All About Hand Instruments
Improving patient care and the dental hygienist’s work environment with new instrument technology.
The growing awareness of the link between oral and systemic health has increased the importance of providing accurate, complete, and comfortable periodontal assessment and treatment. Designs and materials of hand instruments for dental hygiene treatment are constantly changing and improving, providing dental hygienists with the challenge of finding the right instrument for each clinical situation.
Dental hygiene hand instruments can be divided into assessment and treatment categories. Assessment instruments are used to gather clinical data that allow the clinician to analyze the oral and periodontal health of the patient. Assessment hand instruments include mouth mirrors, periodontal probes, and explorers. Periodontal treatment hand instruments include curets, sickle scalers, and periodontal files. Some clinicians were also trained in the use of hoes and chisels but these instruments have largely been replaced by power instruments (ultrasonic and sonic scalers).
HANDLE CHOICE

A primary consideration in handle choice is clinician comfort, which is critical to lessen the effect of repetitive strain injuries. A wide variety of handles are available. Handles with larger diameters may prevent finger cramping and reduce hand fatigue.1 Many manufacturers offer a choice of metal or resin handles. Color-coding adds ease of identification of specific instruments in the tray set-up (Figure 1).1-3
Several factors determine the ease and comfort of instrument handle use:
1. Weight—hollow handles are lightweight and improve tactile sensitivity.
2. Diameter—ranges from 3/8” to 3/16” and may be round or hexagonal in cross-section. Large diameters are easier to hold and may reduce muscle fatigue.
3. Texture—texturing increases control and lessens hand fatigue.
4. Balance—working ends are aligned with the long axis of the handle. Balancing allows the finger pressure to be transferred more effectively to the working end, reducing muscle stress on the hands and arms.1
SHANKS
The shanks of an instrument are classified as simple (straight) or complex (angled).1 In general, simple shanks are designed for use in areas of easy access like the anterior teeth. The more complex or angled shanks are designed for areas that are more difficult to access, such as the posterior teeth. Shanks also vary in length and strength.
Long or extended shanks are designed to access deep periodontal pockets. Rigid, thick shanks are for removal of heavy calculus deposits. Flexible, thinner shanks provide greater tactile sensitivity and are used in the removal of fine calculus deposits and root debridement. A terminal shank extends between the working end and the first bend of the shank. Most instruments are designed for use with the terminal shank parallel to the root or crown being instrumented.
There is tremendous variation in the working end of dental hygiene instruments based on their usage, including differences in toe and tip length, angulation, cutting edges, and working strength. Many submarginal scaling instruments are designed with shorter, thinner working ends to allow access to deep, narrow periodontal pockets.
NEW DEVELOPMENTS IN ASSESSMENT INSTRUMENTS
Calibrated periodontal probes are marked in a variety of millimeter configurations and have many functions in the periodontal assessment. Probe tips can be circular or rectangular in cross-section. The PSR probe, modeled on the World Health Organization probe, has a small ball on the end, which improves patient comfort. Probe shanks may be flat, angled to access posterior regions, or curved (Nabers furcation probe).
 In the past, most probes were manufactured from stainless or carbon steel metal but many companies are now offering plastic probes for use with implants and for increased patient comfort. Some of the plastic probes have pressure indicators that show the clinician when the appropriate amount of pressure is being used. A band of color representing a certain number of millimeters greatly improves visibility. Nabers furcation probes are now also available with color-coded bands at 3 mm intervals, making the probe much easier to read (Figure 2).
In the past, most probes were manufactured from stainless or carbon steel metal but many companies are now offering plastic probes for use with implants and for increased patient comfort. Some of the plastic probes have pressure indicators that show the clinician when the appropriate amount of pressure is being used. A band of color representing a certain number of millimeters greatly improves visibility. Nabers furcation probes are now also available with color-coded bands at 3 mm intervals, making the probe much easier to read (Figure 2).
Explorers have flexible wire-like working ends that transmit vibrations as they are moved over tooth surface irregularities. Accurate submarginal calculus detection is dependent on the tactile sensitivity of the clinician, making the explorer invaluable for complete deposit removal. The development of an explorer angled like a Gracey 11/12 curet has greatly improved calculus detection. Extended shank explorers are designed to access deep periodontal pockets.1

AREA SPECIFIC CURETS
 Area specific curets have a tilted face in relation to the terminal shank. This tilt or offset allows the lower cutting edge of the area-specific curet to be at the correct angulation when the lower shank is parallel to the instrumented tooth surface.1 This angulation and the curved toe and back of the Gracey curet allow submarginal instrumentation without tissue trauma. Each of the area-specific curets is designed to adapt easily to the difference in curvature between the anterior and posterior teeth and the mesial, distal, lingual, and facial surfaces.
