J Gen Pract. 2008;58:535-540.
- Resnicow K, Davis R, Rollnick S. Motivational interviewing for pediatric obesity: Conceptual issues and evidence review. J Am Diet Assoc. 2006;106:2024-2033.
- Stott NCH, Rollnick S, Rees MR, Pill RM. Innovation in clinical method: Diabetes care and negotiating skills. Fam Pract. 1995;12:413-418.
- Jönsson B, öhrn K, Oscarson N, Lindberg P. An individually tailored treatment programme for improved oral hygiene: introduction of a new course of action in health education for patients with periodontitis. Int J Dent Hygiene. 2009;7:166-175.
- Alomomani F, Williams K, Catley D, Brown C. Effects of an oral health promotion program in people with mental illness. J Dent Res. 2009;88: 648-652.
- Miller WR, Rose GS. Toward a theory of motivational interviewing. Am Psychologist. 2009;64:527-537.
- Britt E, Hudson SM, Blampied NM. Motivational interviewing in health settings: a review. Patient Educ Couns. 2004;53:147-155.
- Wagner CC, Ingersoll KS. Beyond cognition: broadening the emotional base of motivational interviewing. J Psychotherapy Integ. 2008;18:191-205.
- Hettema J, Steel J, Miller WR. Motivational interviewing. Ann Rev Clin Psychol. 2005; 1: 91-111.
- Koerber A, Crawford J, O’Connell K. The effects of teaching dental students brief motivational interviewing for smoking-cessation counseling: A pilot study. J Dent Educ. 2003;67:439-447.
- Croffoot C, Krust Bray K, Black M, Koerber A. Evaluating the effects of coaching to improve motivational interviewing skills of dental hygiene students. J Dent Hyg. 2010;84:57-64.
- Prochaska DO, DiClemente CC. Stage and processes of self-change of smoking: Toward an integrative model of change. J Consult Clin Psychol. 1983;51:390-395.
- Motivational Interviewing Resources for Researchers, Clinicians,and Trainers. Available at: www.motivationalinterview.org. Accessed July 30, 2010.
- Motivational Interviewing. Available at: www.mayo.edu/pmts/mc5300-mc5399/mc5383-07.pdf. Accessed July 30, 2010.
From Dimensions of Dental Hygiene. September 2010; 8(9): 60-65.
