The Role of Food and Nutrients in Oral Health
Dental hygienists should be prepared to provide sound, evidence based information on good nutrition in order to help patients achieve optimal health.
This course was published in the August 2013 issue and expires August 2016. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Identify evidence-based resources for information about nutrition.
- Discuss the role of food and nutrients in maintaining periodontal health and preventing oral disease.
- Explain how food and nutrients affect caries risk.
Consumers are inundated with marketing messages about the latest nutritional fads and health products that are “necessary” to achieve optimal health. Separating fact from fiction can be challenging, and dental professionals should be prepared to help patients understand the role that food and nutrients play in their oral health.
The dental literature has discussed the role of nutrition in periodontal diseases and dental caries for decades. While a patient’s nutritional status does not cause these diseases, it can profoundly affect oral health. The Academy of Nutrition and Dietetics also promotes the role of nutrition in oral health (see Academy of Nutrition and Dietetics’ Statement on Oral Health).1
NUTRITION RESOURCES
Nutrients are divided into six categories: carbohydrates, lipids, proteins, vitamins, minerals, and water. Carbohydrates, lipids, and proteins are macronutrients, which provide energy or calories. As micronutrients, vitamins and minerals are required in small quantities to maintain health. Each nutrient has its own role in the body, and they work together to support growth, development, maintenance, resistance, and repair of the oral cavity, while also regulating essential body processes. This intricate process is interrupted when nutrients are inadequate or in excess.
Research-based nutrition tools, such as the Dietary Guidelines for Americans (www.health.gov/dietaryguidelines/2010.asp) and Choose MyPlate (www.choosemyplate.gov), offer dental professionals resources for educating patients about healthy eating. These guidelines, published by the United States Department of Agriculture and the US Department of Health and Human Services, are updated every 5 years. A committee of health care professionals is currently reviewing the scientific data in preparation for the 2015 guidelines. A valuable education tool, the guidelines stress the importance of a nutrient-dense diet, consumption of food in proper portions, adherence to appropriate calorie requirements, and the value of physical activity.
No single food contains all of the essential nutrients in the amounts needed for health. Presenting these educational messages (vs guiding patients to specific nutrients or foods) provides access to effective and practical information.2 If the patient’s nutritional needs fall outside the realm of these guidelines, a referral to his or her primary care provider or a registered dietitian for medical nutrition therapy is necessary.
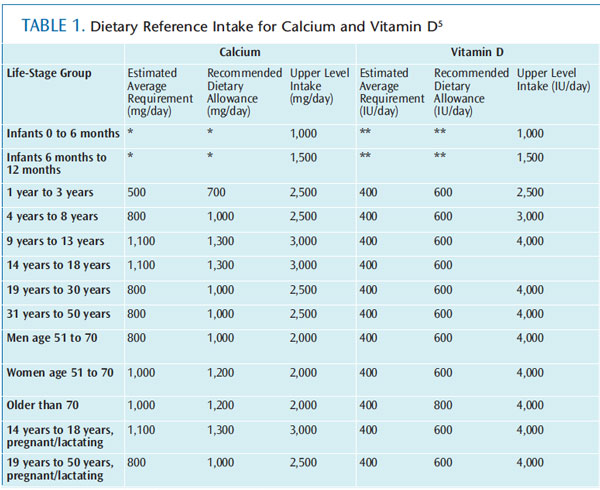
The Dietary Reference Intake (DRI) is an evidence-based system of recommendations for healthy nutrition established by the Institute of Medicine. Table 1 provides the DRIs for calcium and vitamin D. The recommended dietary allowance (RDA), adequate intake (AI), estimated average requirement (EAR), and tolerable upper intake level (UL) are all part of the DRI system.3 Each DRI is classified according to gender and life-stage group. RDA is the level of nutrient needed to meet the requirements of most individuals.
