A Matter of Taste
Medication use can cause significant taste disturbances. Here’s how to best advise your patients about this condition.
This course was published in the March 2012 issue and expires March 2015. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Discuss the mechanism of taste.
- Define the different classifications of taste disturbances.
- Identify the classes of drugs that can cause taste disturbances.
- Detail possible treatments of taste disturbances.
More than 2 million Americans—mostly older adults—suffer from some type of taste disturbance or chemosensory deficiency.1 Every year approximately 200,000 patients complain of a chemosensory loss or defect to their health care providers. Of these patients, an estimated 22% will not have a readily apparent cause.2 Frequently, dental professionals are the first to assess this dysfunction.
Dental hygienists will most likely encounter patients with taste disturbances and should have a basic understanding of their etiology and treatment. Taste disturbances can originate from many different factors beyond the typical culprits of periodontitis, caries, and volatile sulfur compounds (Table 1),3 but medication use is one of the most commonly overlooked causes. Many prescription drugs, over-the-counter medications, herbal supplements, vitamins, and minerals can create taste disturbances in otherwise healthy oral cavities.1,4
Mechanism of Taste
Humans are able to experience taste through taste buds that are located throughout the oral cavity, mainly the tongue, but also the throat, larynx, and esophagus. Each taste bud is composed of 50 taste receptor cells to 100 taste receptor cells that detect chemicals from food and drink which have dissolved into saliva. The information is then passed through sensory nerves to the brain where it is interpreted by the cerebral cortex (Figure 1). Humans have approximately 10,000 taste buds, and they are replaced every 10 days. The smell and texture of foods/drinks also contribute to taste.5,6
Taste Disorders
A taste disorder is broadly defined as diminished discrimination of the primary taste qualities: sweet, bitter, sour, salty, and umami (savory).1 There are four specific classifications of taste disorders. Ageusia, which is rare, is the total absence of one or more of the basic taste sensations. Ageusia is sometimes confused with anosmia (inability to smell odors), because up to 75% of food’s flavor is obtained through smell. Parageusia is a perception of foul or spoiled food. Dysgeusia, the most common drug-induced taste abnormality, is a distorted sense of taste, such as a metallic taste. The aberrant sensation often persists and produces inconsistency in expected tastes. Finally, hypogeusia is a partial loss of taste that often goes unrecognized by patients.2,7,8
Table 1. Possible Causes of Taste Disturbance Besides Medication Use.3
- Oral and perioral infections, eg, candidiasis, gingivitis, herpes simplex, periodontitis, sialadenitis
- Bell’s palsy
- Oral appliances, eg, dentures, restorative materials
- Dental procedures, eg, tooth extraction, root canal
- Age
- Nutritional factors
- Tumor or lesions associated with taste pathways
- Head trauma
- Toxic chemical exposure
- Industrial agent exposure
- Radiation treatment of head and neck
- Psychiatric conditions
- Epilepsy
- Migraine headache
- Sjögren’s syndrome
- Multiple sclerosis
- Endocrine disorders
Xerostomia is not a defined taste disturbance, but it can cause taste alteration because normal salivary flow is necessary for taste. Drugs that commonly cause dry mouth include those with anticholinergic properties, such as tricyclic antidepressants (amitriptyline, imipramine) and antihistamines (chlorpheniramine, diphenhydramine).2 Because zinc is necessary in the production of new taste buds, its deficiency may also cause taste disturbances. Certain medications lower the amount of zinc in the blood (Table 2).9 Table 3 lists other possible mechanisms of drug-induced taste disturbance.4,8
Prevalence
Establishing the prevalence, incidence, or even causality in many cases of taste disturbances is difficult because of several factors.10 Little research has been conducted, and many reports of taste disturbances are anecdotal.10 Dysgeusia often spontaneously resolves, and not all patients taking drugs that cause taste disturbances experience symptoms.10 For example, because hypertensive drugs are taken most often by older adults and taste and smell sensations decrease with age, a report of a diminished taste or smell function could reflect age-related factors, including hypertension. The incidence of drug-induced taste disturbances has been reported as high as 11% and as low as 3%.8 Tomita and Yoshikawa reported that in their clinic, approximately 25% of their patients experienced taste disturbances.11
Table 2. Medications That May Reduce the Amount of Zinc in the Blood.9</sup
- Angiotensin-converting-enzyme (ACE) inhibitors
- Cisplatin (chemotherapy drug)
- Deferoxamine (removes excess iron from the blood)
- Penicillamine (used to treat Wilson’s disease and rheumatoid arthritis)
- Thiazide diuretics (water pills)
Common Drug Classes
The list of drugs that can affect taste is vast, with virtually every therapeutic class represented. While there is limited data from clinical trials, there does appear to be several common culprits. Table 4 includes a list of drugs frequently implicated in taste disturbances.1,2,8,11-14 However, this list is not comprehensive and many others drugs may cause taste disturbances.
