
Show-Do-Tell: The Importance of Using Disclosing Solution
Help your patients improve their self-care with this simple approach.
Everyone — young or old, healthy or ill, male or female — has an acquired salivary pellicle. It regulates mineral homeostasis and acts as a barrier against acids that impact demineralization and erosion.1,2 The pellicle keeps the mouth moist to aid in speech, mastication, swallowing, etc. Fluoride from saliva also binds to the pellicle and provides protection.3
Unfortunately, the acquired salivary pellicle also becomes a nidus for bacteria and infection.1 The pellicle’s sticky nature allows biofilm and calculus to easily attach, leading to gingivitis and periodontal diseases. It is translucent and not readily visible until a disclosing solution is applied.
Dental Biofilm
Dental biofilms are all around us, on us, and in us. A dangerous powerhouse, dental biofilm is dynamic, structured ,and sophisticated.1 Eventually, these smart, dangerous bacterial colonies mature and release planktonic cells to colonize other areas in the oral cavity.3,4 The daily control of biofilm is the cornerstone of preventing gingivitis and dental caries, and patients must understand the gravity of this challenge.
The best way to demonstrate the importance of biofilm removal is visible, concrete evidence. The show-do-tell method can significantly impact patients’ abilities to retain information and comply with the treatment regimen.
Show. Patients need to be able to see the biofilm, which can be viewed by direct vision in some cases or with an explorer. But the best way to demonstrate biofilm to patients is with a disclosing agent. Effective plaque control must be part of all patients’ treatment plans and disclosing solution is key to success.6 Applying disclosing solution also serves as a self-check for the practitioner and helps motivate patients to include this type of check in their toothbrushing regimens.
Do. Dental disclosing solution is available in both liquid and solid form (chewable tablets). The liquid disclosing solution is easily applied to teeth with an applicator during the patient’s prophylaxis appointment. Place a few drops in a dish and use a cotton swab to apply to all teeth surfaces. Following application, have patient swish with water and expectorate.
Disclosing solution is concentrated and fast acting. All disclosing solutions work by dying residual plaque along the gumline but some differentiate between mature and immature plaque. Most commonly, pink dye adheres to all plaque, whereas the blue dye adheres and diffuses more easily into the denser/thicker plaque. The hope is that the young plaque stains pink and matured plaque stains blue-purple.7 This exercise helps open a line of communication with the patient and instills motivation.
Chewable tablets are also an easy way to get patients involved at home as long as they can easily expectorate. Tablets make it easy to see exactly where problem areas occur. The disclosing substance is a temporary dye with a harmless food coloring (no erythrosine) that can easily be washed off the teeth.
Once the dye has been applied clinically, sit the patient upright and have him or her hold the hand mirror. Ask the patient to demonstrate his or her brushing/flossing technique. Then the patient’s biofilm-free score, a dental hygiene metric that measures the percentage of tooth surfaces that are without plaque and biofilm, can be assessed. It is calculated by dividing the number of biofilm-free surfaces by the total number of available surfaces and multiplying by 100. The higher the score the better.
Tell. Finally, explain to patients that biofilm cannot be completely eliminated, and give them a plan to reduce plaque by brushing twice per day, replacing the brush every 3 months, using an interdental aid, and implementing an antimicrobial chemotherapeutic.
Be careful to not give too many instructions at one time, but rather providing two to five steps is more impactful.8 Start with the basics and build at subsequential appointments. Go slowly help the patient comprehend as much information as possible. Ask the patient to repeat back the instructions to ensure he or she understands.
