
Exercise May Be the Missing Link in the Fight Against Musculoskeletal Disorders
New research suggests that regular physical activity may help dental hygienists reduce pain, improve function, and extend career longevity.
Dental hygienists often experience repetitive strain injuries.1-13 The upper extremities, neck, and back regions of the body are often overexerted, sustained in static postures for long periods, and exposed to cumulative trauma which may contribute to persistent pain, fatigue, and functional limitations.
Additionally, the demanding nature of dental hygiene schedules often does not allow for adequate recovery time between loading of the same muscles, ligaments, tendons, and joints.14,15 Because many of these risk factors are unmodifiable, developing interventions for reducing musculoskeletal (MSD) risk and manging pain is critical. Operatory adjustments, clinician and patient positioning, magnification, and ergonomic instrument designs remain essential for MSD prevention, however these strategies may not fully address the cumulative biomechanical strain that occurs clinically. Therefore, exercise-based mitigation strategies should be part of a comprehensive approach to supporting ergonomic health.
Exercise and Prevention of Repetitive Strain Injuries
While ergonomic equipment and positioning may reduce unnecessary exposure to risk factors, exercise may improve the body’s ability to tolerate unavoidable exposures. A promising area of research is the use of exercise programs to address pain and MSD risk.16-21
In a recent systematic review, Van Eerd et al17 summarized the effectiveness of various interventions, including exercise programs, to reduce MSD risk. Findings demonstrated strong, positive effects of resistance training, such as dumbell and kettleball routines, on MSD risk or pain reduction. Overall, results indicated strong evidence for resistance training in preventing work-related MSDs and pain. For dental hygienists, resistance training may be especially relevant because it can improve muscle endurance, postural stability, shoulder and trunk control, grip force capacity, and overall tolerance to repeated muscular loading.
The systematic review also included six studies with moderate to strong evidence supporting stretching exercise programs for reducing MSD risk and pain.17 In dental hygiene, research has indicated stretching may prevent MSD development and pain.16-21 With static and awkward postures that often lead to fatigue, overloading of muscles, and overcompensation of antagonist muscles, stretching could allow for recovery or pain reduction with counteractivation of the muscles overutilized in repetitive dental hygiene tasks.22 Based on current evidence, chairside stretching exercises performed between patients may represent a practical strategy for reducing MSD risk.17-21
Dental hygienists may benefit from incorporating exercise programs into their daily routine as a group at the end of the day.17 The group accountability may lead to successful implementation and continued use of exercise intervention strategies; however more research is needed.
Researchers explored exercise interventions specifically among oral health professionals in a 2020 systematic review that included 34 studies.19 Results indicated most physical activity interventions, such as aerobic exercise, yoga, stretching, and general physical activity, were associated with a reduction in MSD pain and frequency. Home exercise routines may support body awareness, breathing regulation, stress management, and recovery from sustained occupational demands.19
One study found that exercise reduced back pain among dental students, suggesting that interventions for MSDs should begin during professional education.20 Although these findings suggest that physical activity may help reduce MSD pain, a significant limitation is that most studies included participants who already had MSD symptoms, limiting conclusions about its preventive effects.17-21
Further research should explore exercise as a prevention strategy rather than reduction strategy for MSD pain, as well as the specific types and intensities of exercise that may be best for MSD prevention. Regardless, many dental hygienists experience MSD pain1–12 and regular exercise can help reduce these symptoms.16-23
Impact of Stretching
Stretching may also reduce MSD risk.16-21 Nye et al21 examined the effects of chairside stretching exercises by dental hygiene students who were divided into a control group and a stretching intervention group. Researchers found significant differences in self-reported musculoskeletal pain between the control group and treatment group who completed chairside stretching interventions. Interestingly, participants felt neutral about the impacts of chairside stretching on pain. They also reported feeling more aware of their positional ergonomics because of the study, which may have impacted the findings.
Another study demonstrated positive effects on musculoskeletal pain in oral health professionals after stretching interventions.19 The study of dental hygienists and dentists included 27 participants in the control group and 27 subjects in the stretching intervention group. Stretching interventions were guided by a physical therapist for 30 minutes following a workday. Pain pressure threshold tests were completed on both groups at the end of each day. Oral health professionals who participated in the study demonstrated statistically significant increases in pain pressure thresholds at multiple body sites, along with reductions in overall pain.
These studies indicate a positive association with stretching and a reduction in MSD pain and development.21 Dental hygienists should consider incorporating stretching into routines as a preventive and pain-reduction strategy; however, persistent or worsening symptoms may require evaluation and treatment beyond self-directed stretching alone.
