
Radiography
Timing, technique, and behavior management are essential to producing high-quality radiographs with pediatric patients.
Radiology and pediatrics are two of the nine specialties in dentistry. Combining the two brings up an interesting subject—dental radiography and children! Working with children in the dental setting can be frustrating and exasperating. However, putting kids on the path to good oral health is rewarding in itself. One of the daily challenges in working with children is producing high quality diagnostic radiographs.
In most states, the dentist is responsible for deciding on the number, type, and frequency of dental radiographs. Since every patient’s dental condition is different, a radiographic examination should be prescribed based on the needs of the individual, never on a predetermined number of radiographs or set time interval between radiographs. The foundation of
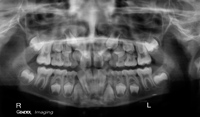
an accurate diagnosis and treatment plan is based on a comprehensive medical and dental history, a thorough clinical examination, and diagnostic radiographs.1 Although obtaining radiographs can be exceedingly difficult in the pediatric population, radiographs are a vital part of children’s dental records and without them, certain dental conditions will surely be overlooked or missed. For example, a panoramic radiograph is a good diagnostic tool to illustrate the mixed dentition of a child, ensuring that all permanent teeth are developing properly (Figure 1).
TIMING
Prescribing radiographs not only depends on the needs of the child but also on his or her age, size of the oral cavity, and willingness to cooperate. Although no exact age exists for the first radiographs to be exposed, somewhere between 5 and 6 years old is a common starting point. The child who has experienced unusual circumstances, such as an early trauma, early childhood caries, or a cleft lip or palate, may require radiographs at an earlier age. If a thorough clinical examination finds the posterior contacts open and interproximal surfaces are easily examined, radiographs may not be necessary at that point in time.2
EXPOSURE
In general, children need radiographic examinations more frequently than adults. Changes occur rapidly as the structures in the oral cavity grow.2 Compared to adults, children are usually more prone to decay.2 It is important to survey the primary teeth as well as account for all unerupted permanent teeth. Along with monitoring growth and development, radiographs also help diagnose diseases of the bone, types of trauma, and aid in planning future orthodontic treatment. The American Academy of Pediatric Dentistry recommends a radiographic examination every 6 months for children with a high risk of tooth decay.3 The frequency of radiographs depends on the child’s risk for developing caries, which is increased by the lack of fluoridated water, a history of tooth decay or poor oral hygiene, and high sugar intake.
Patient protection in diagnostic radiography should be the primary goal of a radiographic examination. The guidelines for prescribing dental radiographs are available at the American Academy of Pediatric Dentistry’s website: www.aapd.org/pdf/radiograph.pdf. Please note that these recommendations are subject to clinical judgment and may not apply to every patient. All patients—children, adolescents, or adults—should be evaluated for dental radiographs on an individual basis.4
SAFETY
Dental professionals should be careful to minimize the exposure of patients to unnecessary radiation. Although children are more sensitive to the effects of radiation than adults, the risk is negligible in a dental radiographic examination when proper protective techniques are employed. Some radiation safeguards include: using digital radiography (or a film with high speed for conventional radiography), placing lead aprons and thyroid collars, using long-cone paralleling technique, and following federal and state regulations on proper filtration and collimation of the x-ray beam.3,4 These steps ensure that the child receives a minimal amount of radiation exposure.
TECHNIQUE
The techniques used to expose intraoral radiographs in pediatric patients are basically identical to those used in adults. Bitewings, periapical films, occlusal projections, and panoramic radiographs are all useful and give valuable diagnostic information. The film size used should be determined by the size of the child’s mouth rather than a specific age.5
With the younger child, beginning a radiographic examination with the most comfortable projection, usually the anterior occlusal view, is helpful.6 Occlusal views are often used in place of periapical radiographs since the small mouth size of a child may limit correct film placement. Occlusal projections are beneficial due to their visualization of a greater area of teeth and supporting structures on one film. Occlusal radiographs may reveal common findings, such as the proper location of developing permanent teeth, or dental anomalies, such as cleft areas, impactions, or jaw expansion. Children bite their teeth lightly together with the white side of the film facing the arch to be radiographed. Size 2 film can be used for the occlusal projections.