Treatment of Taste Disturbance
Treating taste disorders is difficult because the factors involved are varied, difficult to quantitate, and subjective. The most common approach is to stop taking the suspected medication, however, this is not always feasible and may not result in an immediate return to normal taste sensation.2 The onset of taste disturbance caused by medication use is likely patient specific, ie, some patients may experience symptoms immediately after ingesting the drug while others don’t experience symptoms until months later.13
Table 3. Possible Mechanisms of Drug-Induced Taste Disturbances.4,8
- Alterations in saliva and its chemical composition
- Altered neuronal impulse propagation (eg, by neuron demyelination, perineural inflammation or influencing calcium flux)
- Changes in higher-order cortical processing of chemosensory input
- Damage to taste receptors by direct or secondary processes (eg, gastroesophageal reflux disease)
- Disturbances in neurotransmitter functioning
- Drying of the oral mucosa, causing a reduction in chemical access to receptor sites
- Immunosuppression and related sequellae
- Increasing local bradykinin concentration
- Inducing deficiency of zinc and copper
- Unpalatable taste of the drug itself (eg, clindamycin suspension)
Taste disturbances may persist for a significant period after withdrawal of the offending agent.2 One report noted that a
patient taking terbinafine, a medication used to treat nail-based fungal infections, did not recover normal taste function for 3 years after discontinuing its use.14 A separate case report suggests angiotensin-converting enzyme (ACE) inhibitors (used to treat hypertension) may cause irreversible damage to taste perception.15 Unfortunately, therapeutic options are limited to ceasing the offending medication, dosage reduction if the medication cannot be stopped, switching to an agent within the same therapeutic class, and mineral supplementation.2 Zinc supplementation is an intuitive option, but the literature suggests its use provides modest benefits at best, and randomized clinical trials have produced conflicting results.1 Only patients who have true zinc deficiency are likely to experience benefits, and it may take several weeks of supplementation before any positive effects are noted.2,16 Other options for patients who have persistent dysgeusia include the use of lozenges or sugarless gum to mask the taste. Lozenges containing oral anesthetics, such as dyclonine, found in over-the-counter cough suppressants are frequently employed.2 Finally, if xerostomia is thought to be the inciting factor, artificial saliva or cholinergic agents, such as pilocarpine, may help.2
Consequences
Unfortunately, therapeutic options are limited to ceasing the offending medication, dosage reduction if the medication cannot be stopped, switching to an agent within the same therapeutic class, and mineral supplementation.2 Zinc supplementation is an intuitive option, but the literature suggests its use provides modest benefits at best, and randomized clinical trials have produced conflicting results.1 Only patients who have true zinc deficiency are likely to experience benefits, and it may take several weeks of supplementation before any positive effects are noted.2,16 Other options for patients who have persistent dysgeusia include the use of lozenges or sugarless gum to mask the taste. Lozenges containing oral anesthetics, such as dyclonine, found in over-the-counter cough suppressants are frequently employed.2 Finally, if xerostomia is thought to be the inciting factor, artificial saliva or cholinergic agents, such as pilocarpine, may help.2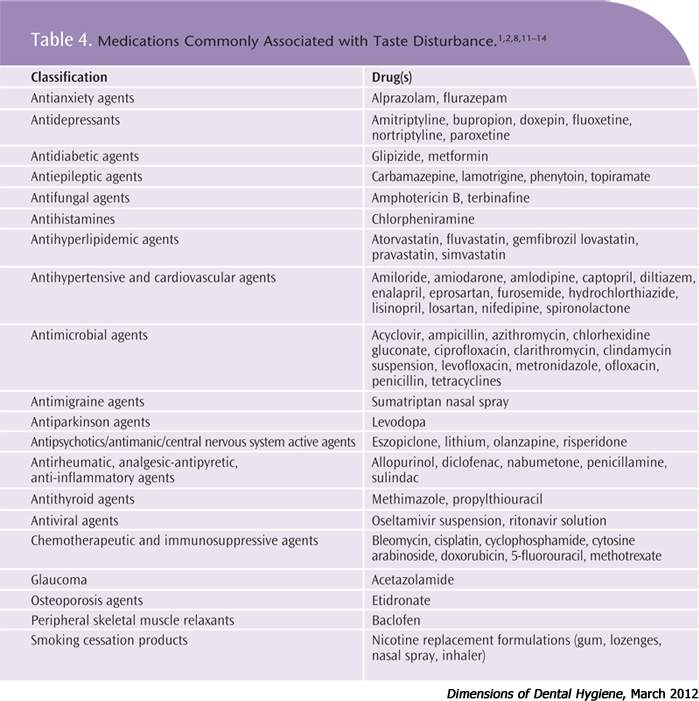
While complaints of taste disturbance may seem benign on the surface, it can have drastic health consequences. Many patients may try to compensate by increasing fluid intake or increasing their use of salts or sugars. These compensatory mechanisms, such as over-salting or over-sweetening food, can translate into harmful health effects including poorly controlled hypertension or diabetes, exacerbated cardiovascular disease, or dental caries. Persistent taste impairment can also have a significant impact on nutritional intake.
