
Building Inclusive, Affirming Care for LGBTQIA+ Patients
Understanding LGBTQIA+ terminology and identities is a foundational step for dental hygienists to reduce disparities, foster trust, and deliver respectful, patient-centered oral healthcare.
This course was published in the March/April 2026 issue and expires April 2029. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 558
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define common, appropriate terms used when referring to the lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual/aromantic/agender (LGBTQIA+) community.
- Identify oral conditions that commonly affect LGBTQIA+ patients.
- Discuss changes that can be made in the dental office to create an inclusive environment for LGBTQIA+ individuals.
Understanding terms that patients may use to identify themselves is an easy first step to improving patient care. Lesbian, gay, bisexual, transgender, queer/questioning, intersex, asexual/aromatic/agender (LGBTQIA+) — with the plus sign referring to any nonheterosexual/noncisgender identities that are not explicitly listed in previous terminology — is a frequently used acronym. These terms are not exhaustive as there are many nuances that continue to evolve as patients’ identities do. These terms serve as a foundation to build an understanding of LGBTQIA+ patients and their identities to facilitate respectful communications (Table 1).
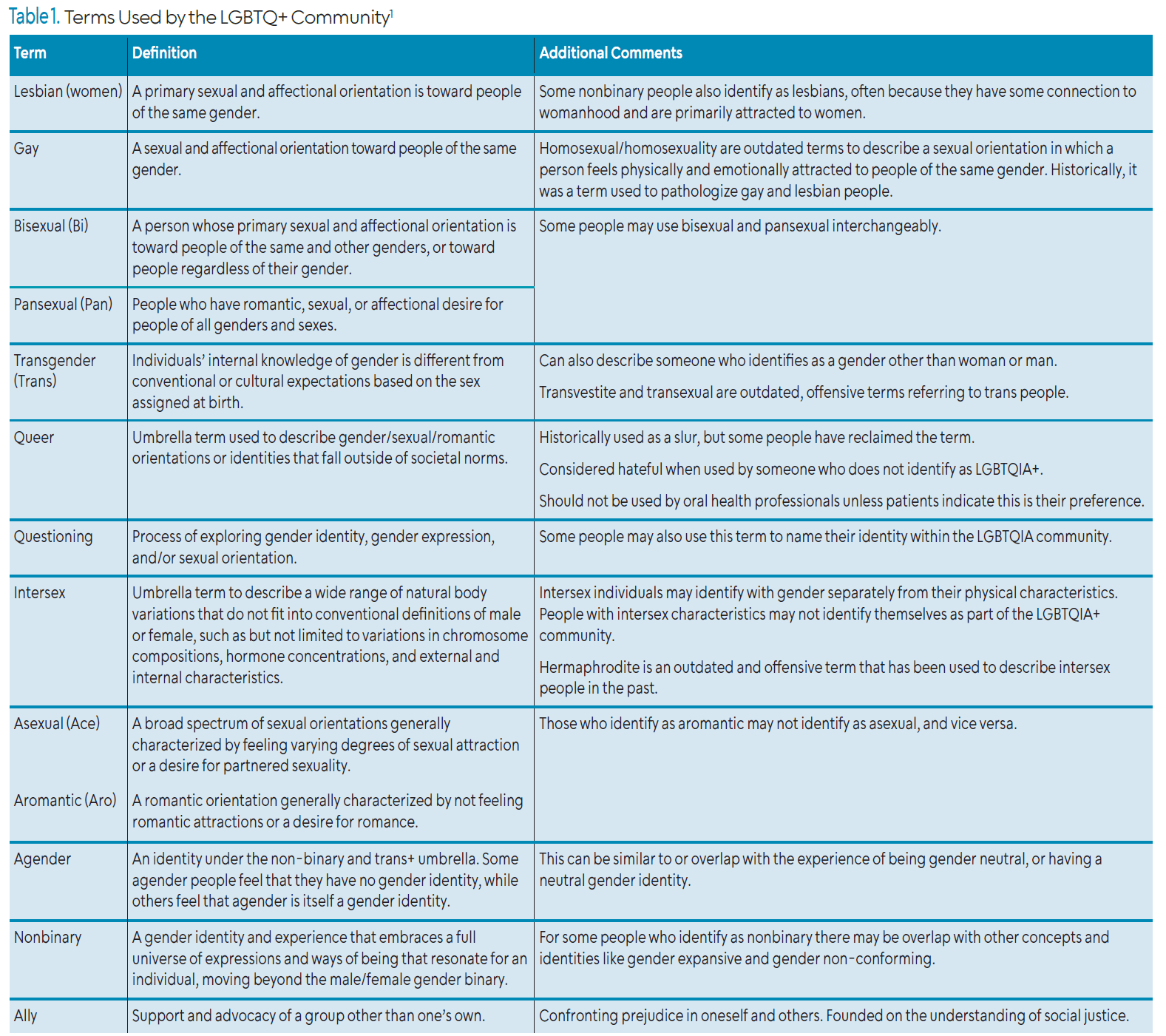
Sexual orientation, biological sex, gender identity, and gender expression are all spectrum-based components of LGBTQIA+ terminology. Sexual orientation describes sexual or romantic attraction to others.1 Terms used to describe sexual orientation include heterosexual, homosexual, gay, lesbian, bisexual, asexual, pansexual, etc.
Romantic attraction is the emotional connection with another person, while sexual attraction is the physical connection to or arousal from others.1 Terms used to describe romantic attraction include aromantic, heteroromantic, homoromantic, etc. Biological sex uses an individual’s chromosomes, gonads, hormones, and genitalia to medically categorize them. Furthermore, biological sex is nonbinary due to the variations in the possible characteristics used to determine categorization.2
Cisgender relates gender identity and sex assigned at birth as congruent. Intersex indicates that a person has a mix of male and female chromosomal, hormonal, internal, or external characteristics. Gender identity is how individuals sense their gender. Gender expression is how individuals present their gender.1 Terms used to express gender identity and expression include transgender (trans), agender, nonbinary, etc.
