
Preventing Harm in Dentistry
Underreported adverse events and preventable errors highlight an urgent need for stronger safety systems, ethical practice, and consistent prevention strategies.
This course was published in the May/June 2026 issue and expires June 2029. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 159
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the ethical and legal principles guiding dental practice.
- Define and discuss adverse events that may occur in dentistry.
- Identify strategies to reduce patient harm.
As dental procedures become more sophisticated, potential risks to patients also increase. Adverse events are unintended or harmful incidents that occur during the delivery of dental care, resulting in patient harm or injury. They are the result of medical errors, system failures, or a combination of factors and may cause injury, disability, or even death. Many of these errors occur with regularity in the dental setting, making prevention a priority.
Ethics and Jurisprudence
Healthcare professionals demonstrate their commitment to patient safety by adhering to ethical values that promote the highest level of practice, including:1-3 nonmaleficence: do no harm; beneficence: doing good and acting in the best interest of others; justice: treating people with fairness and impartiality; veracity: being truthful; autonomy: respecting individuals’ rights to make their own decisions without coercion; confidentiality: keeping each patient’s information private; and trust: acting with integrity to engender trust among patients.
The United States lacks standardized reporting systems and comprehensive data collection in dental settings.4 The National Practitioner Data Bank reported that 8,280 adverse reports involving dental hygienists and 34,327 involving dentists were filed between 2000 and 2025.5
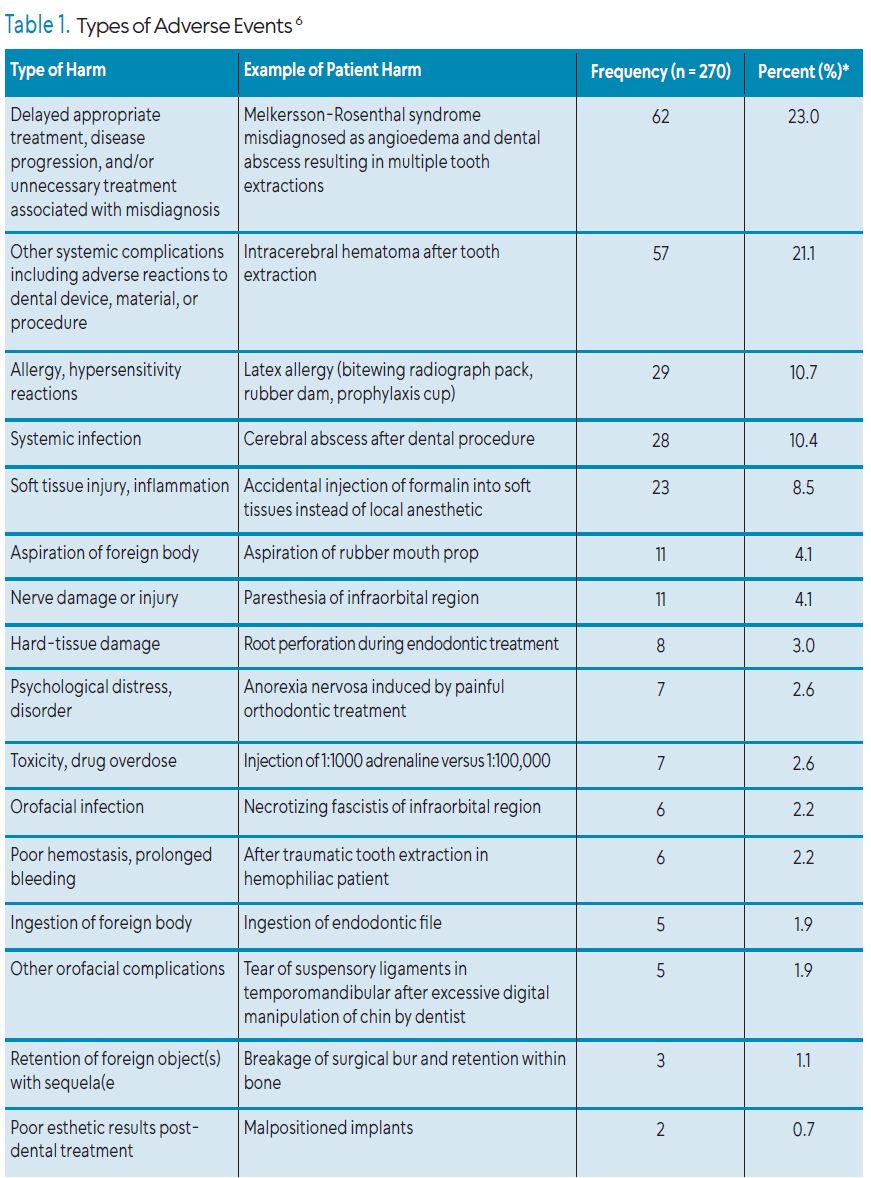
Many types of adverse events may occur in the dental office (Table 1). Obadan et al6 highlight the difficulty of categorizing adverse events, noting that the lack of a standardized dental patient safety taxonomy and wide variation in published case reports make classification challenging. Some of the most cited adverse events are medical errors, which include prescription errors, failure to properly maintain patient records, diagnostic errors, misdiagnosis and failure to refer.7 These often stem from negligence or failure to adhere to the standard of care.
