
When Abuse Presents in the Dental Chair
Intimate partner violence often leaves its clearest signs on the head, neck, and mouth, making oral health professionals uniquely positioned to help patients experiencing abuse.
This course was published in the March/April 2026 issue and expires April 2029. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 156
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define intimate partner violence (IPV) and identify its clinical and behavioral signs.
- Establish a protocol for screening victims of IPV in the dental setting.
- Discuss the legal and ethical obligations of the dental team regarding IPV.
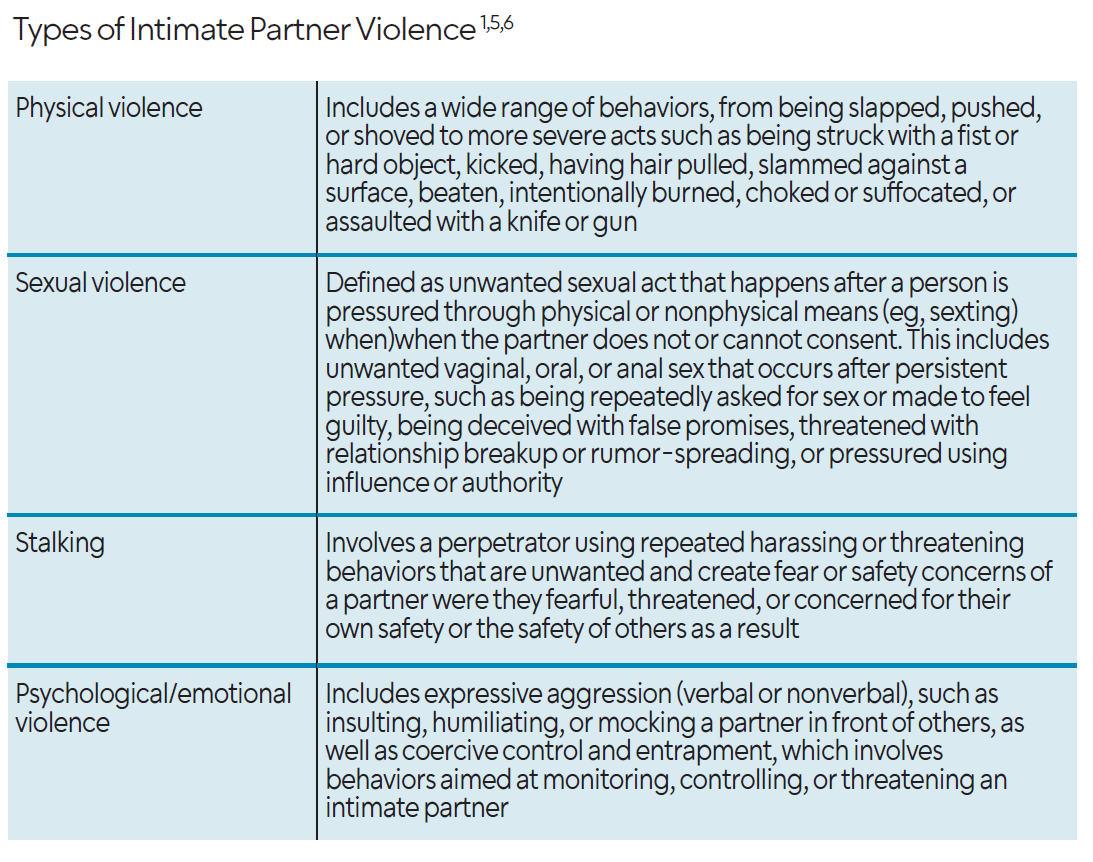
The United States Centers for Disease Control and Prevention (CDC) defines intimate partner violence (IPV) as abuse or aggression that occurs in a romantic relationship.1 IPV can occur within a current relationship or may be initiated and sustained by a former partner. It is also characterized by a partner attempting to exert power and control.
