Evolution of Caries Diagnosis
New technologies can improve the sensitivity of visual methods of caries detection, and help identify lesions in their earliest stages.
This course was published in the Septemeber 2011 issue and expires September 2014. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- List the three components of dental caries diagnosis.
- Discuss evidence-based tools for identifying the presence of lesions and determining their status.
- Explain the technologies available to aid in dental caries detection.
- Detail the process of carious lesion assessment.
A greater understanding of dental caries has led to a paradigm shift in its management. Traditionally, surgical intervention was viewed as the initial course of treatment, but evidence now indicates that prevention is a more effective first step.1 Because caries is most effectively treated when caught early, an accurate diagnosis is essential. Clinicians cannot rely on visual clues alone to aid in caries diagnosis because many are not initially apparent.2 As the caries process continues, symptoms—such as pain and sensitivity to cold, hot, or sweet substances—develop. The mere presence of symptoms without additional information, however, is not indicative of an active, ongoing caries process. Accurate dental caries diagnosis depends on three components: caries risk assessment, detection of carious lesions, and lesion activity assessment.1 These components should be used to determine the best treatment approach.1,3
DIAGNOSTIC PROCESS
Because early lesions are in a dynamic stage of activity (progressing or remineralizing) or inactivity (arrested), much uncertainty exists in the early stages of dental caries.2 However, the best predictor of future caries is past caries experience.1,4 Identifying the presence of lesions and determining whether they are remineralizing or demineralizing are essential to accurate caries diagnosis.5-9
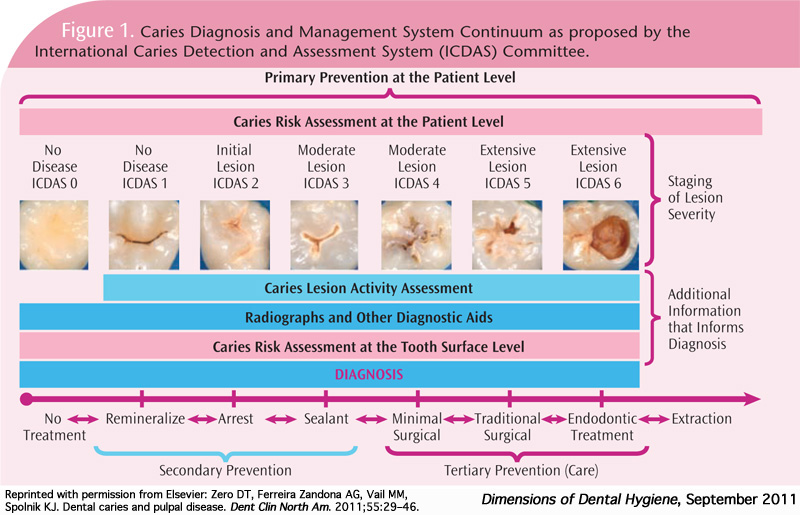
Systems that can support this new paradigm in dental caries management have garnered significant interest. The International Caries Detection and Assessment System (ICDAS) and the Caries Classification System are evidence-based tools that assess the severity of dental caries.7,9-11 They are based on direct visual examination of clean tooth surfaces. The ICDAS has seven categories (0-6) for every tooth surface (Figure 1). Early and advanced enamel carious lesions make up a significant portion of these criteria (categories 1-4). However, in order for these changes to be visible, tooth surfaces must be plaque-free and they must be examined both wet and dry.
The initial stages of an early lesion may not be detected by conventional methods (visual examination or radiography). Despite the difficulty in visually identifying early signs of dental caries, the presence of caries risk factors may indicate a risk of future caries development and thus requires the use of primary preventive interventions, such as topical fluoride and preventive sealants.1 As the process progresses, the initial signs of the disease are identifiable within seconds of the surface being dried (ICDAS 1). These early lesions (incipient or white spot lesions) can be more clearly seen when dried because they are more porous than sound enamel. When the enamel is dried, the water that fills the voids is replaced by air. Due to the difference in refractive indexes of air and water, the lesion is revealed as a white spot.12 If a tooth was examined under a microscope, these lesions would appear limited to the outer half of the enamel (Figure 2).13
As the caries process evolves, the lesions involve the entire thickness of the enamel, sometimes affecting the outer surface of the dentin (ICDAS 2).13 These changes are more distinct, making them visible even when the surface is wet or covered in saliva (Figure 2). At this stage, the dentin-pulp complex responds by increasing the activity of odontoblasts, which deposit a tertiary dentin matrix (reactionary dentin). The underlying dentin may start to acquire a brown tint.
