 DARDESPOT/E+/GETTY IMAGES PLUS. SUBJECT IS A MODEL AND USED FOR ILLUSTRATIVE PURPOSES
DARDESPOT/E+/GETTY IMAGES PLUS. SUBJECT IS A MODEL AND USED FOR ILLUSTRATIVE PURPOSES
Caring for Patients With Alzheimer Disease
The provision of comprehensive, person-centered care for individuals with this neurodegenerative condition is key to maintaining quality of life.
This course was published in the November 2021 issue and expires November 2024. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define Alzheimer disease (AD).
- Explain the similarities between the immune response generated by AD and periodontitis.
- Identify oral health risk factors associated with AD.
- Discuss the role of the dental hygienist in treating patients with AD.
Alzheimer disease (AD) is a progressive neuroinflammatory condition characterized by memory and communication loss, as well as cognitive decline. The most common form of dementia, AD affects more than 6 million Americans over the age of 65, and is the sixth leading cause of death nationwide.1 Dementia is an umbrella term used to describe a group of symptoms that affect intellectual and social abilities severely enough to interfere with daily function.2 There is currently no known cause or cure of AD; however, common risk factors include age, gender, genetics, brain injury, obesity, diabetes, and environmental factors, such as air pollution or geographic location.3
AD encompasses several different stages, including preclinical, mild cognitive impairment, and severe dementia. During the preclinical phase, patients do not show signs of AD, but neuropathologic changes and inflammatory biomarkers are still present. Biological changes of AD can begin years, possibly even decades before the patient experiences any clinical symptoms. Warning signs of mild cognitive impairment include difficulty finding words, diminished reasoning, visual or spatial awareness impediments, and memory loss. As the illness progresses, memory loss becomes more apparent. Some patients experience mood or behavioral changes, as well as difficulty with language, problem solving, and recognizing family members and friends. Signs of late-stage AD include loss of bowel and bladder control, weight loss, inability to communicate or swallow, seizures, and increased sleeping.4
Etiology of Neuroinflammation
Though the initial cause of AD is unknown, its neuropathological hallmarks include the accumulation of ß-amyloid plaques and the formation of neurofibrillary tangles containing tau protein in brain tissue.1–5 The presence of ß-amyloid plaques and tau protein tangles activates a host immune response, resulting in the release of pro-inflammatory cells, which contribute to chronic neuroinflammation and, ultimately, the destruction of brain tissue.5 The host immune response observed in AD is similar to that of periodontal diseases. During periodontal diseases, Gram-negative bacteria invade subgingival tissues in the periodontium, causing the release of pro-inflammatory cytokines and chemokines, resulting in the subsequent destruction of alveolar bone and tooth-supporting tissues.6,7 Periodontal therapy reduces the presence of Gram-negative bacteria, inflammation, and disease destruction.8
Research suggests a bidirectional relationship between AD and periodontal diseases.9 Elevated levels of pro-inflammatory mediators, interleukins, tumor necrosis factor-alpha, C-reactive protein, and matrix metalloproteinases, are present in both AD and periodontal diseases.7,9,10 Risk factors such as age, tobacco use, genetics, obesity, and socioeconomic status, may influence the pathogenesis of AD and periodontal diseases as well.9 Studies have demonstrated a reduction of pro-inflammatory mediators systemically after scaling and root planing;8 however, nonsurgical periodontal therapies are not widely used to treat most chronic conditions affecting other body systems.
Studies also suggest Porphyromonas gingivalis may be a contributing factor in the development of AD, and it has been found in the brain tissue of deceased patients with AD.11 Mice studies have shown that P. gingivalis can travel from the oral cavity, through the bloodstream, into the brain;12 however, this has yet to be demonstrated in human subjects. While the detrimental effects of periodontal diseases on other major systemic diseases have been demonstrated, a causative relationship between periodontal diseases and AD has not been established.