Members of the LGBTQIA+ community account for approximately 20 million people in the United States, yet studies indicate those that identify as LGBTQIA+ are likely to postpone or completely avoid seeking healthcare due to barriers such as anticipation of discrimination, misgendering, and costs.3-6 This highlights how widespread fears of discrimination or financial strain contribute to significant healthcare disparities within a segment of the population.
The diverse personal, social, and systemic experiences of gender- and sexuality-diverse individuals, along with documented inequities in access to health care,7,8 underscore the importance of oral health professionals developing the knowledge and skills needed to address patients’ unique needs and provide inclusive, effective treatment.
Oral health professionals have an ethical responsibility to provide adequate and respectful treatment to all patients, including diverse patient populations such as the LGBTQIA+ community. Dental hygienists specifically play an important role in building the relationship between dental practices and the community as the front line patient educators and preventive service providers.
One study found dental students were less likely than medical and nursing students to express interest in receiving formal LGBTQIA+ health education. Additionally, students across all programs reported feeling unprepared to treat members of the LGBTQIA+ community.9 Competence in inclusive and affirming care significantly improves LGBTQIA+ patients’ comfort with oral health professionals.10
Oral Considerations
When caring for LGBTQIA+ patients, psychosocial factors and individual systemic conditions must be considered. Recommendations should be personalized and delivered with sensitivity to each patient’s unique experiences. LGBTQIA+ populations experience distinct oral health needs resulting from unique social, behavioral, and systemic barriers compared to cisgender, heterosexual individuals. Elevated rates of tobacco, alcohol, and substance use within this community contribute to increased risks of xerostomia, dental caries, periodontal diseases, oral cancer, and bruxism.11,12 Dental hygienists play a critical role in identifying these behaviors, providing nonjudgmental cessation counseling, and connecting patients with resources to support healthier habits.