AI is the recommended amount of a nutrient based on scientific judgment. For example, the nutrient level for vitamin K, which is synthesized in the body, is classified as AI because the amount needed to maintain health is unclear. EAR determines the amount of nutrient needed to meet the needs of half of the individuals in a specific population. Finally, UL is the maximum daily amount of a nutrient that can be consumed before it causes toxic effects.4
PERIODONTAL DISEASES
Patients’ dietary intake can have a positive or negative effect on the periodontium. The normal growth and development of periodontal and oral mucosal tissues begins during gestation. Optimal oral health depends on sufficient intake of vitamin A (salivary glands, epithelial tissue), vitamin C (collagen, connective tissue), and vitamin B complex (epithelial and connective tissue). Calcification and adequate density of the alveolus and cementum happen at 16 weeks in utero and require protein, calcium, phosphorus, vitamin D, vitamin K, boron, and magnesium.
Vitamin D intake during pregnancy is associated with bone ossification. The new guidelines from the American College of Obstetrics and Gynecology and the Institute of Medicine both recommend supplementing with 600 IU daily vitamin D during pregnancy to support maternal and fetal bone metabolism.5–7 The availability of nutrients in utero is essential to the growth and development of the periodontium.
Excessive supplementation during pregnancy, however, can also have deleterious effects. For this reason, dental hygienists should discuss the role of nutrition in the growth and development of the oral cavity with pregnant patients. Choose MyPlate offers nutritional guidelines for pregnant and breastfeeding women.
The soft tissues of the oral cavity are some of the first to develop clinical signs of nutrient deficiencies, due to the 3-day to 7-day turnover of most oral mucosal cells.1 Nutrients work together, and, as such, clinical observations are usually indicative of not just one, but several nutrient deficiencies. In addition, clinical signs observed in an intraoral and extraoral examination are not sensitive enough to diagnose a nutrient deficiency. A diagnosis is made through a comprehensive oral exam; medical, dental, and dietary assessment; and laboratory analyses. When a clinician suspects an imbalance of nutrients in a patient, a referral to his or her primary care provider or a registered dietitian may be warranted.
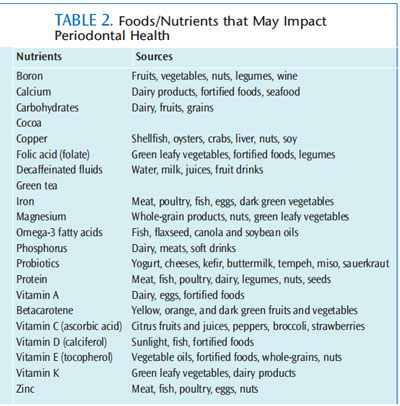
Maintenance and repair of oral tissues, in addition to the health of patients’ immune and repair responses, require sufficient levels of the following: vitamins A, C, D and E; proteins; carbohydrates; calcium; iron; zinc; folic acid; copper; and omega-3 fatty acids.1,8–10 Higher kilocalorie ranges also are indicated for in creased metabolic needs required in the presence of infection, blood loss, catabolism of tissue, trauma (eg, from surgery), repair, and wound healing. Hemorrhage, bluish red gingiva, a widened periodontal ligament, and tooth mobility may be oral signs of a vitamin C deficiency (Figure 1). Vitamin D and calcium levels have been linked to periodontal problems, due to their role in bone homeostasis, including attachment and bone and tooth loss.6 Oral health professionals may use this information to emphasize the need for a varied diet of nutrient-dense foods. Table 2 provides a list of foods and beverages rich in these nutrients.
The effects of tea and probiotics on oral health have been studied. The polyphenols in green tea have been examined for positive effects on the treatment of periodontal diseases, but the evidence remains inconclusive. 11–13 The use of probiotics—live microorganisms that help support the balance of microflora—has also gained popularity for its association with periodontal health. Emerging evidence reveals probiotics may inhibit the growth of plaque biofilm and bacteria associated with periodontal diseases.14–19

Probiotics differ in strains and strengths. Determining the correct probiotic for a periodontal problem is essential, and the process is complex. Currently, there is a small body of evidence supporting the value of probiotics to maintain or promote periodontal health; more research is necessary.14–19 Drinking green tea and consuming probiotics are healthy choices, however, and, thus, may be incorporated into patients’ daily intake in proper portion sizes.
