Role of Lasers in Modern Periodontal Therapy
From bacterial reduction to tissue regeneration, lasers may provide a complementary adjunct to traditional treatments.
This course was published in the March/April 2026 issue and expires April 2029. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 135
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify risk factors for periodontal diseases.
- List the types of lasers used in periodontal treatments.
- Discuss the benefits of laser therapy used in periodontal treatments.
Periodontal diseases are the most common cause of tooth loss in the modern world. According to data from the World Health Organization, gingival bleeding and calculus are most prevalent among adults from all regions of the world, while advanced disease with deep periodontal pockets (≥ 6 mm) affects approximately 10% to 15% of the adult population.1
Periodontitis encompasses a multifaceted interaction between specific bacteria and host factors that results in loss of periodontal attachment structures. The current understanding of periodontitis’ etiopathogenesis describes periodontal diseases as site-specific conditions driven by pathogenic host–microbial interactions that trigger the overproduction of destructive enzymes and pro-inflammatory mediators, ultimately determining the extent and severity of tissue destruction.2,3 This pattern has assisted oral health professionals to better comprehend the underlying host immune responses and the expansion of innovative treatment strategies that may improve therapeutic outcomes and overall clinical management of patients with periodontitis.
The main goal in treating periodontitis is reducing attached and unattached pathogenic bacteria. Attached biofilm is composed of embedded bacteria in a protective extracellular matrix that protects the pathogenic bacteria from the host’s immune response and antimicrobial agents. Pathogenic bacteria include enzymes and lipopolysaccharides that trigger the inflammatory response and tissue destruction. Unattached pathogenic bacteria can detach from the biofilm and enter the bloodstream during the host’s inflammatory response. Consequently, the unattached bacteria have the ability to colonize in different sites in the oral cavity or reattach to tooth surfaces and restorations, initiating new biofilm formation and propagating the disease cycle.
Periodontitis treatment focuses primarily on the reduction of pathogenic bacteria in biofilm. Nonsurgical periodontal therapy (NSPT) reduces periodontal pocket depth and clinical attachment levels in mild to moderate periodontitis cases in which pocket depths are < 6 mm.4 In the treatment of probing depths > 6 mm, surgical periodontal therapy results in greater periodontal pocket depth reduction and clinical attachment gain.4
Chronic periodontal diseases can be arrested and successfully treated by NSPT provided adequate plaque control is maintained throughout the supportive phase of treatment.5 Providing NSPT includes mechanical and chemotherapeutic procedures to minimize or eliminate pathogenic bacteria in the periodontal tissues and alter host immune inflammatory responses. Mechanical therapy refers to both supragingival and subgingival scaling and debridement of the root surfaces by hand or power instrumentation to remove deposits such as plaque, calculus, endotoxins, and other plaque-retentive local factors.6
Chemotherapeutic agents include antimicrobial therapies that can be used systemically or locally to address changes in the microflora. Host modulatory therapy can be implemented to manage altered host immune response consisting of excessive levels of pro-inflammatory enzymes, cytokines, and excessive osteoclast function that may be related to certain risk factors.7
Periodontal diseases are multifactorial, and one or more risk factors are required for disease initiation and progression.1 Poor oral hygiene, poorly controlled systemic diseases, stress, smoking, genetic susceptibility, and alveolar bone loss are just some of the risk factors that may influence long-term outcomes of periodontal therapy.1,8
Smoking
Research studies support the correlation between smoking and periodontal diseases. Tobacco smoking destroys periodontal tissues and increases the rate of periodontal disease progression.9 Smoking tobacco modifies the host response to the pathogenic bacteria in biofilm. Patients with periodontal diseases who smoke present with diminished clinical gingival inflammation and bleeding compared to patients who do not smoke. Patients need to know that nicotine exerts local vasoconstriction, reducing blood flow and causing edema and clinical signs of inflammation.10