Although some quitlines emphasize inclusivity by explicitly inviting LGBTQIA+ individuals to seek support, few demonstrate this commitment through visible acknowledgment on their webpages.¹³ Consequently, dental hygienists serve as an essential, accessible resource for LGBTQIA+ patients by delivering evidence-based cessation counseling, ongoing support and referrals, and reinforcement of cessation messages to improve both oral and systemic health outcomes.
Beyond behavioral interventions, dental hygienists should evaluate patients for signs of bruxism, such as attrition or abfraction, and perform comprehensive caries risk assessments to tailor preventive and therapeutic strategies. Based on these findings, modifications may include the use of occlusal guards, professional fluoride applications, and at-home fluoride therapies. When appropriate, application of silver diamine fluoride offers a minimally invasive adjunctive therapy to arrest active carious lesions and manage high caries risk in patients who may face barriers to restorative care.¹⁴ Recommendations for saliva substitutes, dry mouth products, and individualized self-care aids can further address xerostomia, caries risk, and periodontal concerns for this population.
Among LGBTQIA+ populations, particularly men who have sex with men, higher rates of oral human papillomavirus (HPV) infection may contribute to an increased risk of oral cancer.15 Dental hygienists are already educating patients on risks and how to perform monthly oral cancer self-exams at home. Recommendations may include looking for persistent abnormalities like red, white, or mixed lesions and assessing areas such as the tongue’s lateral borders, tonsillar pillars, soft palate, and floor of the mouth. In addition, patients should be advised that if they see anything of concern, they should take clear photos of the area (documenting date, size, location, and appearance) and, if the abnormality does not resolve within 2 weeks, call the dental office promptly so the patient can be examined and referred to a specialist for definitive diagnosis.16 Promoting self-detection and prompt reporting of symptoms is critical to improving oral cancer outcomes in LGBTQIA+ individuals.
Engaging in nonjudgmental conversations about HPV vaccination is important when caring for LGBTQIA+ patients, especially adolescents, to help reduce HPV-associated oral cancers. HPV vaccines are approved for ages 9 to 45, with two or three doses depending on age, and earlier vaccination provides greater protection.17,18 Dental hygienists are well-positioned to discuss vaccination status and offer evidence-based guidance to promote oral cancer prevention and improve health outcomes.
Mental health conditions, such as anxiety, depression, and eating disorders, are other concerns to consider while treating the LGBTQIA+ community. Transgender individuals, in particular, face a heightened risk of mental health challenges often associated with increased rates of suicide and self-harm.19 Chronic mental health struggles experienced by LGBTQIA+ individuals may lead to neglected oral hygiene and further anxiety when seeking oral healthcare. Clinicians should carefully observe for clinical signs, such as swelling of the parotid glands and erosion on the lingual surfaces of maxillary teeth, as they can indicate eating disorders.20 When these signs are present, dental hygienists should advise patients who engage in purging behaviors to rinse with water or a baking soda solution and to delay brushing for at least 1 hour to allow saliva to restore pH balance to minimize enamel damage.21
Coordination with and referral to mental health professionals when eating disorders are suspected, in addition to tailored oral care plans, are essential to managing these patients effectively and preventing further oral deterioration.22
Practical Changes for Dental Settings
Dental hygienists, particularly those in managerial roles, can feature diverse images of LGBTQIA+ patients and families on social media platforms or practice websites as a nonverbal signal that the office is a safe and welcoming space. This approach helps to build rapport and create a positive impression as both are essential for providing comfortable, patient-centered care.23
Additional strategies to foster inclusivity include installing gender-neutral signage for single-stall restrooms and providing LGBTQIA+-inclusive books or magazines in waiting areas. Displaying visible indicators of support, such as Safe Space Alliance signage, at entrances, reception areas, waiting rooms, or operatories offers an accessible and effective way for dental hygienists and office managers to communicate safety and respect.