Patients need to maintain adequate nutrient stores prior to periodontal surgery to support successful outcomes. This ensures an acceptable immunological response for optimal healing, and can help prevent or minimize infections. A patient with anorexia nervosa, for example, should increase his/her nutrient intake prior to oral surgery to ensure appropriate healing. This may require postponement of the procedure to allow time for nutrient reserves to reach sufficient levels. Supplementation beyond the DRIs is not recommended; however, the evidence on this practice is inconclusive.
Prevention and therapeutic management of periodontal diseases require adequate nutrition. Reviewing the tools, Dietary Guidelines for Americans and Choose MyPlate, can assist dental hygienists in conducting a nutritional assessment with patients, which, ultimately, can reveal dietary imbalances that should be corrected for optimal oral health. Choosing nutrient-dense foods is generally the best strategy for meeting nutritional needs, promoting optimal health, and reducing the risk of periodontal diseases.20 A multivitamin (no nutrient exceeds 100% of the daily value, as indicated on the label) may be required when a dietary gap is assessed.20 Dietary supplements, however, cannot replace a healthy diet. With the addition of supplements, it is easy to exceed the UL for some nutrients when a diet is rich in fortified foods.20 With this in mind, referral to a primary care provider or registered dietitian to assess the need for dietary supplementation may be necessary.
DENTAL CARIES
The decay process involves multiple factors, including food and nutrients. Receiving adequate nutrition in utero is required for healthy tooth development. Post-eruption, the foods and beverages consumed can exert beneficial or detrimental effects on caries risk. Much of this information is familiar to dental hygienists, but keeping up-to-date on the research regarding the role of foods and nutrients in the caries process is important.
A tooth’s ability to resist demineralization begins in the preeruptive phase. The sixth week of gestation marks the beginning of tooth development. By 16 weeks, calcification of primary teeth begins. In primary and permanent tooth development, 60% is initiated during gestation. All primary teeth and many permanent teeth are at various stages of development when the infant is born.
Critical periods for tooth development occur at different times. Severe and irreversible damage to dentin or enamel formation results when nutritional imbalances occur during these periods. Nutrient deficiencies can also cause a reduction in tooth size, problems in tooth formation, delay in tooth eruption, and an increased susceptibility to caries. Adequate nutrients must be available for the development of preeruptive teeth throughout pregnancy. An imbalance of nutrients may result in deficient tooth structures.21 Formation of strong dentin and enamel depend on many nutrients: vitamin C for formation of collagen matrix, and calcium, magnesium, phosphorus, and vitamin D for enamel formation and mineralization. Vitamin D deficiency during pregnancy may increase caries risk; however, further research is needed on this subject.22 During maturation of teeth, adequate vitamin D status may reduce the incidence of dental caries, especially for children age 13 and younger.22 Vitamin A is essential for the production of keratin in enamel. Table 3 lists the foods and nutrients that may impact dental caries.
A discussion about nutrition with pregnant women and mothers/caregivers of young children in the dental office should focus on its relationship to the growth and development of the teeth. Assessing the dietary intake of the mother/caregiver and the child may uncover nutrient imbalances and/or missing food groups. Promoting the consumption of a variety of healthy foods, and suggesting food sources rich in vitamin C, vitamin D, calcium, magnesium, and phosphorus are important.
Foods that may be protective against caries, due to their ability to increase plaque pH or support of remineralization, include protein, fat, phosphorus, and calcium. 21 Recommending additional protein or fat sources is not always in the best interest of patients because they can cause unwanted increases in calories, saturated fat, and cholesterol.
The anticariogenic potential of sugar alcohols (polyols), most notably xylitol and sorbitol, has been widely studied with varying results.23–25 Evidence shows that sugar alcohols may reduce the risk of decay and support remineralization because they are not fermented by oral microorganisms, they interfere with the metabolism of substrates, and inhibit the adhesion of Streptococcus mutans to tooth structure.23 Nonnutritive sweeteners, such as aspartame, saccharin, sucralose, contain no calories, are not metabolized by microorganisms, and do not have an effect on caries activity.