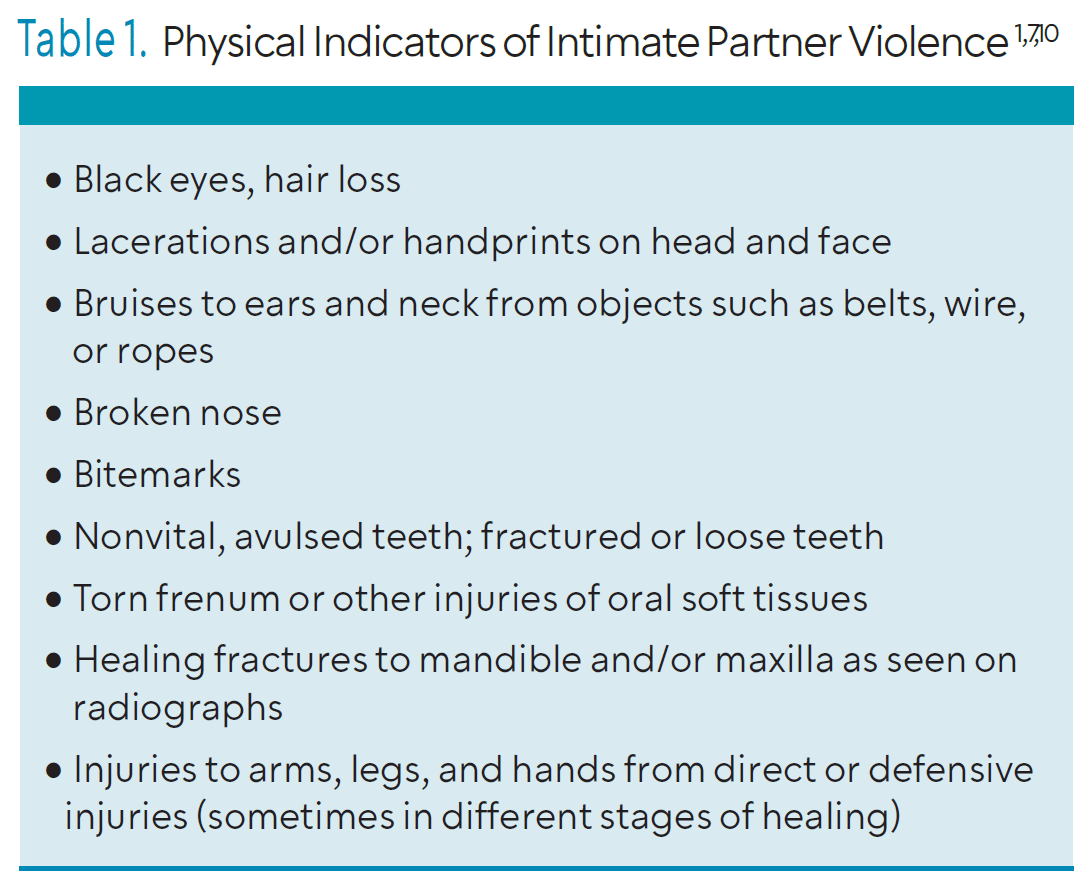
The link between IPV and oral health is well-documented, with those impacted often presenting with dental trauma, facial fractures, and bruising to the head and neck. Oral health professionals are in a key position to screen patients and document and support individuals affected by IPV. Studies have shown strong connections between types of abuse and oral health problems.2,3 For example, psychological abuse is linked to periodontal diseases, while physical violence often leads to broken teeth. Common dental injuries include fractures (59.1%), tooth displacements (27.2%), and tooth loss (13.7%), usually caused by direct blows without weapons.2,3,4 These injuries can be extremely painful, affect chewing and speaking, and lower self-esteem.