Dental hygienists can also participate in registries or services that help LGBTQIA+ patients locate safe and affirming providers. Wearing pins or other visual indicators signaling allyship serves as a nonverbal cue that providers are committed to patient safety and inclusion.23
Normalizing inclusive sexual and health history by asking pronouns, preferred name, and other open-ended questions allows patients to share based on their comfort levels or preferences. Consider training all staff to consistently use patients’ preferred names and pronouns.
Using neutral language and avoiding assumptions based on biases fosters respect and avoid microaggressions, which may decrease healthcare avoidance.24 Fostering an office culture of respect, accountability, and zero tolerance for discrimination can create a consistently LGBTQIA+-friendly environment.
Dental hygienists can encourage language such as “partner” instead of “husband” or “wife” and “parents” rather than “mom and dad” to be used in the office.25 Providing LGBTQIA+ inclusive educational materials and connecting patients to community resources can be included as part of patients’ routine oral hygiene education provided by dental hygienists.
Once a patient has shared pronouns and preferred name, the dental hygienist needs to document and adjust the electronic health record (EHR) to reflect the patient’s wishes. The adjustment in the EHR will further allow other health providers to address the patient respectfully, without forcing the patient to address each provider individually.26
Should the clinician misuse a name pronoun, or gendered term, the best approach is to recognize and own the error, correct the language, and proceed with the conversation utilizing the appropriate vocabulary.27 Drawing excessive attention to the error can increase patient discomfort or embarrassment. Avoid defensiveness when being corrected by LGBTQIA+ individuals and recognize it as an opportunity for growth.
Dental hygienists in educator roles may also be able to seek ally training through their institution to further enhance inclusivity in academic and clinical settings. Ally training can provide dental hygiene educators with specific, personalized, institution accepted ways to improve communications with those of the LGBTQIA+ community in their academic and clinical roles. Dental hygiene educators can also model inclusive language in the classroom to normalize practices with future providers. By modelling inclusive behaviors and fostering consistent institutional support for LGBTQIA+‑affirming communication, educators can help build a culture of respect that future dental providers may carry into practice.23