When Pain Persists
While exercise may be an appropriate first-line strategy for reducing MSD risk and symptom management, dental hygienists should see a physical or occupational therapist when pain persists, worsens, or begins to interfere with clinical practice or daily function. When persistent numbness, tingling, loss of finger or hand grip strength, pain that interferes with work or home tasks, or symptoms that continue despite self-mitigation strategies are present, medical consult and intervention are necessary.
Physical and occupational therapists can assess individual movement impairments, identify contributing ergonomic and workload factors, prescribe progressive strengthening exercises, and provide adjunctive interventions, such as manual therapy.24,25 Manual therapy encompasses hands-on techniques, including joint mobilization, soft tissue mobilization, myofascial release, and manual stretching, with the goal of reducing pain, improving mobility, and restoring musculoskeletal function.
Research suggests that manual therapy combined with stretching and strengthening may improve pain, range of motion, and functional capacity more effectively than exercise alone. Therefore, stretching should be viewed as one component of a broader prevention and management approach.24,25 Given the cumulative nature of occupational MSD risk in dental hygiene, prevention strategies are likely most effective when they are integrated into a daily routine before symptoms become severe or functionally limiting.
![]() Exercise Strategies
Exercise Strategies
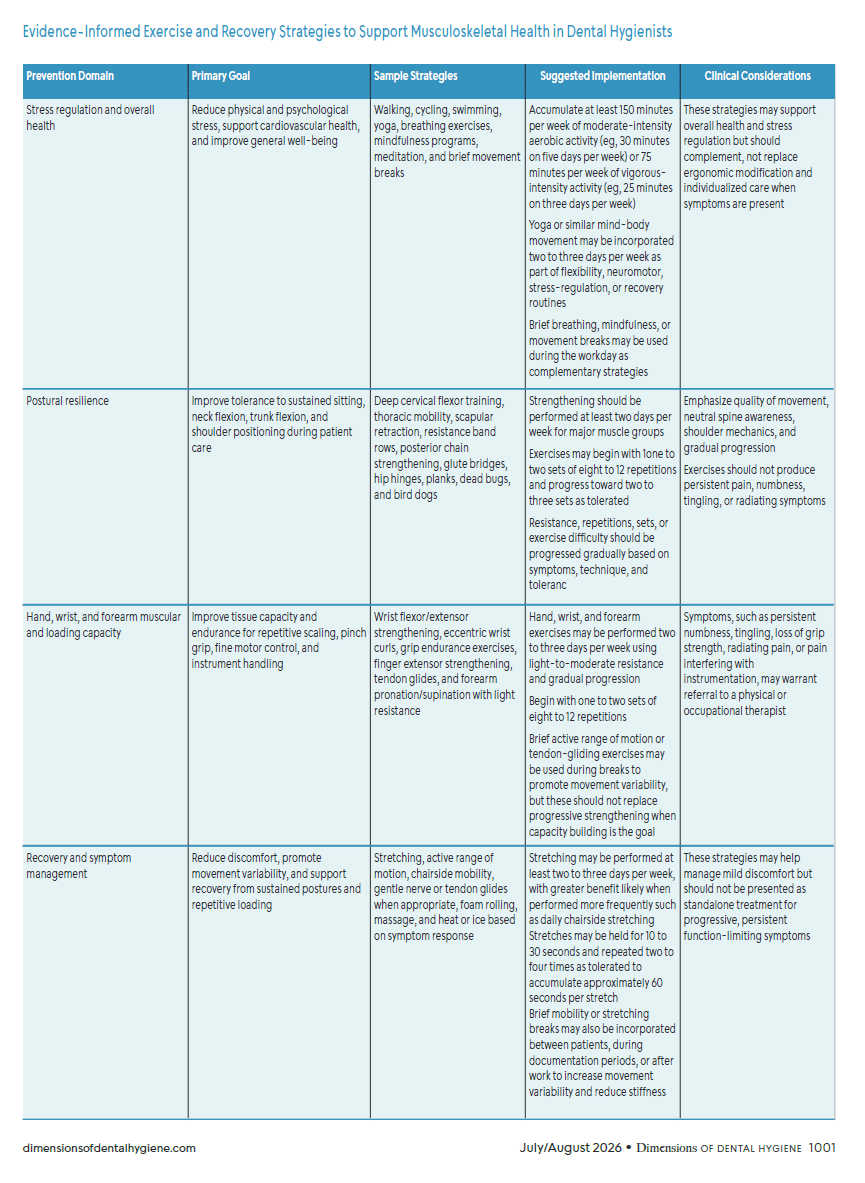
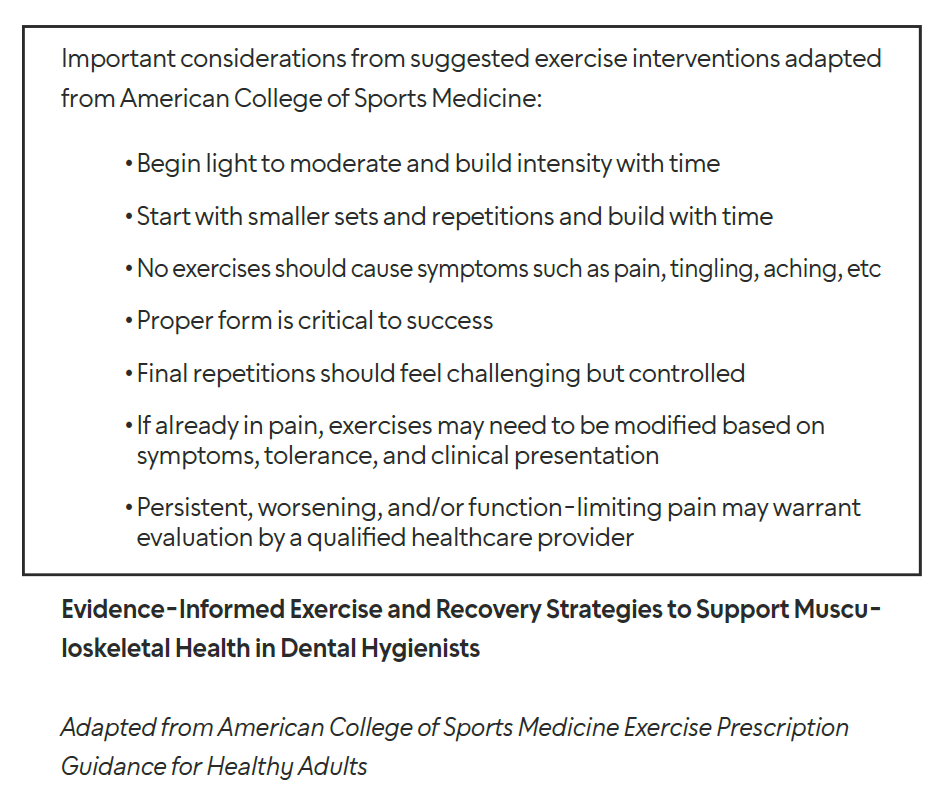
Exercise is a meaningful strategy for preventing occupational MSDs and reducing existing pain.16-25 Dental hygienists should focus on strategies that increase capacity, endurance, and tolerance. While operatory adjustments, positioning, and ergonomic equipment remain essential, exercise may help address some of the cumulative biomechanical strain associated with clinical practice.17
Stretching programs, resistance training, aerobic exercise, and other methods of physical activity reduce the risk of MSDs and related pain, decrease the need for pain medications, and improve productivity by reducing absences and work schedule modifications.16,18,19,21,22 Resistance training may improve physical capacity and muscular endurance while stretching may reduce