Area specific curets have a tilted face in relation to the terminal shank. This tilt or offset allows the lower cutting edge of the area-specific curet to be at the correct angulation when the lower shank is parallel to the instrumented tooth surface.1 This angulation and the curved toe and back of the Gracey curet allow submarginal instrumentation without tissue trauma. Each of the area-specific curets is designed to adapt easily to the difference in curvature between the anterior and posterior teeth and the mesial, distal, lingual, and facial surfaces.
Gracey curets were originally designed with a flexible shank to improve tactile sensitivity and to remove light calculus; these are often called finishing curets.4 Graceys are also manufactured with a rigid shank for moderate to heavy calculus removal. Recent additions to the original 14 working ends are the Gracey 15/16 and 17/18. The Gracey 15/16 is a modification of the 11/12 with a more acutely angled shank to access the mesial surfaces of posterior teeth, especially the mandibular premolars. The extra angulation allows better adaptation and a more stable intraoral fulcrum. The Gracey 17/18 is a modified 13/14 with a 3 mm elongation of the termination shank and a 1 mm shorter blade to provide better access and adaptation to posterior distal surfaces.4
The original Gracey series has seen many evolutions, including rigid and extended shanks, mini working ends, and markings on the shank.
A slightly different adaptation of the Gracey curet is the Turgeon curet, which has a narrower working end and a modified cross-section that some clinicians find easier to sharpen with its triangular cross-section (Figure 3).1
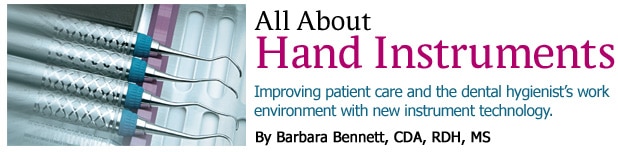
 The O’Hehir New Millennium (PDT/Paradise Dental Technologies Inc, Missoula, Mont) debridement curets are an innovative type of area-specific curet designed to remove light residual calculus deposits and decontaminate the root surface (Figure 4). Similar to spoon excavators or cleoid-discoid restorative instruments, these instruments are used with gentle push or pull strokes in any direction. The instrument has an extended lower shank for easy access into deep periodontal pockets and the working end is a tiny three-dimensional circular disk that adapts easily to furcations, line angles, and developmental grooves.1
The O’Hehir New Millennium (PDT/Paradise Dental Technologies Inc, Missoula, Mont) debridement curets are an innovative type of area-specific curet designed to remove light residual calculus deposits and decontaminate the root surface (Figure 4). Similar to spoon excavators or cleoid-discoid restorative instruments, these instruments are used with gentle push or pull strokes in any direction. The instrument has an extended lower shank for easy access into deep periodontal pockets and the working end is a tiny three-dimensional circular disk that adapts easily to furcations, line angles, and developmental grooves.1
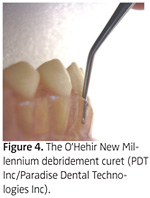
Another new area-specific curet designed to access mesial and distal surfaces of anterior teeth, line angles, and primary teeth is the Y-ME Curette (Hu-Friedy Mfg Co Inc) (Figure 5). The contra-angle shank and the 70° off-set blade allow excellent angulation. It is also part of the EverEdge® line, designed for less sharpening and less hand fatigue.
UNIVERSAL CURETS
Because they can be used on both anterior and posterior teeth, universal curets are one of the most frequently designed and most versatile of all the instruments used for calculus removal.1 The universal curet has a rounded back and toe and is semicircular in cross-section, with the face at a 90° angle to the lower shank. Unlike the Gracey, universal curets have two cutting edges that are level to each other. Many innovative designs have been introduced in addition to the traditional favorites—the Columbia 13/14 and Barnhart 5/6—such as the Columbia 4R-4L and the 2R-2L (Figure 6).