Both civil and criminal offenses are perpetrated in the practice of dentistry. Contract law and tort law are two types of civil offenses. Contracts are legally binding agreements to keep a promise in exchange for something of value. The contract binds both parties to fulfill their committed responsibilities. Torts are civil wrongs resulting from the breach of legal duty. Negligence is an unintentional tort that involves the failure to act as a reasonable, prudent person would under similar circumstances. Dental malpractice is a form of professional negligence by an oral health professional that results in injury, harm, or damage to a patient.
Diagnostic Errors
The National Academy of Medicine defines a diagnostic error as a failure to establish an accurate and timely understanding of a patient’s condition or to effectively communicate that information. More broadly, it encompasses mistakes in the diagnostic process that result in missed, delayed, or incorrect diagnoses.9
Diagnosis-related issues were the leading cause of serious adverse events in dentistry, accounting for 23% of all reported incidents in a review of 270 US case reports.6 The researchers further categorized the extent of harm, reporting that 24% of patients experienced temporary harm significant enough to require a transfer to the emergency department or hospitalization and 24% experienced permanent harm.6
A 2025 study found the most common type of diagnostic dental practice malpractice claims was missed diagnoses (78.6%), followed by delayed diagnoses (13.4%), and wrong diagnoses (8.0%).9 In the review of 58,229 paid dental claims, missed diagnoses (78.6%) were the most common.9 A recent study used a sophisticated record review instrument that uses a list of triggers to alert reviewers to the potential presence of a wrong diagnosis and found that periodontal diseases were misclassified in one third of patients.10
The failure to diagnose or delayed diagnosis of oral cancer is a documented issue in US dental practices. Close to 58,500 Americans each year are diagnosed with oral or oropharyngeal cancer, causing 12,250 deaths.11 This high rate is, in part, due to the late diagnosis of lesions, which are then in advanced stages with poor prognoses.
A definitive diagnosis of oral cancer can only be made via biopsy, which few general dentists perform.12 Clinicians and patients should be aware of the most significant risk factors for oral cancer, including alcohol and tobacco use and sun exposure. A recent study evaluated 65 lawsuits regarding oral cavity cancer malpractice from 2000 to 2019. A total of 17 cases had a dentist defendant but no information on the exact judgments was provided.13 Still, Epstein et al14 emphasize the serious medicolegal consequences associated with delayed or incorrect diagnoses, noting that oral health professionals may face litigation when oral cancer is not identified, often due to routine oral examinations being omitted or performed inadequately.