Abuse-related stress can also lead to grinding teeth, temporomandibular disorders, and chronic facial pain. Table 1 lists other common signs of abuse. Oral health professionals are in a unique position to detect these warning signs during routine visits by carefully examining the head, neck, and mouth.2
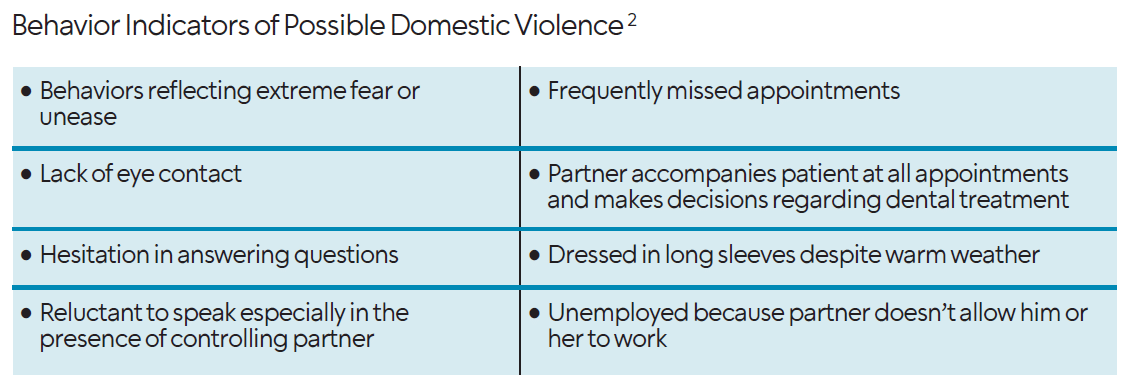
Beyond physical injuries, certain patient behaviors may also suggest abuse, such as missed appointments due to a controlling partner, reluctance to speak in front of a partner, or signs of dental neglect.2,5-9 Oral health professionals should be attuned to patients’ demeanor in the presence of their partners, which may provide important warning signs regarding IPV victimization.2
By remaining observant, empathetic, and supportive, oral health professionals can create a safe space where patients feel comfortable disclosing abuse and receiving the help and resources they need.2,5
Screening for Intimate Partner Violence
Although domestic violence significantly impacts oral health and oral health professionals play a vital role in recognizing signs of abuse, a troubling gap in screening knowledge remains.2 About 75% of physical abuse injuries occur on the head, face, mouth, and neck. Victims who are isolated from friends, family, and social services may seek dental care — either through scheduled visits or emergency appointments.6 Knowledge of IPV screening and how to appropriately respond enables oral health professionals to provide compassionate care, communicate with victims more confidently, and address their needs effectively.6
Dental practices must identify a screening tool that best fits their clinical setting. In 1992, the Massachusetts Medical Society developed the RADAR model, or Routinely screen, Ask direct questions, Document findings, Assess patient safety, and Review options and refer as appropriate, to physicians in responding to patients affected by IPV. Over time, this model has been adapted for use by other health professionals, including dentists and dental hygienists, to address IPV within the dental environment.7
The HITS tool, or Hurt, Insult, Threaten, and Scream, is a brief screening instrument used in healthcare settings to assess the risk of domestic violence or IPV. It consists of four questions, each asking how often a partner engages in these behaviors. Patients respond on a five-point Likert scale (1 = never to 5 = frequently). A higher total score indicates a greater likelihood of IPV.
Because it is short, easy to administer, and validated in multiple populations, the HITS tool is commonly used in medical and dental settings as part of IPV screening.8 As awareness of trauma’s impact grows, healthcare providers are recognizing the importance of trauma-informed care. This approach emphasizes understanding a patient’s life experiences to guide treatment and can enhance patient engagement, adherence, health outcomes, and the well-being of providers and staff.9
Developing trauma-informed care skills is essential for recognizing and responding to patients who may be experiencing violence. For survivors of sexual assault or IPV, the dental setting can be intimidating and may trigger distress linked to past abuse. Oral health professionals should remain mindful of these triggers and incorporate supportive techniques into daily practice.9
A widely recognized and effective trauma- informed approach for addressing such situations is the AVDR method, or Ask, Validate, Document, and Refer/Report. This framework helps guide oral health professionals in appropriately responding to family violence while ensuring that victims receive necessary support and providers fulfill their professional obligations.7,9,10
Before applying the AVDR method, however, oral health professionals should take foundational steps to prepare for these sensitive encounters. This includes building and maintaining a professional, therapeutic relationship with patients, recognizing the signs of IPV, and becoming familiar with their state’s specific reporting requirements for each type of abuse.9
The AVDR approach consists of the following steps:7,9,10
- Ask. Initiate a respectful and private conversation if abuse is suspected (eg, Do you feel safe at home?)
- Validate. Acknowledge the patient’s experience without judgment and express support, (eg, What you’re telling me makes me concerned for your well-being).
- Document. Record observations and patient statements accurately and objectively.