stiffness and discomfort related to symptoms. Aerobic activity and yoga may provide broader benefits for functional capacity, stress management, fatigue, and overall well-being. Dumbbell strengthening, yoga, chairside or post-appointment stretching, guided post-workday exercise sessions, and aerobic activities have shown promising results in MSD pain reduction.16-20,23 Although all included studies involved participants with existing MSD pain, exercise programs may also help prevent MSD development.
Prevention should occur as early as possible in the career of a dental hygienist, ideally while enrolled in a dental hygiene education program.18,19 Preventive exercise routines should be viewed as part of a professional responsibility, investment in career longevity, and a recommended wellness activity for all dental hygienists.17-20,24 MSDs and pain negatively impact the overall practice as well by increased absenteeism, decreased clinical productivity and performance, reduced job satisfaction, decreased clinical hours, and modified work schedules.1-13,26 Therefore, strategies that support musculoskeletal health and reduce pain may significantly impact both the clinician and practice.
![]() Conclusion
Conclusion
Future research should focus on developing and validating dental hygiene-specific preventive exercise and recovery protocols for MSDs. In particular, studies are needed to determine the optimal exercise frequency, intensity, duration, progression, and delivery methods best for dental hygienists. Research should also examine long-term adherence, feasibility within clinical schedules, the comparative effectiveness of different exercise approaches, and when prevention programs are best introduced. Prospective studies are especially needed to determine whether exercise can prevent MSDs before symptoms develop. Ultimately, exercise is understood as a practical, low-risk, and evidence-informed strategy that complements adjunctive ergonomic equipment and positioning in reducing MSD pain.
References
- Lietz J, Kozak A, Nienhaus A. Prevalence and occupational risk factors of musculoskeletal diseases and pain among dental professionals in Western countries: A systematic literature review and meta-analysis. PloS One. 2018;13:e0208628.
- Saccucci M, Zumbo G, Mercuri P, et al. Musculoskeletal disorders related to dental hygienist profession. Int J Dent Hyg. 2022;20:571-579.