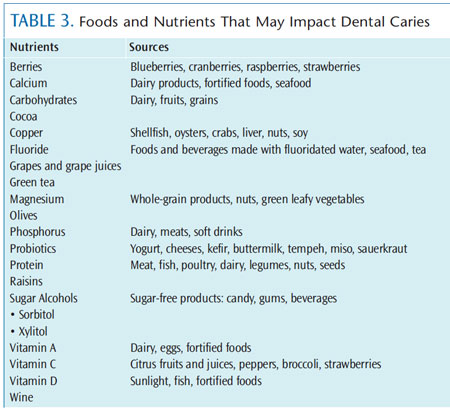
Evolving studies suggest that adequate copper intake has an antimicrobial effect and may inhibit demineralization, possibly reducing the risk of caries (see Table 3 for a list of foods rich in copper).24 Other studies are investigating the anticariogenic activity of tea, cocoa, coffee, olives, berries, raisins, grapes and grape juices, and wine due to their antimicrobial potential.12,24–28 These plant polyphenols are antioxidant phytochemicals thought to prevent or neutralize the damaging effects of free radicals. The use of probiotics for caries reduction, due to their inhibitory effect against S. mutans and S. sorbrinus, is also under investigation.24,29,30
Further research is required before general recommendations for all populations can be provided on the use of these foods/nutrients to prevent or treat caries. Dental hygienists can provide objective, evidence-based nutrition information to guide patients in a healthier direction, including optimal oral hygiene.
CONCLUSION
There is a multidirectional association between diet and nutrition and oral health. An imbalance of nutrients can influence oral health, such as periodontal disease and dental caries status. Conversely, oral issues can affect patients’ ability to consume an adequate diet. Therefore, dental professionals should include diet and nutrition as a component of the dental and medical assessment for optimum oral health. The Dietary Guidelines for Americans and Choose MyPlate, along with DRIs, provide valuable tools for dental hygienists to use in dietary assessment and education. If the nutrition intervention requires more complex and extensive information, the patient should be referred to his or her primary care provider or a registered dietitian for medical nutrition therapy. Collaborating with other health disciplines to design and implement the treatment plan helps support the provision of optimal care for patients.
The role of foods and nutrients in periodontal diseases and dental caries begins in utero with the growth and development of oral hard and soft tissues. The value of food and nutrients continues through maintenance and repair of the periodontium and remineralization or other protective mechanisms involved in the caries process. Oral health professionals should encourage patients to consume a wide variety of nutrient-dense foods and beverages rather than recommend specific foods or nutrients, as well as to maintain proper portion control and adhere to calorie intake requirements.
The continued examination of current, relevant, and evidence-based information regarding nutrition is critical to the effective education of patients.
ACKNOWLEDGMENT
FIGURE 1. ST. MARY’S HOSPITAL MEDICAL SCHOOL / SCIENCE SOURCE
REFERENCES
- Touger-Decker R, Mobley C, Academy ofNutrition and Dietetics. Position of the Academy of Nutrition and Dietetics: oral health and nutrition. J Acad Nutr Diet. 2013;113:693–701.
- Freeland-Graves JH, Nitzke S, Academy of Nutrition and Dietetics. Position of the academy of nutrition and dietetics: total diet approach to healthy eating. J Acad Nutr Diet. 2013;113: 307–317.
- Institute of Medicine, Food and NutritionBoard. Dietary Reference Intakes: Applications in Dietary Assessment. Washington, DC: National Academy Press; 2000.
- Wansink B, American Dietetic Association.Position of the American Dietetic Association: food and nutrition misinformation. J Am Diet Assoc. 2006;106:601–607.
- Urrutia RP, Thorp JM. Vitamin D in pregnancy:current concepts. Curr Opin Obstet Gynecol. 2012; 24:57–64.
- Institute of Medicine of the NationalAcademies, Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academy Press; 2011.
- The American College of Obstetricians andGynecologists: Committee Opinion. Vitamin D: Screening and Supplementation During Pregnancy. Available at: www.acog.org/~/media/Committee%20Opinions/Committee%20on%20Obstetric%20Practice/co495.pdf–dmc=1&ts=20130722T1627324701. Accessed July 22, 2013.