Bitewing radiographs determine the presence of interproximal caries if the proximal surfaces cannot be visualized clinically. Size 0 or 1 film may be used for younger children. If the child continues to struggle with an intraoral film, the reverse bitewing should be considered.7 In this method, the film is not placed inside the mouth but rather into the buccal sulcus on the side being radiographed. The child bites on the tab to hold the film in place beneath his or her cheek. The x-ray beam is directed from underneath the opposite side of the mandible, much like an extraoral film, with the beam aimed at the bitewing. An advantage of this technique is that the reverse bitewing may be the only way to visualize interproximal regions of the uncooperative child. However, disadvantages include increased exposure times (due to greater target- to-film distance) and poor diagnostic quality of the image.
A common type of initial radiographic examination is a four film series that includes two posterior bitewings and an occlusal projection of each arch.2 As children get older and their mouths become larger and more accommodating, an 8 film series may be indicated.
BEHAVIOR
Exposing radiographs can create concern and apprehension for children. The dental professional can calm the anxious child in a number of ways. Managing children requires confidence, patience, and understanding. Various strategies for behavior management have been well documented over time.2,3,4,6,8,9 Some common behavior procedures that can be applied to dental radiography include:
1. Use simple instructions. The “tell/ show/do” approach can be very helpful. Tell the child what to expect and briefly explain the procedure. Follow with a demonstration, perhaps on a doll or another person. Then perform the procedure on the child. Seeing an older sibling or parent demonstrate holding an intraoral film between his or her teeth may calm an anxious child.
2. Desensitize the child. Explain procedures and talk to your patient in words that are easy to comprehend. The x-ray tubehead can be referred to as a camera that takes a picture of the teeth. Let the child touch and hold a film, and place it in his or her own mouth. 1
3. Use positive reinforcement. Children should receive praise and encouragement, especially when the behavior has been acceptable. Non-verbal signs, such as smiling, nodding your head, or cheerful facial expressions, are appreciated when they are keeping their mouths wide open or holding very still.
4. Create a distraction. There may be moments during a dental visit that are not pleasant. Draw the child’s attention away from the task-at-hand by telling a story, humming a song, or giving positive feedback. Distraction can help in producing diagnostic radiographs in children with a gag reflex. Instruct them to focus on an object in the room, breathe through their nose, or keep one foot in the air until the exposure button has beeped.
5. Maintain a supportive office environment. Children are more apt to cooperate during all dental procedures if the entire staff shows support. This can be accomplished by smiling, talking to the child, and establishing good rapport. Early positive experiences influence children in seeking dental health care throughout the rest of their life.10
Other behavior techniques have also been used in the past including, hand-over-mouth, voice control, and physical restraints such as papoose boards. With time, these disciplinary forms of behavior management have lost acceptance in society.8 If a child’s behavior precludes obtaining radiographs of adequate diagnostic quality, this type of examination should be postponed until the behavior can be managed or improves.
REFERENCES
- Schwartz S. Radiographic techniques for the pediatric patient. J Contemp Dent Pract. 2000;1:60-73.
- McDonald RE. Radiographic techniques. In: McDonald RE, Avery DR, Dean JA, et al, eds. Dentistry for the Child and Adolescent. 8th ed. St Louis: Mosby Inc; 2004:60-69.
- American Academy of Pediatric Dentistry. Prescribing dental radiographs. Available at: www.aapd.org/media/policies.asp. Accessed January 11, 2005.
- Haring JI, Jansen L. Radiation protection. In: Haring JI, Jansen L, eds. Dental Radiography: Principles and Techniques, Second Edition. Philadelphia: W.B. Saunders Co; 2000:63-75.
- LePeau NS. Pediatric oral health care. In Wilkins EM, eds. Clinical Practice of the Dental Hygienist. 9th ed. Baltimore: Lippincott, Williams & Wilkins; 2005:782-802.
- Pinkham JR. Examination, diagnosis, and treatment planning: the primary dentition years 3-6. In: Pinkham JR, Fields HW Jr, McTigue DJ, Casamassino PS, Nowak A, eds. Pediatric Dentistry: Infancy Through Adolescence. 3rd ed. Philadelphia: W.B. Saunders Co; 1999:272-275.
- Frommer HH. Patient management and special problems. In: Frommer HH. Radiology for Dental Auxiliaries. 7th ed. St Louis: Mosby Inc; 2001:286-311.
- Law CS, Blain S. Approaching the pediatric dental patient: a review of nonpharmacologic behavior management strategies. J Calif Dent Assoc. 2003;31:703-713.
- Pinkham JR. Behavior management of children in the dental office. Dent Clin North Am. 2000;44:471-486.
- Kaakko T, Riedy CA, Nakai Y, Domoto P, Weinstein P, Milgrom P. Taking bitewing radiographs in preschoolers using behavior management techniques. ASDC J Dent Child. 1999;66:320-324.