 The Langer curets are a hybrid of the universal curets with the area-specific feature of the Gracey curet series. They have a long, complex shank design. The working end has a face that is 90° to the lower shank, with two parallel working and cutting edges. The Langer curets must be used in a set to access the entire dentition and are available in standard, rigid, extended shank, and mini working end versions. The combination of the universal and area-specific designs prevents the Langer from being a balanced instrument and adaptation of the posterior Langers may be difficult in patients who have difficulty in opening widely.1
The Langer curets are a hybrid of the universal curets with the area-specific feature of the Gracey curet series. They have a long, complex shank design. The working end has a face that is 90° to the lower shank, with two parallel working and cutting edges. The Langer curets must be used in a set to access the entire dentition and are available in standard, rigid, extended shank, and mini working end versions. The combination of the universal and area-specific designs prevents the Langer from being a balanced instrument and adaptation of the posterior Langers may be difficult in patients who have difficulty in opening widely.1
Other universal series the clinician may wish to try include the Younger-Good series (Figure 7), the Goldman-Fox series (Figure 8), and the Quetin furcation series. Each has its own advantages and disadvantages.
Many manufacturers are combining the universal with a sickle tip as one instrument, improving scaling efficiency for patients with small amounts of calculus concentrated in the anterior region of the mouth. One such instrument is the HL-55 sickle/universal curet (PDT/Paradise Dental Technologies Inc), which is similar to an anterior Gracey but with two cutting edges. It also comes in a mini curet version for tight tissue.
PERIODONTAL FINISHING INSTRUMENTS
Diamond burs have long been the premier choice for restorative dentistry and now several manufacturers are using this technology for finishing files for periodontal therapy. These diamond-coated files have different angulations for access to all root surfaces.
IMPLANT INSTRUMENTS
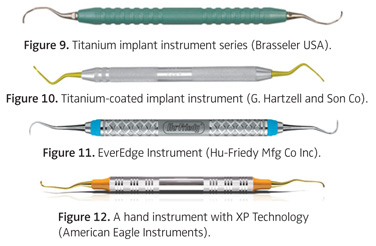
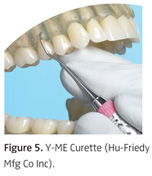
Trying to remove a tenacious calculus deposit from an implant with a graphite or plastic instrument is extremely difficult. A new solid titanium implant instrument series (Brasseler USA) is available that does not damage the implant surface, yet is able to effectively remove the deposit (Figure 9). G. Hartzell and Son Co makes titanium-coated implant instruments that are rigid and they have a stainless steel core underneath the titanium coating to increase rigidity (Figure 10).
SHARPENING
Although sharpening instruments is much easier than in the past, it is still a challenging task that must be worked into busy schedules. Today’s dental hygiene scaling instruments tend to stay sharper longer due to improved formulations of the metals. Hu-Friedy has patented EverEdge technology for its new stainless steel alloy instrument series (Figure 11). The instruments are designed to stay sharper 50% longer than other instruments. Although the instrument stays sharper longer, it may be sharpened many times throughout the life of the instrument and will retain its sharpness longer after sharpening than traditional instruments. The EverEdge technology is available in many of the scaling instrument designs.
American Eagle Instruments, offers XP Technology instruments that never need to be sharpened (Figure 12). The XP curets are treated with a patented process that hardens the stainless steel and then encapsulates the steel with a diamond-like layer, making an edge that lasts for months. The blades are thinner for easier insertion and patient comfort. These instruments are discarded when they become dull.
Sharper instruments minimize the amount of time and effort that the clinician must spend to remove calculus deposits, and may reduce the likelihood of repetitive motion injuries. These instruments are designed for use on moderate to light calculus deposits and root debridement. Both manufacturers suggest that best results are achieved by using a light touch with less pressure than traditional curets.
SUMMARY
Today’s dental hygienist can choose from a vast array of instrument designs and materials to make periodontal therapy less fatiguing and more comfortable for both the clinician and the patient. The new technology in hand instruments makes it possible for the hygienist to improve the quality of treatment for the patient while improving the work environment simultaneously.
REFERENCES
- Nield-Gehrig JS. Fundamentals of Periodontal Instrumentation and Advanced Root Instrumentation. 6th ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2007:149-163, 219-531.
- Darby ML, Walsh MM. Dental Hygiene Theory and Practice. 2nd ed. St. Louis: Saunders; 2003:399-425.
- Wilkins EM. Clinical Practice of the Dental Hygienist. 9th ed. Baltimore, Md: Lippincott, Williams, and Wilkins; 2004:225-237, 610-625.
- Newman MG, Takei HH, Carranza FA. Carranza’s Clinical Periodontology. 9th ed. Philadelphia: WB Saunders Co; 2002:6, 567-579.
*Rota-Dent One Step®, Pro-Dentec®, a Zila Inc Co, Batesville, Ark
From Dimensions of Dental Hygiene. November 2007;5(11): 20-23.

{kind=link}