Documentation
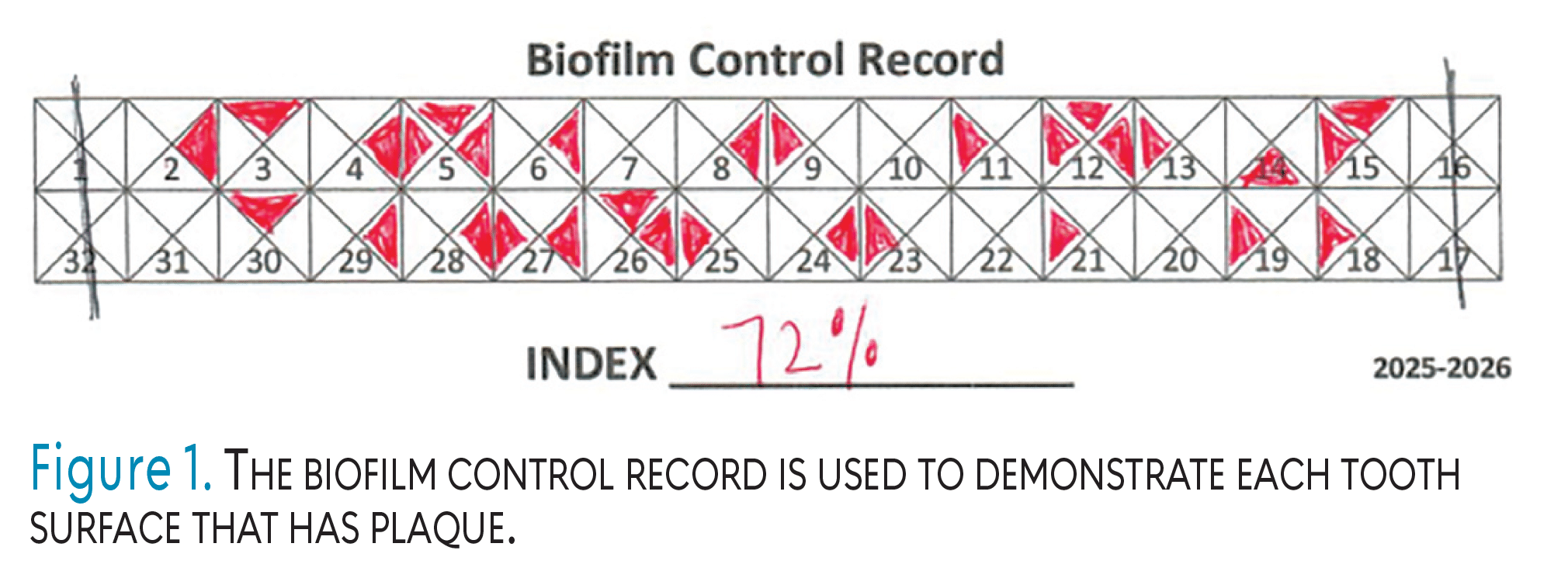
A modified quantitative graph can be used to color in the individual tooth surfaces that have plaque (Figure 1). The percentage of biofilm-free surfaces is ascertained and that information is shared with the patient. Developed by Sigurd Ramfjord, PhD, and Timothy J. O’Leary, DDS, in 1972, the biofilm control record is simple enough to use in large populations for public health education or individual patients at their recare appointments.
Following are the steps for effectively using the biofilm control record.9-11
- Mark the missing teeth on the record form.
- Apply the disclosing agent to the patient’s teeth. Instruct patient to swish and rub the solution over the tooth surfaces with the tongue before rinsing.
- Examine each tooth surface for evidence of plaque biofilm.
- Record each area that is stained by making a dash in the appropriate space on the record form. Record only those surfaces that are stained at the gingival margin or interproximally.
- Calculate the patient’s score. For example, if the patient has 28 teeth and 31 surfaces have plaque, the Plaque Free Score Index used to determine his or her biofilm-free score is 72% (ie, 72% of teeth are biofilm free and 28% are covered in plaque).
- A biofilm-free score of 85% or higher is considered to demonstrate adequate oral hygiene.