With further progression, the continuity of the enamel is compromised and micro-cavitations are formed (Figure 2). Bacteria can then invade the dentin expeditiously. However, nonsurgical treatment is still feasible.1 The lesion then spreads along the dermal-epidermal junction and destroys the dentino-enamel, resulting in less support for the overlying enamel.14 When the enamel surface collapses, dentin is exposed (ICDAS 5 and 6), and the cavitation fills with food debris, saliva, and bacteria (Figure 2).14 The bacteria then come in direct contact with the dentin, demineralize the dentin, and expose the extracellular matrix, which are successively degraded by matrix metalloproteinases found in the saliva and the dentin itself.15,16 At this stage, pulpal involvement is certain.
DIFFICULTY OF DIAGNOSIS
Diagnosis of carious lesions can be a subjective process. Under- or over-diagnosis provide negative outcomes—the former resulting in additional tooth destruction,1 and the latter leading to unnecessary restorative treatment.17 However, progression of dental caries is slow, and in cases of uncertainty, delaying surgical intervention in favor of prevention is in the best interest of patients.
 Visual examination alone is highly specific (ie, effective at determining whether surfaces are sound), but lacks sensitivity (ie, not very effective at detecting early stage lesions on surfaces) when surfaces have a lesion, especially in the early stages. Bitewing radio graphs improve sensitivity of detection on proximal surfaces.18 Because the X-ray beam must pass through the whole tooth, it will only detect a carious lesion when at least one-third to one-half of the hard tissue is affected. Thus, only more advanced lesions (ICDAS 2-6 on proximal surface and ICDAS scores 4-6 on occlusal surfaces) are detected on radiographs (Figure 2).14 Early carious lesions do not provide enough contrast to be clearly visible on radiographs.19 Consequently, several new technologies have been developed to aid in the detection and diagnosis of dental caries.7
Visual examination alone is highly specific (ie, effective at determining whether surfaces are sound), but lacks sensitivity (ie, not very effective at detecting early stage lesions on surfaces) when surfaces have a lesion, especially in the early stages. Bitewing radio graphs improve sensitivity of detection on proximal surfaces.18 Because the X-ray beam must pass through the whole tooth, it will only detect a carious lesion when at least one-third to one-half of the hard tissue is affected. Thus, only more advanced lesions (ICDAS 2-6 on proximal surface and ICDAS scores 4-6 on occlusal surfaces) are detected on radiographs (Figure 2).14 Early carious lesions do not provide enough contrast to be clearly visible on radiographs.19 Consequently, several new technologies have been developed to aid in the detection and diagnosis of dental caries.7
NEW TECHNOLOGIES
New methods of caries detection and diagnosis are especially suitable for the detection of early- to moderate-stage lesions (ICDAS 1-4). Figure 2 illustrates the ability of each method to detect lesions on occlusal and proximal surfaces.
Because demineralization changes the optical properties of enamel, several of these new methods are based on optical properties. Most use some form of light—from the blue-green region to near-infrared region of the light spectrum. Some measure reflectance (amount of light that is reflected by the tooth surface in relation to the amount of incident light), while others measure a combination of luminescence (the level of glow) and heat generated after a laser light is shone on a tooth. Additional tools note differences in light transmission. Several technologies measure differences in fluorescence, which is a type of luminescence. One option uses electrical impedance to determine the health of the tooth.