![TABLE 1. Medications Approved for the Management or Treatment of Alzheimer Disease]() Management of Alzheimer Disease
Management of Alzheimer Disease
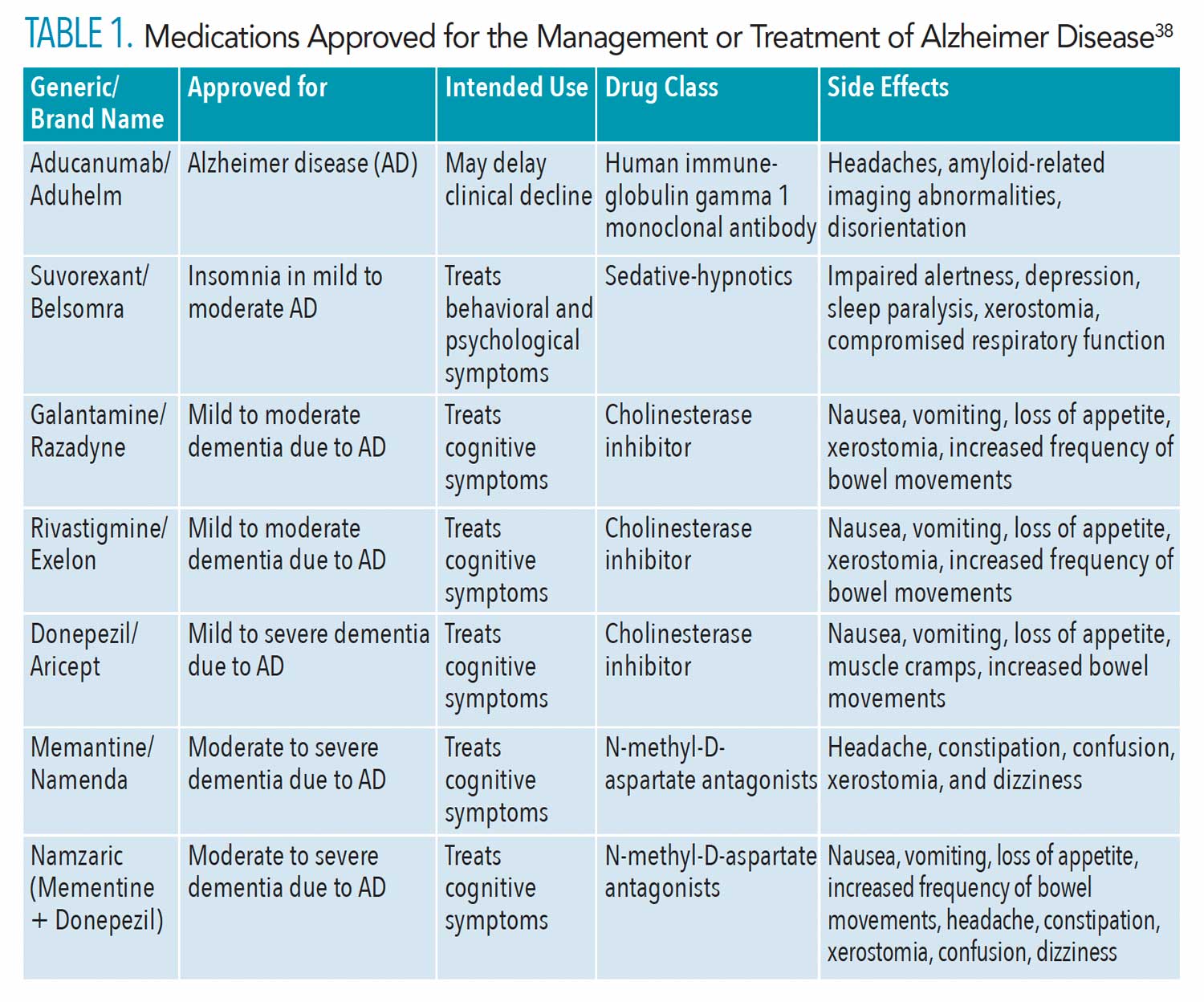
Therapies, including both pharmacological and nonpharmacological management, are available to reduce AD signs and symptoms, while improving overall quality of life. The United States Food and Drug Administration (FDA) has approved several cholinesterase inhibitors (Table 1), which may reduce or delay AD symptoms.13 The efficacy of these drugs, however, is limited, and major side effects include nausea, fatigue, weight loss, and hyposalivation.14 Aducanumab, a monoclonal antibody therapy for ß-amyloid, has received accelerated approval from the FDA for the treatment of AD.15 Aducanumab is the first therapy that targets the fundamental pathophysiological changes seen in AD.16 The most common side effects are amyloid-related imaging abnormalities, headaches, and disorientation.15,16 Aducanumab reduces the amount of ß-amyloid plaque in the brain,16 but it has yet to show either reduced decline, stability, or improvement of cognitive function following decreases in plaque.17 Failure to show efficacy has created controversy over the FDA approval; however, efficacy is not required for accelerated approval of drugs that treat serious conditions.