- Refer/Report. Provide appropriate resources or make a report as required by state law.
Reporting Intimate Partner Violence
In situations involving suspected domestic violence, oral health professionals have important legal and ethical responsibilities that must inform their actions and guide their decision-making.2,11,12 A key responsibility in cases of suspected IPV is understanding reporting laws, which can vary significantly by jurisdiction.
Although dental practitioners are generally bound by strict standards of patient confidentiality, laws may require them to report suspected abuse if there is a reasonable belief that the patient is in immediate danger. In such cases, the duty to protect the patient can override the standard confidentiality expectation.2
Oral health professionals must be familiar with the specific reporting requirements in their state or locality to ensure legal compliance. Beyond legal duties, they also face complex ethical considerations. Oral health professionals must carefully balance respecting a patient’s autonomy with the need to ensure his or her safety — an especially challenging task when patients are hesitant to disclose abuse or decline help due to fear, shame, or other personal barriers.2,11 Creating a supportive, nonjudgmental environment that encourages trust, highlights available resources, and emphasizes the importance of safety and support is the best approach.2
Documentation and Patient Confidentiality
Careful and accurate documentation is one of the most important steps after recognizing potential signs of IPV. Thorough documentation serves as a vital record for future reference, enabling healthcare providers to monitor the progression and severity of abuse over time. This ongoing record supports continual assessment of the patient’s condition and guides appropriate care and intervention strategies.2
Detailed documentation can also help identify patterns or trends in abusive behavior, offering insight into relationship dynamics and assisting in evaluating the patient’s level of risk. To enhance accuracy and accountability, asking a witness, such as a dental assistant or other office staff, to be present during the documentation process is recommended.2,10
In the dental record, providers should include clear, objective details about the injuries, noting the location, size, color, and any other observable characteristics. Supplementary documentation may include intraoral and extraoral photographs, as well as periapical and panoramic radiographs. Narrative notes must remain factual and unbiased, incorporating precise measurements of affected hard and soft tissues. Any verbal statements made by the patient concerning their injuries should be recorded word-for-word to preserve the integrity of his or her account.7,11
Best Practices
When IPV may be a concern, how an oral healthcare provider communicates with a patient can significantly influence his or her comfort, trust, and willingness to seek support or intervention. Conversations related to violence or trauma should always be approached using a trauma-Informed framework.
Trauma can affect both the brain and body in complex and far-reaching ways, influencing oral health, overall health, and patient behavior. When oral health professionals are not aware of how trauma may impact patients, opportunities may be missed to promote safety, connect patients to supportive resources, and prevent further harm. Additionally, communication that is not trauma-informed may unintentionally contribute to distress.13
Trauma-informed care aims to create safety for people by recognizing the effects of trauma and its close links to health and behavior. Unlike trauma-specific care, it does not focus on eliciting or treating trauma histories, but rather on fostering safe, respectful environments that minimize the potential for harm during healthcare interactions.13
Before engaging in conversations related to IPV, oral health professionals are encouraged to learn about how trauma and trauma-related symptoms may affect patients, to create a supportive, nonjudgmental clinical environment. Clinicians should also become familiar with local community resources related to IPV and establish relationships with community partners who can assist with referrals and staff training.14
When communicating with patients about sensitive topics such as violence, several factors should be considered, including the physical environment and approaches to screening and intervention. Screening should be conducted as confidentially as possible.13 This may involve using a private room, drawing a curtain, or checking in about safety and privacy if the patient is accompanied by another person.
Before beginning any screening or discussion related to personal experiences, clinicians should ask for the patient’s permission and clearly explain the purpose of the conversation. Oral health professionals should also address any questions about confidentiality and explain relevant policies or reporting requirements so patients can make informed decisions about what they choose to share.14
If a patient expresses interest in support or resources, clinicians should avoid directing or prescribing what the patient “should” do. Trauma-informed communication prioritizes patient autonomy and supports individuals in making their own informed choices. During dental procedures, clinicians should clearly explain each step, including what will happen, why it is necessary, and what areas of the face or mouth will be touched. Ongoing communication during procedures can help maintain a sense of control and safety.