Medication Errors
A medication error refers to any preventable incident that can lead to or result in inappropriate medication use or patient harm while the medication is under the control of a healthcare professional, patient, or consumer.15 Globally, dentists represent the second largest group of prescribers, including antibiotics, analgesics, anesthetics, anti-inflammatories, and high-fluoride content toothpastes, and antiseptics such as chlorhexidine.15 It is difficult to quantify the harm resulting from medication errors, especially since research consistently reports widespread misuse of these drugs.16
Errors associated with anesthetic delivery include administering too much or too little, not waiting long enough for the anesthetic effect to begin, administering an anesthetic known to cause nerve toxicity, accidental intravascular injection, improper needle placement, needle penetration into the orbit, and needle or cartridge breakage.17
Informed Consent
Oral health professionals must obtain valid consent before starting any treatment. The concept of informed consent is based on the ethical principle of autonomy, which asserts the right of a competent individual to self-determination. A competent person has the right to consent to or refuse any course of treatment. Consent can be given only after a patient has been fully advised of:
- Diagnosis (or suspected diagnosis)
- Nature and purpose of the proposed treatment or procedure; a concise description of what is to be done
- Risks and benefits of the proposed treatment (including common and serious/rare but significant risks)
- Prognosis if the treatment is successful or if it fails
- All alternatives, including the option of no treatment, and the risks and benefits of the alternatives.
Informed consent (Table 2) is generally categorized into three main types, distinguished by the level of formality and documentation required.18
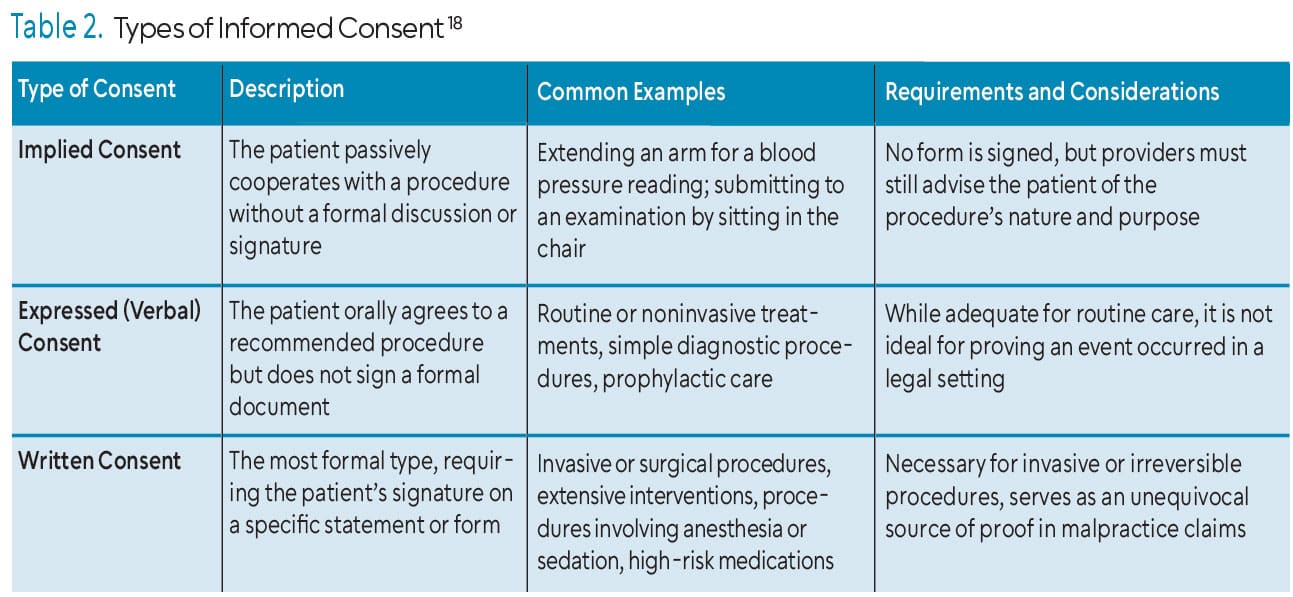
Informed consent forms should be used for all procedures and should be specific to the procedure, especially if the practice frequently performs complex procedures. The patient must always sign the consent form before treatment is provided.19
The legal definition and application of consent to treatment are facing increased scrutiny. Failure to obtain valid informed consent can lead to two types of legal claims: negligence and battery. Failing to disclose any risk that ultimately occurs is a breach of the standard of care and is considered negligence. Performing a procedure without consent constitutes battery. Consequently, any healthcare provider who fails to adequately prove that a patient has given valid, proper consent for a procedure is significantly increasing his or her vulnerability to litigation and malpractice lawsuits.