Smoking tobacco impairs the healing process especially in the gingival tissues and supporting periodontal structures. Smoking reduces blood flow to the gingival tissues, delaying the body’s normal healing processes. Subsequently, smoking weakens the immune system, making it less effective in resisting the pathogenic bacteria that cause periodontal diseases. Smoking also causes hyposalivation, and alters the composition of saliva, decreasing antimicrobial properties and increasing pathogenic bacteria.11 The combined effects of hyposalivation, altered salivary composition, and increased bacterial growth can lead to a higher risk of dental diseases including caries, gingivitis, and periodontitis.11
Diabetes Mellitus
Diabetes has been unequivocally confirmed as a major risk factor for periodontitis.12 The risk of periodontitis is increased by approximately threefold in patients with diabetes compared to those without.13 Diabetes can exacerbate the severity and accelerate the progression of periodontal diseases. Altered wound healing is a common problem among individuals with diabetes. The primary reparative cell in the periodontium (fibroblast) does not function properly in high-glucose environments.14 Furthermore, the collagen that is produced by fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes, the production of which is elevated in diabetes.15 Consequently, periodontal wound healing responses to chronic microbial insult may be altered among those with sustained hyperglycemia, resulting in increased bone loss and attachment loss.16
Cardiovascular Disease
A correlation between oral health and cardiovascular disease has been proposed for more than a century. Oral sepsis and dental extractions were suggested as causes of cardiac tissue infection.17 Periodontal diseases generate an inflammatory host response that may support the development and progression of cardiovascular diseases.
Research suggests that patients with periodontal diseases may face an increased risk of cardiovascular disease, with greater periodontal severity potentially associated with higher cardiovascular risk.18 Epidemiologic research has substantiated the link between periodontal diseases and cardiovascular diseases.19 Although research continues to point to a connection, causality has not yet been established. Shetty et al19 report an improvement in cardiovascular diseases risk factors after periodontal interventions.
Lasers in Periodontal Treatment
Traditional management of periodontal diseases involves mechanical debridement, oral hygiene education, and, in some cases, adjunctive antibiotic therapy.20,21 While these methods are effective in managing mild to moderate cases, they have limitations. Deep periodontal pockets (> 6 mm) can be challenging to scale thoroughly with mechanical methods and systemic conditions may impair wound healing and response to treatment.22
Recent advancements in light amplification by stimulated emission of radiation (laser) technology have introduced new paradigms in periodontal therapy.23 Lasers create a narrow beam of light in a specific wavelength that produces concentrated energy at a exact location. Research studies revealed developments in laser technology for use in periodontal treatments known as laser periodontal therapy.22
Laser Safety
Most lasers used in dentistry are user friendly, however, precautions must be followed to ensure safe and effective operation. Lasers used in dentistry require proper training and education. Training and requirements for dental hygiene laser use vary by state. Oral health professionals must keep apprised of state regulations to determine whether laser use is permitted within their scope of practice.
Wavelength protective eyewear must be worn by anyone in the vicinity of the laser while in use.24 The meaning of a safe distance is not standardized as a variety of laser types are used in dentistry. As such, every office should have a designated laser safety officer (LSO) to supervise the proper use of the laser, coordinate staff training, oversee the use of protective eyewear, and remain up to date with pertinent regulations.24 The LSO will determine the nominal hazard zone, which depends on the type of laser used. The Occupational Safety and Health Administration (OSHA) requires the display of appropriate signage in each room in which a laser is used.25 The use of lasers during any dental treatment must be documented in the patient chart.
Clinical Applications of Lasers in Periodontal Treatment
Laser therapy in periodontal treatment uses either soft-tissue or hard-tissue lasers. The choice between these modalities depends on the target tissue and the wavelength of the laser used. The most common dental lasers are carbon dioxide (CO2) lasers (water and hydroxyapatite); erbium lasers (water and hydroxyapatite); neodymium-doped yttrium aluminum garnet (Nd:YAG) lasers (melanin, hemoglobin and pigmentation); and diode lasers (melanin, hemoglobin, and pigmentation).