The emotional and behavioral changes linked with AD can be difficult to manage. Individuals with AD may experience depression, anxiety, sleep problems, or irritability.4 These experiences may be triggered by environmental changes or when prompted to perform routine hygiene tasks, such as brushing their teeth or taking a bath.18 Managing triggers will help to reduce the frequency and severity of these emotional and behavioral changes, while providing comfort and security for those with AD. In severe cases, medications such as antidepressants, antianxiety, or antipsychotic drugs, can be prescribed by a physician.19
Exercise is an effective nonpharmacological management strategy and improves cognitive function for all stages of AD.20 Exercise also helps combat disease modifying risk factors, such as depression, diabetes, and obesity. A hallmark symptom of AD is the progressive shrinkage of the hippocampus, which is responsible for storing long-term memories, spatial processing, and navigation.21 A meta-analysis by Wilckens et al21 found a year of mild-to-moderate exercise preserved hippocampal volume in at-risk older adults. Exercise has few side effects and better compliance when compared to medications. Though dental hygienists primarily focus on oral hygiene instruction, they should discuss the benefits of physical activity on brain health during preventive care appointments for at-risk patients.
Diagnosis and therapeutic interventions in the preclinical stage of AD can preserve brain function and delay symptom onset.22 Early diagnosis can also help patients live independently and maintain a better quality of life. Patients may also preemptively make legal, financial, and future care plans to avoid any complications during the more severe stages of AD.22 Currently, diagnostic biomarkers for AD are tested via cerebral spinal fluid collection through painful lumber punctures; however, salivary diagnostics for ß-amyloid and tau protein are in development. Current research shows that salivary biomarkers can be used to diagnose AD.23 Further research is necessary before this testing can be widely implemented.
Oral Considerations for Alzheimer Disease
Research suggests that severe periodontitis increases the risk of developing dementia by an odds ratio of 1.17, and patients with dementia are 69% more likely to be diagnosed with periodontal diseases than those without.24 Additionally, patients diagnosed with AD are at increased risk of partial or complete edentulism compared to control groups.25 During early stages of AD, dental care should focus on disease prevention and oral health maintenance. Preventive oral healthcare is critical for the preservation of overall health and quality of life. As AD progresses, the risk of oral disease increases because the ability to adequately and/or consistently perform oral hygiene tasks declines. Common oral conditions associated with AD include dental caries, hyposalivation, and periodontal diseases.26
Due to the degenerative nature of AD, caries risk assessments should be performed at each hygiene appointment. Clinical assessments, along with current AD status and/or cognitive function, must be considered in the caries risk assessment process. Prescription and over-the-counter fluoride applications should be used for caries prevention. Fluoride, whether self-applied, professionally applied, or delivered through community water systems, reduces the incidence of caries by at least 25%.27 In advanced stages of AD, prescribed topical fluoride supplements, such as toothpastes or mouthrinses, should be stored in a secure location to avoid accidental ingestion.