Using Disclosing Solution Throughout the Appointment
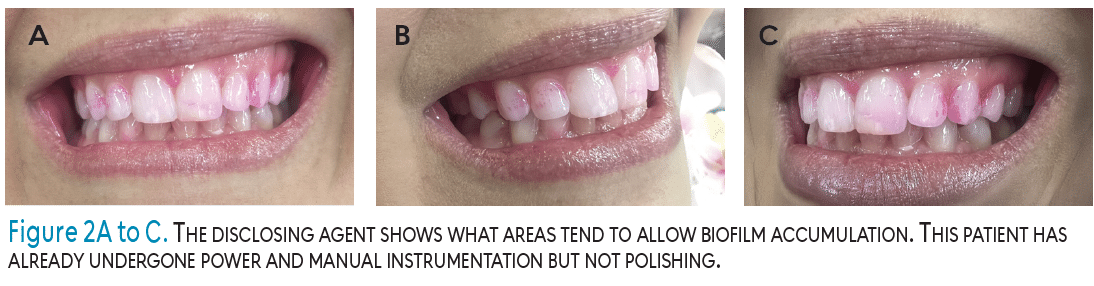
Applying a disclosing agent mid-appointment or post-prophylaxis provides the clinician with either confidence that the appointment is progressing appropriately or alerts the clinician to areas that need more attention. Figure 2A to C features a patient with disclosing solution after ultrasonic and manual instrumentation had been performed but before polishing. This provides the clinician with a guideline on what areas to emphasize. Patients should also be educated on those areas that tend to invite biofilm accumulation.
Conclusion
Recording patients’ biofilm-free scores in their charts and using them for comparison will demonstrate whether oral hygiene instructions are being followed correctly or done at all. Making disclosing solution part of hygiene appointments and collecting objective, quantifiable facts regarding patients self-care regimens help clinicians improve their gingival health and reduce their risk for periodontal diseases and dental caries.
Research shows that the use of engaging material in the learning process improves patients’ motivation to comply.12 Incorporating disclosing solution and biofilm-free scoring into daily practice can help enhance patient education, support the development of treatment plans, and monitor patients self-care.1,3
References
- Chawhuaveang DD, Yu OY, Yin IX, Lam WY, Mei ML, Chu CH. Acquired salivary pellicle and oral diseases: A literature review. J Dent Sci. 2021;16:523-529.
- Marsh PD. Dental plaque as a biofilm and a microbial community — implications for health and disease. BMC Oral Health. 2006;6(Suppl 1):S14.
- Boyd LD, Mallonee LF. Wilkins’ Clinical Practice of the Dental Hygienist. 14th ed. Burlington, Massachusetts: Jones & Bartlett Learning; 2024
- Frias J, Olle E, Alsina M. Periodontal pathogens produce quorum sensing signal molecules. Infect Immun. 2001;69:3431-3434.
- White DJ. Dental calculus: recent insights into occurrence, formation, prevention, removal and oral health effects of supragingival and subgingival deposits. Eur J Oral Sci. 1997;105(5 Pt 2):508-522.
- Fujikawa K, Sugai K, Suzuki K, Haruta K, Okada A, Murai S. A comparison of the effects of various plaque disclosing material on plaque accumulation. Journal of the Japanese Society of Periodontology. 1983;25(2):399-404.
- Volgenant CMC, Mostajo MFY, Rosema NAM, van der Weijden FA, Ten Cate JM, van der Veen MH. Comparison of red autofluorescing plaque and disclosed plaque—a cross-sectional study. Clin Oral Investig. 2016;20:2551-2558.
- Gardner J. Tell, show, do, apply: the anatomy of good instruction. Available at https://elearningindustry.com/tell-show-do-apply-the-anatomy-of-good-instruction. Accessed October 24, 2025.
- Ramfjord SP, Ash MM. Periodontology and Periodontics: Modern Theory and Practice. Philadelphia: WB Saunders Co; 1979:273.
- O’Leary TJ, Drake RB, Naylor JE. The plaque control record. J Periodontol. 1972;43:38.
- Grant DA, Stern IB, Everett FG. Periodontics. 5th ed. St.Louis: Mosby; 1979.
- Atlantic University. Show, Don’t Tell: What It Means to Be a Visual Learner. Available at https://bau.edu/blog/visual-learner. Accessed October 24, 2025.
From Dimensions of Dental Hygiene. November/December 2025; 23(6):26-27.