Documentation and Dental Patient Records
Maintaining secure, detailed, and accurate records is an ethical and legal obligation of all oral health professionals. The dental record is a legal document that includes patient’s assessment findings, treatment rendered, outcomes, and notations regarding communications between the patient and office staff.20 Oral health professionals provide the treatment, including dentists, dental hygienists, dental therapists, and dental assistants; however, a nonprovider may also enter information in the dental record. Patients also have responsibilities to their providers. Noting “no show,” “canceled”, or “came late ” is important to indicate patients’ noncooperation as well as patients’ failure to perform self-care or follow referrals as noted in an informed refusal. This will help show contributory negligence.
The dental record clearly states what work was previously completed on the patient and plays a critical role in the event of a malpractice insurance claim. Often, the dental record has absolved providers of responsibility in court cases. While written consent is not always necessary, it is an unequivocal source of proof of an event. Relying on verbal consent is not ideal in proving (or disproving) an event occurred. Dental records are also important when submitting dental benefit claims and help providers monitor progress of treatment.
There is no mandatory way to maintain a dental record. Providers record treatment using whatever format they choose. For example, providers choose different abbreviations for treatment. One dentist may choose to write the word lidocaine while another may choose to use the common abbreviation “lido.”Additionally, most offices now have electronic health records with custom-made templates that allow for ease in completing progress notes.
State laws and participating provider contracts generally specify the time following the last patient visit during which records must be maintained. Different requirements typically exist for the retention of children’s records.
The Privacy Rule and the Security Rule of the Health Insurance Portability and Accountability Act (HIPAA) also affect recordkeeping requirements. While there is no stipulation as to how long patient medical records must be kept (this is usually determined by state law), it does require that certain HIPAA compliance documents must be retained for at least 6 years from their date of creation or the date they were last in effect. The dental office should have a records retention policy and all staff should understand it. Poor documentation and record-keeping errors are a major contributing factor in dental malpractice lawsuits.