When a patient complains of altered taste, taking a thorough history of the problem is essential. Some questions to consider include:
- How long has the taste disturbance been happening?
- What type of altered taste are you experiencing?
- Did this begin after you started taking any prescribed, herbal, or over-the-counter medication?
- Were you advised by your health care provider that this drug may cause an altered taste?
Because taste disturbance is often caused by medication use, dental hygienists must be able to investigate symptoms in a drug reference resource as part of the differential decision making process. By thoroughly addressing these problems with their patients, dental hygienists can make a difference before serious side effects occur.
Sample Case Report
A 62-year-old, previously healthy man presented with the chief complaint of a “bad taste” in his mouth. During the medical history review, he reported that he had been recently diagnosed with hypertension and was prescribed captopril, a drug used to treat high blood pressure and heart failure by decreasing specific chemicals that constrict the blood vessels. His blood pressure at the dental appointment was 156/94, indicative of stage 1 hypertension.
His extraoral and intraoral exams were within normal limits and showed no signs of candidiasis, thus fungal infection was eliminated as a cause. He had two areas of bleeding on probing and his clinical attachment levels remained stable from his last visit. No carious lesions were detected radiographically or clinically. After interviewing the patient, it was determined that the timing of his ingesting captopril coincided directly with the presence of symptoms. The dental team collaborated with the patient’s physician to find another blood pressure medication that might not cause the same symptoms. The patients switched medications, and within 1 month, the taste disturbance symptoms were ameliorated.
PHOTO CREDITS:
HEADER IMAGE: SCIENCE PHOTO – TONGUE TASTE BUDS, LIGHT MICROGRAPH
FIGURE 1: FRANCIS LEROY, BIOCOSMOS/SCIENCE PHOTO LIBRARY
REFERENCES
- Mott AE, Grushka M, Sessle BJ. Diagnosis and management of taste disorders and burning mouth syndrome. Dent Clin North Am. 1993;37:33-71.
- Ackerman BH, Kasbekar N. Disturbances of taste and smell induced by drugs. Pharmacotherapy. 1997;17:482-496.
- Bromley SM. Smell and taste disorders: a primary care approach. Am Fam Phys. 2000;61:427-436.
- A better understanding of drug-induced taste disturbances may improve management of the condition. Drugs and Therapy Perspectives. 2008;24(12):22-24.
- Feske SK, Samuels MA. Office Practice of Neurology. 2nd ed. Philadelphia: Elsevier Science; 2003:114.
- Mann NM. Management of smell and taste problems. Cleve Clin J Med. 2002;69:334.
- WebMD. Taste Changes — Topic Overview. Available at: www.webmd.com/a-to-z-guides/taste-changes-topic-overview. Accessed February 7, 2012.
- Naik BS, Shetty N, Maben EV. Drug-induced taste disorders. Eur J Intern Med. 2010;21:240-243.
- Saper R, Rash R. Zinc: An essential micronutrient. Am Fam Physician. 2009;79:768-772.
- Doty RL, Bromley SM. Effects of drugs on olfaction and taste. Otolaryngol Clin North Am. 2004;37:1229-1254.
- Tomita H, Yoshikawa T. Drug-related taste disturbances. Acta Otolaryngol Suppl. 2002;546:116-121.
- Hummel T, Welge-Lussen A, eds. Taste and Smell: An Update. Adv Otorhinolaryngol. Basel, Karger. 2006;63:265-77.
- Henkin RI. Drug-induced taste and smell disorders. Incidence, mechanisms and management related primarily to treatment of sensory receptor dysfunction. Drug Saf. 1994;11:318-377.
- Bong JL, Lucke TW, Evans CD. Persistent impairment of taste resulting from terbinafine. Br J Dermatol. 1998;139:747-748.
- Coulter DM. Eye pain with nifedipine and disturbance of taste with captopril: a mutually controlled study showing a method of postmarketing surveillance. Br Med J. 1988;296:1086-1088.
- Heyneman CA. Zinc deficiency and taste disorders. Ann Pharmacother. 1996;30:186-187.
From Dimensions of Dental Hygiene. March 2012; 10(3): 60-63.