The effects of laser energy are wide ranging. Lasers exhibit potential in wound healing, tissue ablation, bacterial reduction, epithelial ablation, connective tissue remodeling, enhanced bone metabolism, hemorrhage control, and enhanced root preparation.25 When choosing the appropriate laser for periodontal treatment, the wavelength, target tissue, type of power, pulsing mode, cooling mechanism, delivery system, quality, and, most important, the training required to safely operate the device are all factors to consider.25
Laser therapy can control bacteremia, remove pocket epithelium, reduce bacteria, and improve periodontal regeneration in animals and humans without damaging the surrounding bone and pulp tissues.26 Erbium lasers demonstrate significant bactericidal effect against Porphyromonas gingivalis and Actinobacillus actinomycetemcomitans.27 Reduction of interleukins and pocket depth have also been reported.27
Soft tissue diode lasers may support new cementum-mediated connective tissue attachment and periodontal regeneration of diseased root surfaces.27 Diode lasers target pigmentation and melanin, use low power, and can be used to excise tissue, kill bacteria at shallow depths, and provide low-level laser therapy.25
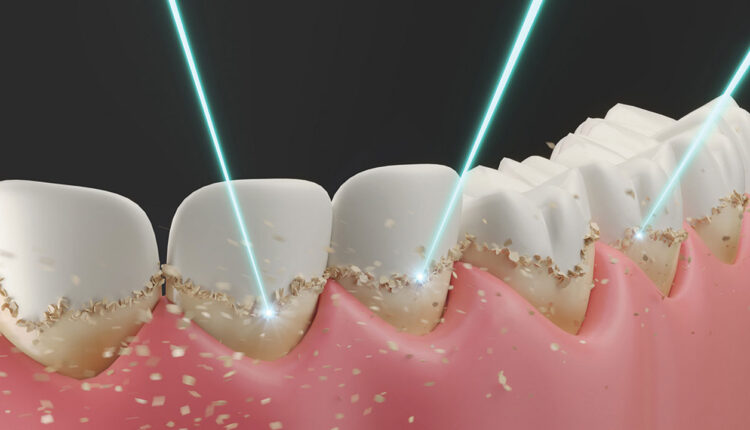
Laser bacterial reduction (LBR), a noninvasive procedure, uses a noncutting laser to eliminate bacteria in periodontal pockets as an adjunctive therapy during scaling and root planing or prophylaxis. During LBR, a soft tissue laser is inserted into the periodontal pocket, providing a small amount of thermal energy that decontaminates and eradicates the bacteria in the periodontal pocket. The laser is applied for a short duration, usually 5 to 10 seconds per area, and is moved continuously with apical to coronal strokes to ensure complete decontamination of the periodontal pocket has been completed. LBR likely provides some antimicrobial benefit, but the magnitude of that benefit varies depending on the laser type, clinical protocol, and patient condition. As a result, many researchers conclude that lasers may enhance periodontal treatment when used appropriately, but stronger clinical evidence is still needed to establish consistent, long-term advantages over conventional care.28
Laser-assisted new attachment procedure (LANAP) employs a laser beam for the breakdown of pathogenic bacteria and elimination of damaged periodontal tissues.29 This is accomplished through the sterilization of the compromised areas, promoting tissue regeneration without surgery, regenerating the damaged periodontal tissues, and developing an attachment to the root surfaces of the newly formed connective tissues.28 LANAP may be associated with cementum-mediated tissue attachment and apparent periodontal regeneration of diseased root surfaces.27
LANAP also increases the release of endorphins, diminishes nerve sensitivity, and decreases the perception of pain by blocking pain signals transmitted from the inflamed area to the brain.27 Additionally, LANAP causes vasodilation, which clears inflammation and edema and promotes lymphatic drainages. Through vasodilation, wound healing is accelerated due to better blood flow through new formation of capillaries within the inflamed tissues.27
In LANAP, the laser targets diseased tissue as it presents with darker hues and laser wavelengths are highly absorbed by melanin and hemoglobin. The LANAP procedure usually requires two passes with the laser.27 The first pass of the laser eradicates pathogenic bacteria in the periodontal pocket, followed by ultrasonic and hand scaling to remove accretions on the root surfaces. A second pass with the laser will produce clotting in the periodontal pocket to seal the area, promoting tissue regeneration.27
Evidence shows LANAP works best as part of a comprehensive periodontal treatment plan, rather than as a standalone procedure. Additionally, while some case series and studies show tissue regeneration, results can vary depending on patient factors, operator experience, and disease severity.30
Developing a Periodontal Treatment Plan
After obtaining a thorough medical history, a comprehensive treatment plan is established. The periodontal charting and radiographs are reviewed in order to determine the periodontal stage and grade. The patient’s assessment is used to determine whether laser therapy is an appropriate option. If the patient presents with deep periodontal pockets and/or chronic inflammation, LBR or LANAP may be beneficial in the comprehensive periodontal treatment plan.