- Van der Velden U, Kuzmanova D, Chapple ILC.Micronutritional approaches to periodontal therapy. J Clin Periodontol. 2011;38(Suppl 11):142–158
- Iwasaki M, Manz MC, Taylor GW, Yoshihara A,Miyazaki H. Relations of serum ascorbic acid and alpha-tocopherol to periodontal disease. J Dent Res. 2012;91:167–172.
- Naqvi AZ, Buettner C, Phillips RS, Davis RB,Mukamal KJ. N-3 Fatty acids and periodontitis in US adults. J Am Diet Assoc. 2010;110:1669–1675.
- Venkateswara, B, Sirisha K, Chava VK. Greentea extract for periodontal health. J Indian Soc Periodontol. 2011;15:18–22.
- Narotzki B, Reznick, AZ, Aizenbud D, Levy Y.Green tea: a promising natural product in oral health. Arch Oral Biol. 2012;57:429–435.
- Chatterjee A, Saluja M, Agarwal G, Alam M.Green tea: A boon for periodontal and general health. J Indian Soc Periodontol. 2012;16:161–167.
- Chatterjee A, Bhattacharya H, Kandwal A.Probiotics in periodontal health and disease. J Indian Soc Periodontol. 2011;15:23–28.
- Dhingra K. Methodological issues in randomized trials assessing probiotics for periodontal treatment. J Periodont Res. 2012;47:15–26.
- Gupta G. Probiotics and periodontal health.J Med Life. 2011;4:387–394.
- Koduganti RR, Sandeep N, Guduguntla S,Chandana Gorthi VS. Probiotics and prebiotics in periodontal therapy. Indian J Dent Res. 2011;22:324–330.
- Slawik S, Staufenbiel I, Schilke R, et al.Probiotics affect the clinical inflammatory parameters of experimental gingivitis in humans. Eur J Clin Nutr. 2011;65:857–863.
- Teughels W, Loozen G, Quirynen M. Do probiotics offer opportunities to manipulate the periodontal oral microbiota? J Clin Periodontol. 2011;38(Suppl 11):159–177.
- Marra MV, Boyar AP. Position of the AmericanDietetic Association: nutrient supplementation.J Am Diet Assoc. 2009;109:2073–2085.
- Stegeman CA, Davis J. The Dental Hygienist’sGuide to Nutritional Care . 4th ed. St. Louis:Elsevier. In press.
- Hujoel PP. Vitamin D and dental caries in controlled clinical trials: systematic review and meta-analysis. Nutr Rev. 2013;71:88–97.
- Trahan L. Xylitol: a review of its action on mutans streptococci and dental plaque—its clinical significance. Int Dent J. 1995;45:77–92.
- van Loveren C, Broukal Z, Oganessian E.Functional foods/ingredients and dental caries. Eur J Nutr. 2012;51(Suppl 2):S15–S25.
- Bader JD, Vollmer WM, Shugars DA, et al.Results from the Xylitol for Adult Caries Trial (XACT). J Am Dent Assoc. 2013;144:21–30.
- Wong A, Young DA, Emmanouil DE, WongLM, Waters AR, Booth MT. Raisins and oral health. J Food Sci. 2013;78(Suppl 1):A26–A29.
- Vislocky LM, Fernandez ML. Grapes andgrape products: their role in health. Nutrition Today. 2013;48(1):47–51.
- Naderi NJ, Niakan M, Kharazi Fard MJ, ZardiS. Antibacterial activity of Iranian green and black tea on streptococcus mutans: An in vitro study. J Dent (Tehran). 2011;8(2):55–59.
- Chuang LC, Huang CS, Ou-Yang LW, Lin SY.Probiotic Lactobacillus paracasei effect on cariogenic bacterial flora. Clin Oral Investig. 2011;15:471–476.
- Teanpaisan R, Piwat S, Dahlen G. Inhibitoryeffect of oral Lactobacillus against oral pathogens. Lett Appl Microbiol. 2011;53:452–459.
From Dimensions of Dental Hygiene. August 2013; 11(8): 26–30.