- Vidal, HF, Soriano EP, Caldas AF, et al. Cumulative trauma disorders among dentists. J Musculoskelet Pain. 2014;22:193-198.
- Pejcic N, Duric-Jovicic M, Milijkovic N, Popovi, DB, Petrovic V. Posture in dentists: Sitting vs. standing positions during dentistry work – an EMG study. Srpski Arhiv Za Celokupno Lekarstvo. 2016;144:181-187.
- Howarth SJ, Grondin DE, La Delfa NJ, Cox J, Potvin JR. Working position influences the biomechanical demands on the lower back during dental hygiene. Ergonomics. 2016;59:545-555.
- Dong H, Loomer P, Barr A, et al. The effect of tool handle shape on hand muscle load and pinch force in a simulated dental scaling task. Appl Ergon. 2007;38:525-531.
- Dong H, Barr A, Loomer P, et al. The effects of periodontal instrument handle design on hand muscle load and pinch force. J Am Dent Assoc. 2006;137:1123-1130.
- Dong H, Loomer P, Villanueva A, Rempel D. Pinch forces and instrument tip forces during periodontal scaling. J Periodontol. 2007;78:97-103.
- Villanueva A, Dong H, Rempel D. A biomechanical analysis of applied pinch force during periodontal scaling. J Biomech. 2007;40:1910-1915.
- Suedbeck JR, Armitano-Lago C. The effects of the traditional scaling technique versus a modified scaling technique on muscle activity and pinch force generation: a pilot study. J Dent Hyg. 2021;95:6-13.
- Suedbeck J, Tolle SL, McCombs G, et al. Effects of instrument handle design on dental hygienists’ forearm muscle activity during scaling. J Dent Hyg. 2017;91:47-54.
- Suedbeck J, Russell D, Armitano-Lago C, Ludwig E. The effects of dental hygiene instrument handles on muscle activity production. Int J Dent Hyg. 2023;21:731-737.
- Cherniack M, Brammer AJ, Nilsson T, et al. Nerve conduction and sensorineural function in dental hygienists using high frequency ultrasound handpieces. Am J Ind Med. 2006;49:313-326.
- Karsh BT. Theories of work-related musculoskeletal disorders: Implications for ergonomic interventions. Theor Issues Ergon Sci. 2006;7:71-88.
- Kumar S. Theories of musculoskeletal injury causation. Ergonomics. 2001;44:17-47.
- Hayes M. The effect of stainless steel and silicone instruments on hand comfort and strength: a pilot study. J Dent Hyg. 2017;91:40-44.
- Van Eerd D, Munhall C, Irvin E, et al. Effectiveness of workplace interventions in the prevention of upper extremity musculoskeletal disorders and symptoms: an update of the evidence. Occup Environ Med. 2016;73:62-70.
- Kim ES, Jo ED, Han GS. Effects of stretching intervention on musculoskeletal pain in dental professionals. J Occup Health. 2023;65:e12413.
- Roll SC, Tung KD, Chang H, et al. Prevention and rehabilitation of musculoskeletal disorders in oral health care professionals: A systematic review. J Am Dent Assoc. 2019;150:489-502.
- Shirzaei M, Mirzaei R, Khaje-Alizade A, Mohammadi M. Evaluation of ergonomic factors and postures that cause muscle pains in dentistry students’ bodies. J Clin Exp Dent. 2015;7:e414-418.
- Nye WH, Partido BB, DeWitt J, Kearney RC. Prevention and reduction of musculoskeletal pain through chair-side stretching among dental hygiene students. J Dent Hyg. 2021;95:84-91.
- Takeuchi K, Nakamura M, Fukaya T, Nakao G, Mizuno T. Stretching intervention can prevent muscle injuries: a systematic review and meta-analysis. Sport Sciences for Health. 2024;20(4):1119-1129.
- Ludwig E, Tolle SL. Ensure proper fit. Dimensions of Dental Hygiene. 2017;15(4):24-26.
- Tauqeer S, Arooj A, Shakeel H. Effects of manual therapy in addition to stretching and strengthening exercises to improve scapular range of motion, functional capacity and pain in patients with shoulder impingement syndrome: a randomized controlled trial. BMC Musculoskelet Disord. 2024;25:192.
- Speicher TE, Selkow NM, Warren AJ. Manual therapy improves immediate blood flow and tissue fiber alignment of the forearm extensors. Journal of Physical Medicine and Rehabilitation. 2022;4(2):28-36.
- Occupational Safety and Health Administration. Ergonomics. Available at osha.gov/ergonomics. Accessed June 10, 2026.
From Dimensions of Dental Hygiene. July/August 2026; 24(4):24-26

{kind=link}