When discussing available resources, oral health professionals should offer information about local support services and acknowledge the patient’s strength in engaging in conversation and seeking care.14
Resources for Suspected Victims
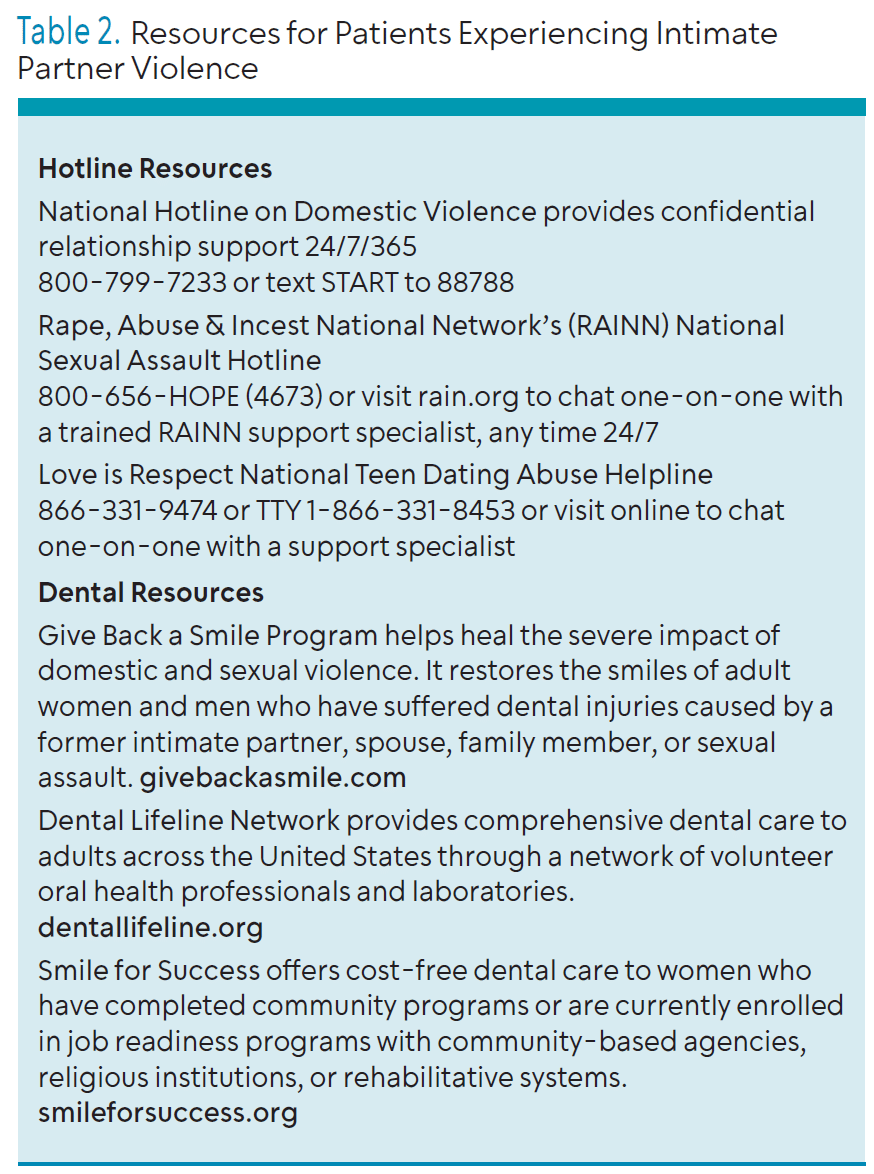
To support victims of IPV, dental office staff should collaborate with other healthcare professionals to compile and regularly update a comprehensive list of local resources. Once a patient discloses that he or she has been a victim, the healthcare professional’s role is to provide safe access to help (Table 2). This means that victims should never be asked to leave the appointment with a physical list of contacts, as a perpetrator could find it and escalate the danger. Instead, patients should be assured that the office has these resources available and that they can call at any time to get a contact number.