Once it has been determined that laser therapy will be incorporated into the comprehensive periodontal treatment plan, the patient must give informed consent. Informed consent includes explaining the assessment and proposed treatment, benefits and risks of the treatment, and alternative treatment options, including the consequences of not treating the periodontal condition. Treatment should not commence unless the patient has signed the proposed treatment plan.
The evaluation of laser therapy’s efficacy in periodontal treatment involves an assessment of clinical outcomes, comparisons with traditional treatments, and analysis of various studies and clinical trials.23 Laser therapy is not a substitute for traditional methods of periodontal treatment but may be a helpful adjunct. Its efficacy varies depending on the type of laser used, the severity of the periodontal disease, and individual patient factors.23 Mills et al30 report that current evidence is inadequate to conclude laser therapy alone is either superior or comparable to conventional periodontal therapy in terms of clinical improvement in probing depths in the treatment of moderate to severe periodontitis.
In dentistry, laser therapy has become more prevalent as an adjunctive method to periodontal treatment. Conventional scaling and root planing may not always allow thorough access to the periodontal pockets during treatment. Lasers may offer bactericidal and detoxification effects, as well as removal of the epithelium lining and granulation tissue.31 Lasers in the periodontal treatment plan focus on bactericidal and disinfection of periodontal pathogens while aiming to diminish the etiology of periodontal diseases.
References
- Bhansali RS. Non-surgical periodontal therapy: An update on current evidence. World Journal of Stomatology. 2014;3(4):38-51.
- Ryan ME, Preshaw PM. Host modulation. Carranza’s Clinical Periodontology. 11th ed. Philadelphia: Saunders; 2012:275-280.
- Kirkwood KL, Cirelli JA, Rogers JE, Giannobile WV. Novel host response therapeutic approaches to treat periodontal diseases. Periodontol 2000. 2007;43:294-315.
- Heitz-Mayfield LJ, Trombelli L, Heitz F, Needleman I, Moles D. A systematic review of the effect of surgical debridement vs non-surgical debridement for the treatment of chronic periodontitis. J Clin Periodontol. 2002;29 Suppl 3:92-102.
- Axelsson P, Lindhe J. Effect of controlled oral hygiene procedures on caries and periodontal disease in adults. Results after 6 years. J Clin Periodontol. 1981; 8:239-248.
- Drisko CH. Nonsurgical periodontal therapy. Periodontol 2000. 2001;25: 77-88.
- Ryan ME. Nonsurgical approaches for the treatment of periodontal diseases. Dent Clin North Am. 2005;49:611-36.
- Albandar JM. Epidemiology and risk factors of periodontal diseases. Dent Clin North Am. 2005;49:517-532.
- Zini A, Sgan-Cohen HD, Marcenes W. Socio-economic position, smoking, and plaque: a pathway to severe chronic periodontitis. J Clin Periodontol. 2011;38:229–235.