Silver diamine fluoride (SDF) is ideal for this patient population, as it arrests active dentin caries and is an effective interim therapy.28 SDF application, however, is not a replacement for permanent restorative treatment. Dental hygienists are permitted to apply SDF under the same authorization as other topical fluorides.29
Hyposalivation in patients with AD is often medication induced. To help address hyposalivation, dental hygienists should assess salivary gland function at each preventive or maintenance appointment.30 Saliva substitutes, increased water consumption, and caries-reducing strategies should be considered.30 During advanced stages of AD, a humidifier in the patient’s home may help reduce the severity of xerostomia.
The Role of the Dental Hygienist
Dental hygienists must be prepared to provide comprehensive, person-centered care for individuals with AD. Person-centered care requires a treatment plan for a person, not his or her disease. Collecting biographical information or interacting with family members can help personalize a care plan.31 Evaluating the patient’s cognitive function and physical ability can also inform the creation of an individualized therapeutic care plan. Dental hygienists can personalize preventive care appointments through collaborative efforts with oral health professionals, medical providers, and caregivers.
When providing person-centered dental care for patients diagnosed with AD, dental hygienists should consider the following:32
- Work closely with the patient and/or caregiver to schedule appointments at a time that is most ideal for the patient.
- Encourage 3-month, 4-month, or 6-month preventive/periodontal recare intervals depending on the patient’s oral health status.
- Allow for longer appointment times.
- Prevent falls by moving cords and adjusting the dental chair to an appropriate height.
- Minimize distractions and noise in the patient care room. This may require seating the patient in a secluded room to avoid excessive noise from surrounding treatment rooms.
- Avoid the use of dental terminology when appropriate to reduce confusion.
- Use assistive devices such as bite-wedges, metal finger guards, or a neck pillow and blanket to ensure comfort and safety.
- Palliative/emergency care is dependent on patient’s ability to cooperate. In severe cases when general anesthesia may be required, the value of the natural dentition should be assessed.
Intra- and Interprofessional Collaboration
AD places significant burden on patients, caregivers, providers, and healthcare delivery systems.33 As such, dental hygienists need to collaborate with dental and medical healthcare team members in order to provide comprehensive person-centered care and reduce the impact of disease.33 Within the dental office, dental hygienists and dentists work together to diagnose and meet the oral health needs of all patients. In the advanced stages of AD, the patient may require extensive treatment or accommodations. If the dental practice or provider is unable to provide adequate and safe care, referrals to oral health professionals who have experience treating patients with AD should be considered.
Interprofessional collaboration improves person-centered care, reduces medical errors and healthcare costs, provides early diagnosis and intervention, and optimizes medication or treatment regimens.34 Unfortunately, communication between disciplines is one of the greatest barriers to providing comprehensive treatment.35 The dental practice should maintain a comprehensive list of all healthcare providers and caregivers providing direct care for the patient with AD, as well as a complete list of medications and other treatment modalities. Additionally, many patients with AD reside in long-term care facilities and have limited access to dental care. Some states allow dental hygienists to practice in nontraditional settings, such as long-term care facilities or hospitals.36 Direct access agreements vary between states, so dental hygienists should stay up to date on current regulations and operate within their scope of practice or push for legislation allowing expanded dental hygiene functions in alternative settings.
Caregiver Support and Oral Health Education
Caregivers play a vital role in the oral health maintenance of people with AD; therefore, effective communication and rapport between caregivers and the dental team are essential. Caregivers may require oral health training and education to properly care for those with AD. Providing short and simple instructions on how to provide oral care to their loved one is a good starting point.37 The mirroring technique is a strategy in which the caregiver demonstrates how to perform oral hygiene, while the patient mirrors his or her actions at the same time.37 This may be most effective when caring for patients who have lost the ability to follow step-by-step instructions. Encourage caregivers to experiment with different methods to find what works best for the patient. Training for effective handling and cleaning of removable dentures may be necessary in some cases.37 In the advanced stages of AD, the caregiver should continue to support and encourage good oral health to the best of his or her ability.