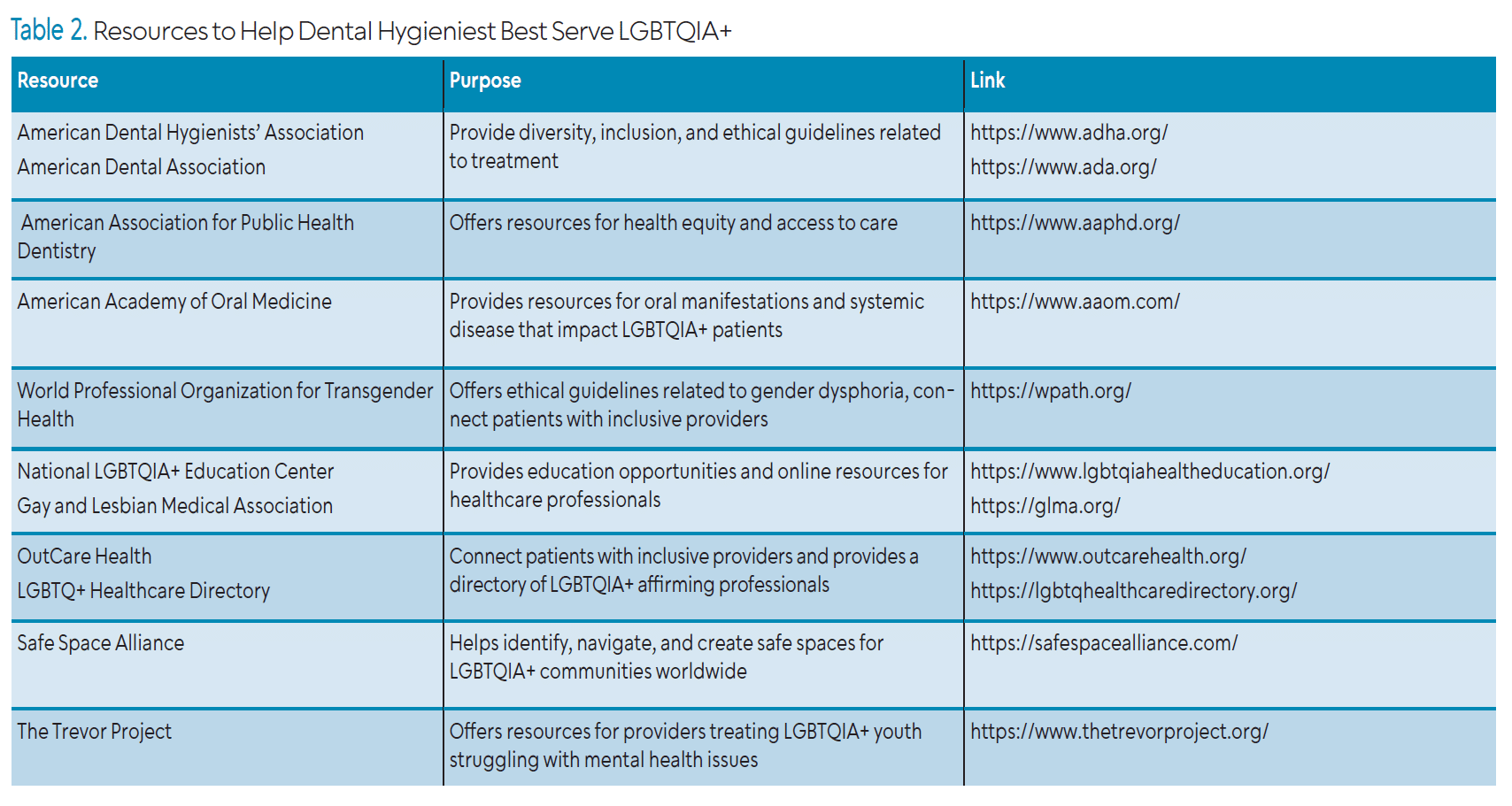
Many resources are available to aid dental hygienists in working with the LGBTQIA+ community (visit the web version of this article for a list). Dental hygienists may want to connect with local centers for community-specific resources and referral networks to best serve their patient populations.
![]() Conclusion
Conclusion
Providing equitable and respectful care is a core principle of the dental hygiene profession. Providing affirming care to LGBTQIA+ patients requires a foundational understanding of cultural competency, inclusive communication, and the unique oral considerations of these individuals.
References
- LGBTQIA Resource Center Glossary. LGBTQIA Resource Center. Available at https://lgbtqia.ucdavis.edu/educated/glossary. Accessed January 31, 2026.
- American Society for Reproductive Medicine. Just the Facts: Biological Sex. Available at asrm.org/advocacy-and-policy/fact-sheets-and-one-pagers/just-the-facts-biological-sex/. Accessed January 31, 2026.
- Stacey L. An updated data portrait of heterosexual, gay/lesbian, bisexual, and other sexual minorities in the United States. Soc Curr. 2024;11:383-400.
- Kcomt L, Gorey KM, Barrett BJ, McCabe SE. Healthcare avoidance due to anticipated discrimination among transgender people: A call to create trans-affirmative environments. SSM Popul Health. 2020;11:100608.
- Raisin JA, Keels MA, Roberts MW, Divaris K, Jain N, Adkins DW. Barriers to oral health care for transgender and gender nonbinary populations. J Am Dent Assoc. 2023;154:384-392.
- Gupta A, Salway T, Jessani A. Cost-related avoidance of oral health service utilization among lesbian, gay, and bisexual individuals in Canada. J Public Health Dent. 2023;83:254-264.
- Jessani A. Oral health equity for global LGBTQ+ communities: A call for urgent action. Int Dent J. 2025;75:17-19.
- Wickman J, Mukherjee S, Mintz A, Northridge JL. A social ecological approach to identifying barriers and proposing interventions at multiple levels to improve healthcare for LGBTQIA+ youths in the United States. J Adolesc Health. 2025;76:967-984.