Varying degrees of evidence are available to support the use of these technologies.3,7,20 The methods based on fluorescence in the blue range are highly sensitive and can detect the majority of very early lesions; however, this sensitivity can lead to an increased rate of false positives.21 Combining this approach with a visual method might be a viable clinical alternative.22 Fluorescence in the infrared range has greater sensitivity for more severe lesions (ICDAS 2-4),23 but it is not as effective in diagnosing caries around restorations.24
The tools that use reflectance detect changes in reflectance from sound enamel to demineralized enamel. Limited data are available showing that they can detect very early lesions (ICDAS 2-4), but they may offer advantages that include minimal dilution of the light signal (because light is sent and captured in a direct line) and its insensitivity to the presence of bacteria.25
Another technology analyzes luminescence (glow) and the thermal behavior (heat) captured from the tooth. The system has a good performance record for detection of enamel caries on occlusal surfaces.26
Methods that use transmission of light through the tooth structures perform similarly to bitewing radiographs in the detection of approximal and occlusal caries when lesions extend into dentin (ICDAS 3-4).27These methods place a light on one surface and observe the area from a different surface. For example, a light is placed below the contact point on the interproximal surface from the buccal or lingual aspect and the tooth is then observed from the occlusal surface.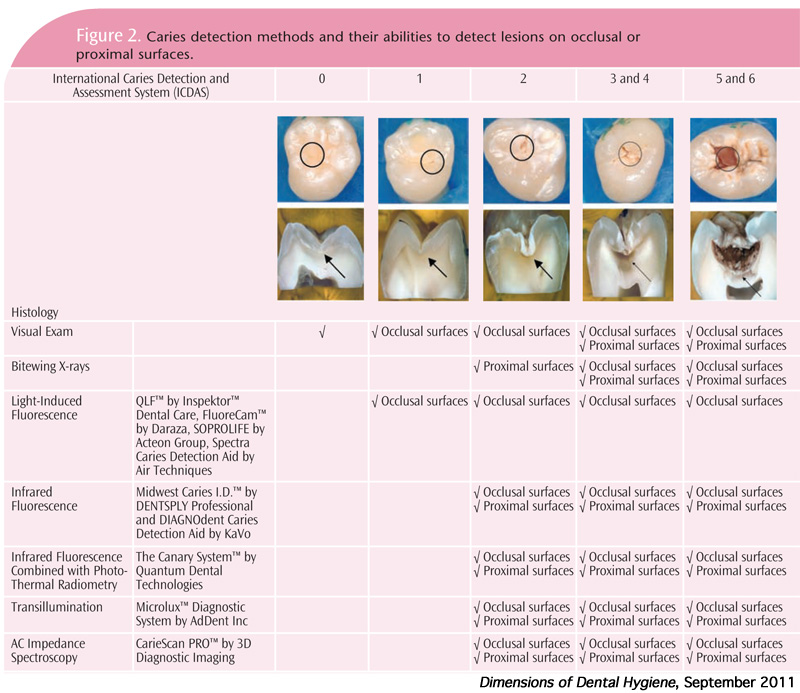
Another method uses electrical impedance that looks at electrical resistance or lack of resistance. It is able to detect lesions on approximal surfaces and occlusal surfaces,28 but limited data are available on the effectiveness of this device.29 Other technologies, such as optical coherence tomography, show promise but are not yet commercially available.30
All of these devices can be used to aid in the diagnosis of dental caries.7 They have the potential to improve the sensitivity of visual methods of detecting early lesions and assist in the diagnosis of questionable surfaces.
ACTIVITY ASSESSMENT
Once a lesion has been detected, the activity status of the lesion must be assessed. Activity assessment criteria have been proposed.11,31 Limited data indicate that the systems are feasible and likely able to predict the activity of lesions.3,11,31 Both of these assessments are based on severity of the lesions and characteristics of the surface such as color, location in plaque stagnation area, surface texture,31and hardness.11 Once a lesion is detected and its activity is assessed, the information is compiled with the caries risk assessment to achieve the best treatment decision for the patient.1
If a patient has several risk factors (eg, highly cariogenic diet, lack of saliva, lack of exposure to fluoride), even in the absence of clinically detectable lesions, the patient may still face a moderate or high caries risk. Carious lesions are dynamic and early lesions are not easily visualized. A patient with active lesions should be assessed minimally as moderate risk of future caries development or progression.1
CONCLUSION
In the best possible scenario, patients at high risk of developing lesions would be recognized before the caries process even begins. However, at this time none of the caries risk assessment tools have sufficient accuracy to identify patients who will develop new lesions.32 The best predictor of caries is past caries history.1,4 Thus, all patients should receive primary prevention, oral hygiene instructions, dietary advice, and recommendations to use fluoridated dentifrice twice per day.1 Nonetheless, identification of early lesions is a requisite for managing patients with secondary preventive measures (topical fluorides and sealants) instead of resorting to surgical intervention.
REFERENCES
- Zero DT, Ferreira Zandona AG, Macapagal Vail M, Spolnik KJ. Dental caries and pulpal disease. Dent Clinics of North Amer. 2011;55:29-46.
- Nyvad B. Diagnosis versus detection of caries. Caries Res. 2004;38:192-198.
- Braga MM, Ekstrand KR, Martignon S, Imparato JC, Ricketts DN, Mendes FM. Clinical performance of two visual scoring systems in detecting and assessing activity status of occlusal caries in primary teeth. Caries Res. 2010;44:300-308.
- Disney JA, Graves RC, Stamm JW, et al. The University of North Carolina Caries Risk Assessment study: further developments in caries risk prediction. Community Dent Oral Epidemiol. 1992;20:64-75.