While the patient’s health is a caregiver’s chief concern, quality of life is equally important. Oral diseases can lead to other health disparities including eating difficulties, digestive problems, malnutrition, and increased risk of infections.26 Loss of appetite in those with AD is a cardinal sign of oral discomfort.26 With the support and education given by dental hygienists, caregivers and family members have the greatest opportunity to recognize oral diseases in their earliest stages.
Conclusion
AD is a progressive and debilitating neuroinflammatory condition with no known cause or cure. Individuals diagnosed with AD have an increased risk of poor oral health outcomes. Dental hygienists should work closely with healthcare teams and caregivers to maintain patients’ oral health. Above all, a dental hygienist’s ethical responsibility is to provide education to patients and caregivers on health promotion and disease prevention.
References
- National Institute on Aging. Alzheimer’s Disease Fact Sheet. Available at: nia.nih.gov/health/alzheimers-disease-fact-sheet. Accessed October 20, 2021.
- Alzheimer’s Association. What Is Dementia? Available at: alz.org/alzheimers-dementia/what-is-dementia? Accessed October 20, 2021.
- Armstrong R. Risk factors for Alzheimer’s disease. Folia Neuropathol. 2019;57:87–105.
- National Institute on Aging. What Are the Signs of Alzheimer’s Disease? Available at: nia.nih.gov/health/what-are-signs-alzheimers-disease. Accessed October 20, 2021.
- Kametani F, Hasegawa M. Reconsideration of amyloid hypothesis and tau hypothesis in Alzheimer’s disease. Front Neurosci. 2018;12:25.
- Kinane DF. Causation and pathogenesis of periodontal disease. Periodontol 2000. 2001;25:8–20.
- Cekici A, Kantarci A, Hasturk H, et al. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol 2000. 2014;64:57–80.
- Acharya AB, Thakur S, Muddapur MV. Effect of scaling and root planing on serum interleukin-10 levels and glycemic control in chronic periodontitis and type 2 diabetes mellitus. J Indian Soc Periodontol. 2015;19:188–193.
- Kamer AR, Craig RG, Niederman R, et al. Periodontal disease as a possible cause for Alzheimer’s disease. Periodontol 2000. 2020;83:242–271.
- Rempe RG, Hartz AMS, Bauer B. Matrix metalloproteinases in the brain and blood-brain barrier: versatile breakers and makers. J Cereb Blood Flow Metab. 2016;36:1481–1507.
- Dominy SS, Lynch C, Ermini F, et al. Porphyromonas gingivalis in Alzheimer’s disease brains: evidence for disease causation and treatment with small-molecule inhibitors. Sci Adv. 2019;5:1.
- Ishida N, Ishihara Y, Ishida K, et al. Periodontitis induced by bacterial infection exacerbates features of Alzheimer’s disease in transgenic mice. NPJ Aging Mech Dis. 2017;3:15.
- Sharma K. Cholinesterase inhibitors as Alzheimer’s therapeutics (Review). Mol Med Rep. 2019;20:1479–1487.
- Rewgenold W, Loreck D, Brandt N. Prescribing cholinesterase inhibitors for Alzheimer’s disease: timing matters. Am Fam Physician. 2018;97:700.
- United States Food and Drug Administration. Aduhelm. Available at: accessdata.fda.gov/drugsatfda_docs/label/2021/761178s000lbl.pdf. Assessed October 20, 2021.
- Schneider L. A resurrection of aducanumab for Alzheimer’s disease. Lancet Neurol. 2020;19:111–112.
- Alzforum. Aducanumab Approved to Treat Alzheimer’s Disease. Available at: alzforum.org/news/research-news/aducanumab-approved-treat-alzheimers-disease. Assessed October 21, 2021.
- Gould E, Reed P. Alzheimer’s Association Quality Care Campaign and professional training initiatives: improving hands-on care for people with dementia in the USA. Int Psychogeriatr. 2009;21(Suppl 1):S25–S33.