- Greene MZ, France K, Kreider EF, et al. Comparing medical, dental, and nursing students’ preparedness to address lesbian, gay, bisexual, transgender, and queer health. PLoS One. 2018;13:e0204104.
- Tharp G, Wohlford M, Shukla A. Reviewing challenges in access to oral health services among the LGBTQ+ community in Indiana and Michigan: A cross-sectional, exploratory study. PLoS One. 2022;17e0264271.
- Boyd CJ, Veliz PT, Stephenson R, Hughes TL, McCabe SE. Severity of alcohol, tobacco, and drug use disorders among sexual minority individuals and their “not sure” counterparts. LGBT Health. 2019;6:15-22.
- Fakhrjahani I, Tiwari T, Jessani A. A scoping review of oral health outcomes and oral health service utilization of 2SLGBTQ+ people. JDR Clin Trans Res. 2024;9:199-211.
- Ramos-Santiago JW, McIntosh S, Orfin RH, et al. Do US quitsites present information related to providing services for LGBTQ individuals? An audit study. Tob Prev Cessat. 2024;10:191457.
- Santos NML, Tohara H, Rodrigues LKA, et al. The role of silver diamine fluoride as dental caries preventive and management: A systematic review. J Clin Med. 2024;13:4647.
- Sonawane K, Shyu SS, Damgacioglu H, Li R, Nyitray AG, Deshmukh AA. Prevalence and concordance of oral and genital HPV by sexual orientation among US men. JNCI Cancer Spectr. 2023;7:pkac088.
- Oral Cancer Foundation. Early Detection, Diagnosis, and Staging. Available at https://oralcancerfoundation.org/cdc/early-detection-diagnosis-staging. Accessed January 30, 2026.
- Wolf J, Kist LF, Pereira SB, et al. Human papillomavirus infection: Epidemiology, biology, host interactions, cancer development, prevention, and therapeutics. Rev Med Virol. 2024;34:e2537.
- Kamolratanakul S, Pitisuttithum P. Human papillomavirus vaccine efficacy and effectiveness against cancer. Vaccines (Basel). 2021;9(12):1413. doi:10.3390/vaccines9121413
- Ziegler E, Valaitis R, Carter N, Risdon C, Yost J. Primary care for transgender individuals: A review of the literature reflecting a Canadian perspective. SAGE Open. 2020;10:1-14.
- Valeriani L, Frigerio F, Piciocchi C, et al. Oro-dental manifestations of eating disorders: A systematic review. J Eat Disord. 2024;12:87.
- Rangé H, Colon P, Godart N, Kapila Y, Bouchard P. Eating disorders through the periodontal lens. Periodontol 2000. 2021;87:17-31.
- Presskreischer R, Prado MA, Kuraner SE, Arusilor IM, Pike K. Eating disorders and oral health: A scoping review. J Eat Disord. 2023;11:55.
- Braybrook D, Bristowe K, Timmins L, et al. Communication about sexual orientation and gender between clinicians, LGBT+ people facing serious illness and their significant others: A qualitative interview study of experiences, preferences and recommendations. BMJ Qual Saf. 2023;32:109-120.
- Marchi M, Travascio A, Uberti D, et al. Microaggression toward LGBTIQ people and implications for mental health: A systematic review. Int J Soc Psychiatry. 2024;70:23-35.
- National LGBTQIA+ Health Education Center. Providing Inclusive Services and Care for LGBT People: A Guide for Health Care Staff. Available at lgbtqiahealtheducation.org/publication/learning-guide/. Accessed January 30, 2026.
- Grutman AJ. Use of chosen names in electronic health records to promote transgender inclusivity. J Am Med Inform Assoc. 2023;30:1219-1221.
- Okamuro K, Card A, Barton HJ, et al. Patient and clinician perspectives on misgendering in healthcare. BMJ Qual Saf. 2025:bmjqs-2024-018364.
From Dimensions of Dental Hygiene. March/April 2026;24(2):36-39