- Jensen JA, Goodson WH, Hopf HW, Hunt TK. Cigarette smoking decreases tissue oxygen. Arch Surg. 1991;126:1131–1134.
- Sever E, Božac E, Saltović E, Simonić-Kocijan S, Brumini M, Glažar I. Impact of the tobacco heating system and cigarette smoking on the oral cavity: a pilot study. Dent J (Basel). 2023;11:251.
- Khader YS, Dauod AS, El-Qaderi SS, Alkafajei A, Batayha WQ. Periodontal status of diabetics compared with nondiabetics: a meta-analysis. J Diabetes Complicat. 2006; 20:59–68.
- Mealey BL, Ocampo GL. Diabetes mellitus and periodontal disease. Periodontol 2000. 2007;44:127–153.
- Willershausen-Zönnchen B, Lemmen C, Hamm G. Influence of high glucose concentrations on glycosaminoglycan and collagen synthesis in cultured human gingival fibroblasts. J Clin Periodontol. 1991;18:190-195.
- Golub LM, Lee HM, Ryan, ME .Tetracyclines inhibit connective tissue breakdown by multiple non-antimicrobial mechanisms. Adv Dent Res. 1998;12:12-26.
- Mealey BL. Periodontal disease and diabetes: A two-way street. J Am Dent Assoc. 2006;137:S26-S31.
- Miller WD. The human mouth as a focus of infection. Dent Cosmos. 1891; 33: 689– 713.
- Alwithanani N. Periodontal diseases and heart diseases: a systemic review. J Pharm Bioallied Sci. 2023;15(Suppl 1): S72-S78.
- Shetty B, Fazal I, Khan SF, et al. Association between cardiovascular diseases and periodontal disease: more than what meets the eye. Drug Target Insights. 2023; 17:31-38.
- Batchelor P. Is periodontal disease a public health problem? Br Dent J. 2014;217:405-409.
- Ramesh T, Sundar M, Ranjani SS, Kurian B. Efficacy of scaling and root planing with and without adjunctive use of diode laser or tetracycline fibers in patients with generalized chronic periodontitis: a comparative study. J Investig Clin Dent. 2017;8: e12188.
- Kwon T, Lamster IB, Levin L. Current concepts in the management of periodontitis. Int Dent J. 2021;71:462-476.
- Al Asmari D, Alenezi A. Laser technology in periodontal treatment: benefits, risks, and future directions-a mini review. J Clin Med. 2025;14:1962.
- Verma SK, Maheshwari S, Singh RK, Chaudhari PK. Laser in dentistry: An innovative tool in modern dental practice. Natl J Maxillofac Surg. 2012;3:124-132.
- Linden E. Laser basics. Dimensions of Dental Hygiene. 2016;14(4):56–59.
- Romanos G. Current concepts in the use of lasers in periodontal and implant dentistry. J Indian Soc Periodontol. 2015;19:490-494.
- Elavarasu S, Naveen D, Thangavelu A. Lasers in periodontics. J Pharm Bioallied Sci. 2012;4 (Suppl 2): S260-263.
- Patel S, Awan KH, Freitas CMT, Bhandi S, Licari, FW, Patil S. Diode laser targeting red-complex bacteria in periodontitis: a systematic review. Eur Rev Med Pharmacol Sci. 2023;27:11806-11816.
- Bechir ES. The clinical and microbiological effects of LANAP compared to scaling and root planing alone in the management of periodontal conditions. Diagnostics (Basel). 2023;13:2450.
- Mills MP, Rosen PS, Chambrone L, et al. American Academy of Periodontology best evidence consensus statement on the efficacy of laser therapy used alone or as an adjunct to non-surgical and surgical treatment of periodontitis and peri-implant diseases. J Periodontol. 2018; 89: 737–742.
- Aoki A, Sasaki KM, Watanabe H, Ishikawa I. Lasers in nonsurgical periodontal therapy. Periodontol 2000. 2004;36:59-97.
From Dimensions of Dental Hygiene. March/April 2026;24(2):40-45