- Calsolaro V, Antognoli R, Okoye C, et al. The use of antipsychotic drugs for treating behavioral symptoms in Alzheimer’s disease. Front Pharmacol. 2019;10:1465.
- Meng Q, Lin MS, Tzeng IS. Relationship between exercise and Alzheimer’s disease: a narrative literature review. Front Neurosci. 2020;14:131.
- Wilckens KA, Stillman CM, Waiwood AM, et al. Exercise interventions preserve hippocampal volume: a meta-analysis. Hippocampus. 2021;31:335–347.
- Chu LW. Alzheimer’s disease: early diagnosis and treatment. Hong Kong Med J. 2012;18:228–237.
- Pawlik P, Błochowiak K. The role of salivary biomarkers in the early diagnosis of Alzheimer’s disease and Parkinson’s disease. Diagnostics (Basel). 2021;11:371.
- Ju X, Kapellas K, Jamieson L, et al. The association between periodontal disease and dementia: a systematic review and meta-analysis. J Oral Biol Craniofac Res. 2019;2:2–11.
- Dioguardi M, Gioia GD, Caloro GA, et al. The association between tooth loss and Alzheimer’s disease: a systematic review with meta-analysis of case control studies. Dent J (Basel). 2019;7:49.
- Gao SS, Chu CH, Young FYF. Oral health and care for elderly people with Alzheimer’s disease. Int J Environ Res Public Health. 2020;17:5713.
- American Dental Association. Fluoridation Facts. Available at: ada.org/~/media/ADA/Files/Fluoridation_Facts.pdf?la=en. Assessed October 20, 2021.
- Subbiah GK, Gopinathan NM. Is silver diamine fluoride effective in preventing and arresting caries in elderly adults? A systematic review. J Int Soc Prev Community Dent. 2018;8:191–199.
- American Dental Hygienists’ Association. State Specific Information on Silver Diamine Fluoride. Available at: adha.org/resources-docs/Silver_Diamine_Fluoride_State_by_State_Information.pdf. Assessed October 21, 2021.
- Alabdullah J, Almuntashiri A. Strategies for safe and effective treatment of patients with Alzheimer disease. Dimensions of Dental Hygiene. 2020;18(7):32–35.
- Godfrey M, Young J, Shannon R, et al. Person-centred care: meaning and practice. In: Godfrey M, Young J, Shannon R, et al. The person, interactions and environment programme to improve care of people with dementia in hospital: a multisite study. NIHR Journals Library. June 2018.
- Marchini L, Ettinger R, Caprio T, et al. Oral health care for patients with Alzheimer’s disease: an update. Spec Care Dentist. 2019;39:262–273.
- Galvin JE, Valois L, Zweig Y. Collaborative transdisciplinary team approach for dementia care. Neurodegener Dis Manag. 2014;4:455-469.
- Reeves S, Pelone F, Harrison R, et al. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2017;6:CD000072.
- O’Daniel M, Rosenstein AH. Professional communication and team collaboration. In: Hughes RG. Patient Safety and Quality: an Evidence-Based Handbook for Nurses. Rockville, Maryland: Agency for Healthcare Research and Quality; April 2008.
- Falcon CI, Coplen AE, Davis-Risen S, et al. Impact of an interprofessional education intervention and collaborative practice agreements of expanded practice dental hygienists in Oregon. J Dent Hyg. 2020;94:6–15.
- Manchery N, Subbiah GK, Nagappan N, et al. Are oral health education for carers effective in the oral hygiene management of elderly with dementia? A systematic review. Dent Res J (Isfahan). 2020;17:1–9.
- Alzheimer’s Association. FDA-Approved Treatment for Alzheimer’s. Available at: alz.org/media/documents/fda-approved-treatments-alzheimers-ts.pdf. Accessed October 20, 2021.ers-ts.pdf. Accessed October 20, 2021.
From Dimensions of Dental Hygiene. November 2021;19(11)40-43.