- Nyvad B, Fejerskov O. Assessing the stage of caries lesion activity on the basis of clinical and microbiological examination. Community Dent Oral Epidemiol. 1997;25:69-75.
- Zero DT. Dental caries process. Dent Clin North Am. 1999;43:635-664.
- Ferreira Zandona A, Zero DT. Diagnostic tools for early caries detection. J Am Dent Assoc. 2006;137:1675-1684.
- Ekstrand KR, Zero DT, Martignon S, et al. Lesion activity assessment. Monogr Oral Sci. 2009;21:63-90.
- Pitts NB. Modern concepts of caries measurement. J Dent Res. 2004;83:C43-C47.
- Ismail AI, Sohn W, Tellez M, et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol. 2007;35:170-178.
- Nyvad B, Machiulskiene V, Baelum V Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res. 1999;33:252-260.
- Kidd EAM, Fejerskov O. What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J Dent Res. 2004;83:C35-C38.
- Ekstrand KR, Ricketts DN, Kidd EA. Reproducibility and accuracy of three methods for assessment of demineralization depth on the occlusal surface: an in vitro examination. Caries Res. 1997;31:224-231.
- Ekstrand KR, Ricketts DN, Kidd EA. Occlusal caries: pathology, diagnosis and logical management. Dent Update. 2001;28:380-387.
- Tjaderhane L, Larjava H, Sorsa T, et al. The activation and function of host matrix metalloproteinases in dentin matrix breakdown in caries lesions. J Dent Res. 1998;77:1622-1629.
- Chaussain-Miller C, Fioretti F, Goldberg M, et al. The role of matrix metalloproteinases (MMPs) in human caries. J Dent Res. 2006;85:22-32.
- Elderton RJ. Clinical studies concerning restoration of tooth. Adv Dent Res. 1990;4:4-9.
- Dove B. Radiographic diagnosis of dental caries. J Dent Educ. 2001;65:985-990.
- Ko A, Hewko M, Sowa M, et al. Early Dental Caries Detection using Fibre-optic coupled Polarization-resolved Raman spectroscope system. Optic Expres. 2008;16:6274-6284.
- Pretty IA. Caries detection and diagnosis: novel technologies. J Dent. 2006;34:727-739.
- Ferreira Zandoná AG, Analoui M, Beiswanger BB, et al. An in vitro comparison between laser fluorescence and visual examination for detection of demineralization in occlusal pits and fissures. Caries Res. 1998;32:210-218.
- Ferreira Zandona AG, Santiago E, Eckert G, et al. The Use of ICDAS combined with QLF as a caries detection method. Caries Res. 2010;44:317-322.
- Costa AM, Paula LM, Bezerra AC. Use of Diagnodent for diagnosis of non-cavitated occlusal dentin caries. J Applied Oral Sci. 2008;16:18-23.
- Bamzahim M, Aljehani A, Shi XQ. Clinical performance of DIAGNOdent in the detection of secondary carious lesions. Acta Odontol Scand. 2005;63:26-30.
- Amaechi B. Emerging technologies for diagnosis of dental caries: the road so far. J Appl Phys. 2009;105:102047.
- Jeon RJ, Hellen A, Matvienko A, et al. In vitro detection and quantification of enamel and root caries using infrared photothermal radiometry and modulated luminescence. J Biomed Optics. 2008;13:034025-034011.
- Chesters RK, Pitts NB, Matuliene G, et al. An abbreviated caries clinical trial design validated over 24 months. J Dent Res. 2002;81:637-640.
- Huysmans MC, Longbottom C, Pitts NB, et al. Impedance spectroscopy of teeth with and without approximal caries lesions– an in vitro study. J Dent Res. 1996;75:1871-1878.
- Longbottom C, Hall AF, Czajczynska-Waszkiewicz A, et al. Caries detection by optimal clinical visual, radiographic, laser fluorescence and ac impedance spectroscopy techniques. Caries Res. 2007;41:297.
- Louie T, Lee C, Hsu D, et al. Clinical assessment of early tooth demineralization using polarization sensitive optical coherence tomography. Lasers Surg Med. 2010;42:738-745.
- Ekstrand KR, Martignon S, Ricketts DJ, Qvist V. Detection and activity assessment of primary coronal caries lesions: a methodologic study. Oper Dent. 2007;32:225-235.
- Hausen H, Kärkkäinen S, Seppä L. Application of the high-risk strategy to control dental caries. Community Dent Oral Epidemiol. 2000;28:26-34.
From Dimensions of Dental Hygiene. September 2011; 9(9): 84-87.