Patient Safety Initiatives
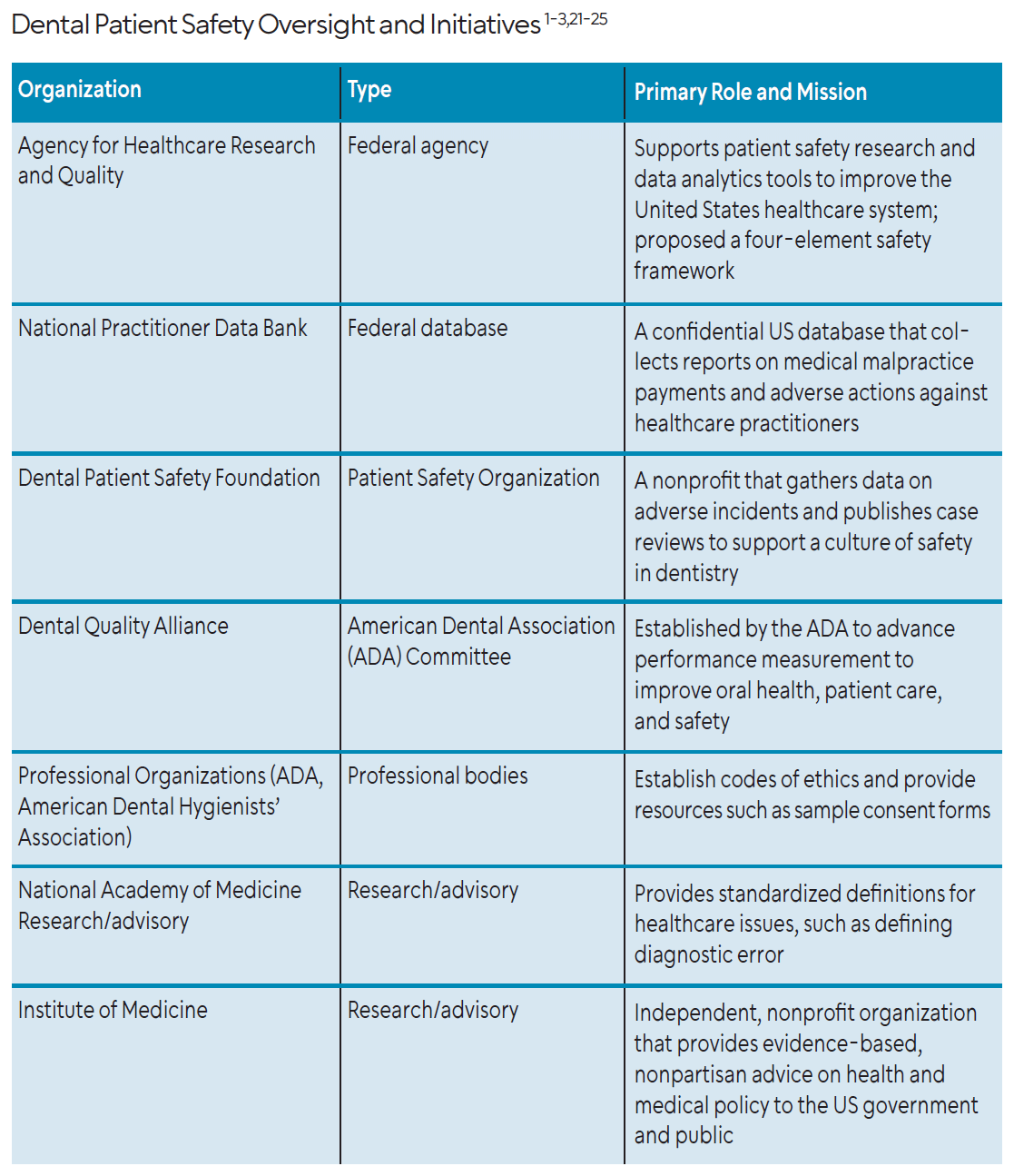
Evident from the lack of literature related to dental patient safety, standardized safety conventions and initiatives in dentistry are slowly starting to materialize. In 1999, Congress created the Agency for Healthcare Research and Quality (AHRQ) to support patient safety research and state-of-the-art data analytics tools to analyze and improve the US healthcare system.20 The organization has proposed a four-element patient safety framework to reduce treatment-related harm:21
- Identifying patient safety threats through rigorous chart reviews and assessing organizational patient safety cultures using the Medical Office Survey on Patient Safety Culture. This has been adapted for use in dentistry, in dental schools, specifically. It requires considerable resources.
- Identifying and evaluating effective patient safety practices using root-cause analysis and health are failure mode and effect analysis.
- Disseminating and implementing best practices while enlisting the help of organizations and stakeholders.
- Monitoring threats to patient safety to encourage a positive safety culture.
In 2005, AHRQ was further empowered, through the Patient Safety and Quality Improvement Act, to create and maintain a Network of Patient Safety Databases, which provides interactive, evidence-based management resources for healthcare providers, patient safety organizations (PSOs) listed by AHRQ, and others.22 The Dental Patient Safety Foundation gathers data on adverse incidents, publishes case reviews, and provides real-time data.23 Additionally, the American Dental Association established the Dental Quality Alliance to promote safety.24
A single provider can do a lot to ensure patient safety, such as creating a safety culture that includes infection prevention and control, ensuring medical histories are thoroughly reviewed, use of safety checklists, maintaining clear, accurate records to ensure continuity of care and prevent miscommunication, obtaining informed consent, and participating in continuing dental education.
![]() Conclusion
Conclusion
The underreporting of adverse events coupled with the lack of scientific research creates an imperative to enhance patient safety. Ethical principles along with informed consent and meticulous recordkeeping form the foundation from which all oral health professionals practice. The lack of a standardized reporting system and patient safety taxonomy continues to put patient safety at risk. Ultimately, reducing patient harm requires a conscious, daily commitment from every oral health professional.
