
Understanding the Complex Communication Between the Root Canal System and Periodontium
Endodontic-periodontal lesions can mimic one another, making accurate diagnosis crucial for effective treatment. Discovering the different ways the root canal system and periodontium communicate — through lateral canals, dentinal tubules, and fractures — can help pinpoint the primary cause and guide therapy decisions.
Determining the precise etiology of an endodontic-periodontal lesion can be challenging because these lesions can present with similar signs and symptoms. Because successful treatment ultimately relies on an accurate diagnosis, it is critical that the primary etiology be identified before therapy is initiated.
The root canal system and periodontium are interconnected.1 The primary mode of communication between the root canal system and periodontium is through the apical foramina because these openings are the largest, and bacteria and/or their by-products can freely pass through them.
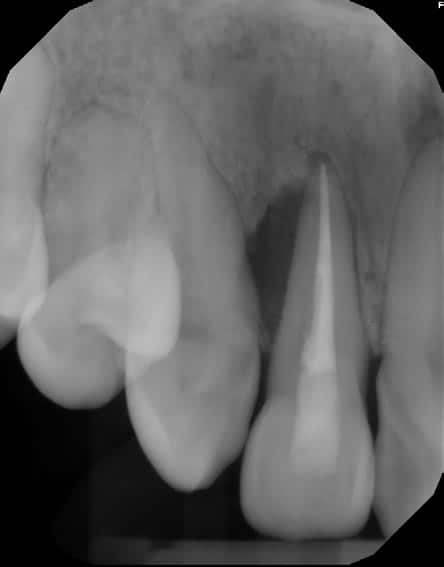
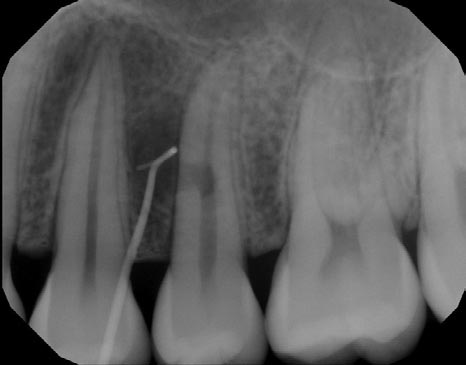
The smaller lateral and/or accessory canals can also act as a mode of communication between the root canal system and periodontium. Lateral and accessory canals are formed during tooth development due to a disturbance in the Hertwig’s epithelial root sheath and subsequent entrapment of blood vessels and connective tissue.2 The incidence of lateral canals varies with root location, with a lower frequency occurring coronally and a higher frequency occurring apically (Figures 1A and 1B).3 Accessory canals can also occur in the furcation region of mandibular molars. One investigator injected ink into molars under pressure and found the presence of furcation canals in 28% of teeth examined; however, the incidence of accessory furcation canals may be as high as 76%.4,5


Note the radiolucency in the furcation adjacent to the lateral canals’ portals of exit. Dentinal tubules are another potential mode of communication between the root canal system and periodontium. These tubules are usually covered with cementum that acts as a physical barrier. However, the cementum can be physically removed during periodontal treatment; in addition, a congenital absence of cementum is also possible. When the cementoenamel junction was studied using a scanning electron microscope, 18% of teeth were found to have exposed dentinal tubules at the cementoenamel junction due to a congenital absence of cementum.6



When the dental pulp is vital, there is an outward flow of dentinal fluid which contains immunoglobulins that can help prevent bacteria and/or their by-products from entering the root canal system.7 However, when the pulp becomes necrotic or the tooth has been previously treated, there is a lack of dentinal fluid, and this allows bacteria or their by-products to invade the root canal system more readily through the exposed dentinal tubules.
Vertical root fractures are yet another potential means of communication between the root canal system and periodontium. Clinical signs of a vertical root fracture include:
- A tooth that was previously treated endodontically
- J-shaped or “halo” radiolucency
- Deep, isolated periodontal pocket
- Coronally located sinus tract
The presence of two sinus tracts on both the buccal and lingual aspects are considered pathognomonic for a vertical root fracture.8 Although cone beam computed tomography has a low specificity for visualization of such fractures, there are common features that can be observed from cone beam imaging.9 These include:
- Loss of bone in the mid-root area, with intact bone coronal and apical to the defect
- Absence of the entire buccal plate of bone
- Radiolucency at the terminus of a post
- Space between the buccal and/or lingual plate of the bone and the root surface
- Visualization of the vertical root fracture10
Developmental malformations, such as vertical radicular grooves, can result in extensive periodontal attachment loss and bone destruction. As the groove becomes contaminated with bacteria and biofilm along its length, periodontal destruction continues until the periodontal pocket eventually reaches the apex of the tooth (Figures 2A through 2D).1




Other potential avenues of communication between the root canal system and periodontium include internal and external resorption (Figures 3A through 3E), perforations (Figure 4), and horizontal root fractures (Figure 5).


This information originally appeared in Dunlap CA, Lundergan WP, Dunlap BC. Diagnosis of endodontic-periodontal lesions. Decisions in Dentistry. 2023;9(2):42-45.