The resource list should be created and maintained by the office staff, and every team member must know its secure location. This list needs to include national resources, such as 24-hour hotlines, as well as local contacts for shelters, victim’s advocacy organizations, nonemergency police, crisis lines, and medical facilities.10,15
![]() Conclusion
Conclusion
Oral health professionals occupy an often underutilized position as frontline responders in the fight against domestic violence. The literature overwhelmingly demonstrates that the oral and maxillofacial regions are primary targets of abuse, with up to 75% of physical assault injuries occurring in the head, neck, and face.6,16 Given this striking statistic, routine dental examinations that inherently involve a thorough assessment of the head and neck offer a necessary point of contact for intervention that victims may not seek elsewhere. However, the efficacy of this role hinges entirely on standardization. Current data show that a significant gap exists between opportunity and action. Integrating trauma-informed training and mandatory reporting protocols into dental and dental hygiene school curricula and continuing education is not just beneficial, but essential.16 The simple act of asking, “Is everything alright at home?” can transform a routine check-up into a life-saving intervention.17
References
- United States Centers for Disease Control and Prevention. About Intimate Partner Violence. Available at cdc.gov/intimate-partner-violence/about/index.html. Accessed January 29, 2026.
- Levin L, Bhatti C. The role of dental professionals in identifying, reporting, and supporting domestic violence victims. Dent Traumatol. 2024;40(Suppl 2):3-9.
- Jones ML, Francisco E. Addressing intimate partner violence. Dimensions of Dental Hygiene. 2014;12(10):63–66.
- Jailwala M, Timmons JB, Gül G, Esshaki D, Ganda K. See the signs. Dimensions of Dental Hygiene. 2015;13(3):48–51.
- Garbin CA, Guimarães e Queiroz AP, Rovida TA, Garbin AJ. Occurrence of traumatic dental injury in cases of domestic violence. Braz Dent J. 2012;23:72-76.
- Parish CL, Pereyra MR, Abel SN, Siegel K, Pollack HA, Metsch LR. Intimate partner violence screening in the dental setting: results of a nationally representative survey. J Am Dent Assoc. 2018;149:112-121.
- Alshouibi EN. General dentists’ readiness and barriers in intimate partner violence screening: a cross-sectional study in Jeddah City. BMC Oral Health. 2022;22:1-7.
- Lemich SA, Freudenthal JJ, Neill K, Bowen DM. Dental hygienists’ readiness to screen for intimate partner violence in the state of Texas. J Dent Hyg. 2018;92:47-55.
- Minnesota Department of Health. IPV Screening Toolkit. Available at health.state.mn.us/docs/communities/fhv /ipvscreentoolkit.pdf. Accessed January 29, 2026.
- Menschner C, Maul A. Key ingredients for successful trauma-informed care implementation. Available at chcs.org/media/Brief-Key-Ingredients-for-TIC-Implementation.pdf. Accessed January 29, 2026.
- Futures Without Violence. Compendium of State and U.S. Territory Statutes and Policies on Domestic Violence and Health Care 2019. Available at futureswithoutviolence.org. Accessed January 29, 2026.
- Maimon-Blau I. Medicolegal aspects of domestic violence against children. Dent Traumatol. 2024;40(Suppl 2):18-22.
- Wathen CN, Mantler T. Trauma- and violence-informed care: orienting intimate partner violence interventions to equity. Curr Epidemiol Rep. 2022;9:233-244.
- Mehra V, Family Prevention Fund. Culturally competent responses for identifying and responding to domestic violence in dental care settings. J Calif Dent Assoc. 2004;32:387-394.
- Health Partners IPVE. A Guide to Support Dental Patients Experiencing Intimate Partner Violence (IPV) and Exploitation. Available at healthpartnersipve.org/wp-content/uploads/2024/06/FINAL-A-Guide-to-Support-Dental-Patients-Experiencing-Intimate-Partner-Violence-IPV-and-Exploitation.pdf. Accessed January 29, 2026.
- Women’s Advocates. Enhancing Dental Professionals’ Response to Domestic Violence. Available at wadvocates.org/wp-content/uploads/2020/01/DENTAL-AND-DV.pdf. Accessed January 29, 2026.
- Trindade TF, da Silva MC, Dietrichkeit Pereira JG, Alves da Silva RH. Dentist’s ability to identify and act upon signs of domestic violence against women. Braz J Dent Educ. 2025;25:2450.
From Dimensions of Dental Hygiene. March/April 2026; 24(2):28-31