References
- American Dental Association. Principles of Ethics and Code of Professional Conduct. Available at ada.org/about/principles/code-of-ethics. Accessed April 14, 2026.
- American Dental Hygienists’ Association (ADHA). ADHA Code of Ethics. Available at adha.org/about-adha/policies-bylaws/. Accessed April 14, 2026.
- American Dental Assisting Association (ADAA). ADAA Principles of Professional Ethics. Available at https://adaausa.org/about/about-adaa/. Accessed April 14, 2026.
- Kalenderian E, Obadan-Udoh E, Maramaldi P, et al. Classifying adverse events in the dental office. J Patient Saf. 2021;17:e540-e556.
- Division of Practitioner Data Bank. Data Analysis Tool. Available at npdb.hrsa.gov/analysistool. Accessed April 14, 2026.
- Obadan EM, Ramoni RB, Kalenderian E. Lessons learned from dental patient safety case reports. J Am Dent Assoc. 2015;146:318-326.
- Grober ED, Bohnen JM. Defining medical error. Can J Surg. 2005;48:39-44.
- Obadan-Udoh E, Howard R, Valmadrid LC, Walji M, Mertz E. Patients’ experiences of dental diagnostic failures: a qualitative study using social media. J Patient Saf. 2024;20:177-185.
- Singhania R, Obadan-Udoh E. Dental diagnostic errors and characteristics associated with claims in the United States, 1990-2020. J Am Dent Assoc. 2025;156:563-570.
- Tokede B, Yansane A, Brandon R, et al. The burden of diagnostic error in dentistry: a study on periodontal disease misclassification. J Dent. 2024;148:105221.
- Oral Cancer Foundation. Oral Cancer Facts. Available at https://oralcancerfoundation.org/facts/. Accessed April 14, 2026.
- González-Moles MÁ, Aguilar-Ruiz M, Ramos-García P. Challenges in the early diagnosis of oral cancer, evidence gaps and strategies for improvement: a scoping review of systematic reviews. Cancers. 2022;14:4967.
- Wong A, Zhu D, Tong JY, et al. The jaw-dropping costs of oral cavity cancer malpractice. Head Neck. 2021;43:2869-2875.
- Epstein JB, Sciubba JJ, Banasek TE, Hay LJ. Failure to diagnose and delayed diagnosis of cancer: medicolegal issues. J Am Dent Assoc. 2009;140(12):1494-1503.
- Eriksen N, Kleva S, Shpati D, Xhizdari R. Medical errors in dentistry, improving by knowing and accepting the reality. Eur J Med Nat Sci. 2024;7.
- Lockhart PB, Thornhill MH, Zhao J, et al. Factors that affect dentists’ use of antibiotic prophylaxis: findings from the National Dental Practice-Based Research Network questionnaire. J Am Dent Assoc. 2022;153(6):552-562.
- Nagelberg R. Medical errors in dentistry. RDH. 2015;35:79-85.
- Kakar H, Gambhir RS, Singh S, Kaur A, Nanda T. Informed consent: corner stone in ethical medical and dental practice. J Family Med Prim Care. 2014;3:68-71.
- American Dental Association. Types of Consent. Available at ada.org/resources/practice/practice-management/types-of-consent. Accessed April 14, 2026.
- Agency for Healthcare Research and Quality. AHRQ: A Brief History. Available at ahrq.gov/cpi/about/brief-history.html. Accessed April 14, 2026.
- Yansane A, Walji MF, Kalenderian E. Introducing safety in dentistry: perspectives and directions. J Calif Dent Assoc. 2019;47:433-437.
- Agency for Healthcare Research and Quality. What is the Network of Patient Safety Databases? Availabel at ahrq.gov/npsd/what-is-npsd/index.html. Accessed April 14, 2026.
- Dental Patient Safety Foundation. Enhance Our Culture of Safety. Available at dentalpatientsafety.org/. Accessed April 14, 2026.
- American Dental Association. Dental Quality Alliance. Available at ada.org/resources/research/dental-quality-alliance. Accessed April 14, 2026.
From Dimensions of Dental Hygiene. May/June 2026; 24(3):28-31

{kind=link}