Understanding and Managing Periapical Lesions
Retrograde peri-implantitis presents a rare but challenging complication in implant dentistry. Learn about its potential causes, diagnostic methods, and treatment strategies, including the role of growth factors like rh-PDGF in promoting successful bone regeneration.
Periapical lesions or radiolucencies around implants pose a unique challenge to the dental team. Retrograde peri-implantitis (RPI) is defined as a clinically symptomatic periapical lesion that develops after implant placement and maintains normal bone-to-implant contact at the coronal aspect.1,2 The prevalence of RPI is generally very low. A retrospective study of 1,651 implants over 20 years noted a prevalence of RPI of 0.34%.3
 While there is no consensus about the etiology of RPI, several factors have been proposed, including bacterial contamination of the implant surface and surgical site, thermal osteonecrosis, over-extension of the implant bed, pre-existing bone diseases, presence of foreign bodies or root fragments, and endodontic complications of adjacent teeth.4-6
While there is no consensus about the etiology of RPI, several factors have been proposed, including bacterial contamination of the implant surface and surgical site, thermal osteonecrosis, over-extension of the implant bed, pre-existing bone diseases, presence of foreign bodies or root fragments, and endodontic complications of adjacent teeth.4-6
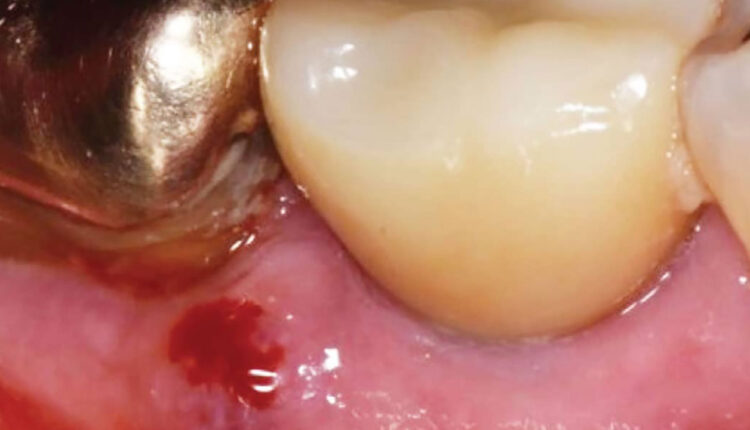
The diagnosis of RPI is made both clinically and radiographically. Reiser and Nevins7 first classified these lesions as either inactive (not infected) or active (infected). Inactive lesions present without clinical signs and symptoms. They often decrease in size and are usually attributed to an over-extension of the implant osteotomy. Active lesions, however, increase in size and are associated with swelling, pain, erythema, and/or fistula formation.7
 There is no singular treatment for RPI, as it largely depends on its clinical and radiographic presentation.8 Inactive lesions are usually monitored with radiographs, assuming they do not expand. Although proper self-care and regular maintenance are critical to implant success, they do not directly affect the incidence of RPI because its pathogenesis is related to the implant apex.
There is no singular treatment for RPI, as it largely depends on its clinical and radiographic presentation.8 Inactive lesions are usually monitored with radiographs, assuming they do not expand. Although proper self-care and regular maintenance are critical to implant success, they do not directly affect the incidence of RPI because its pathogenesis is related to the implant apex.
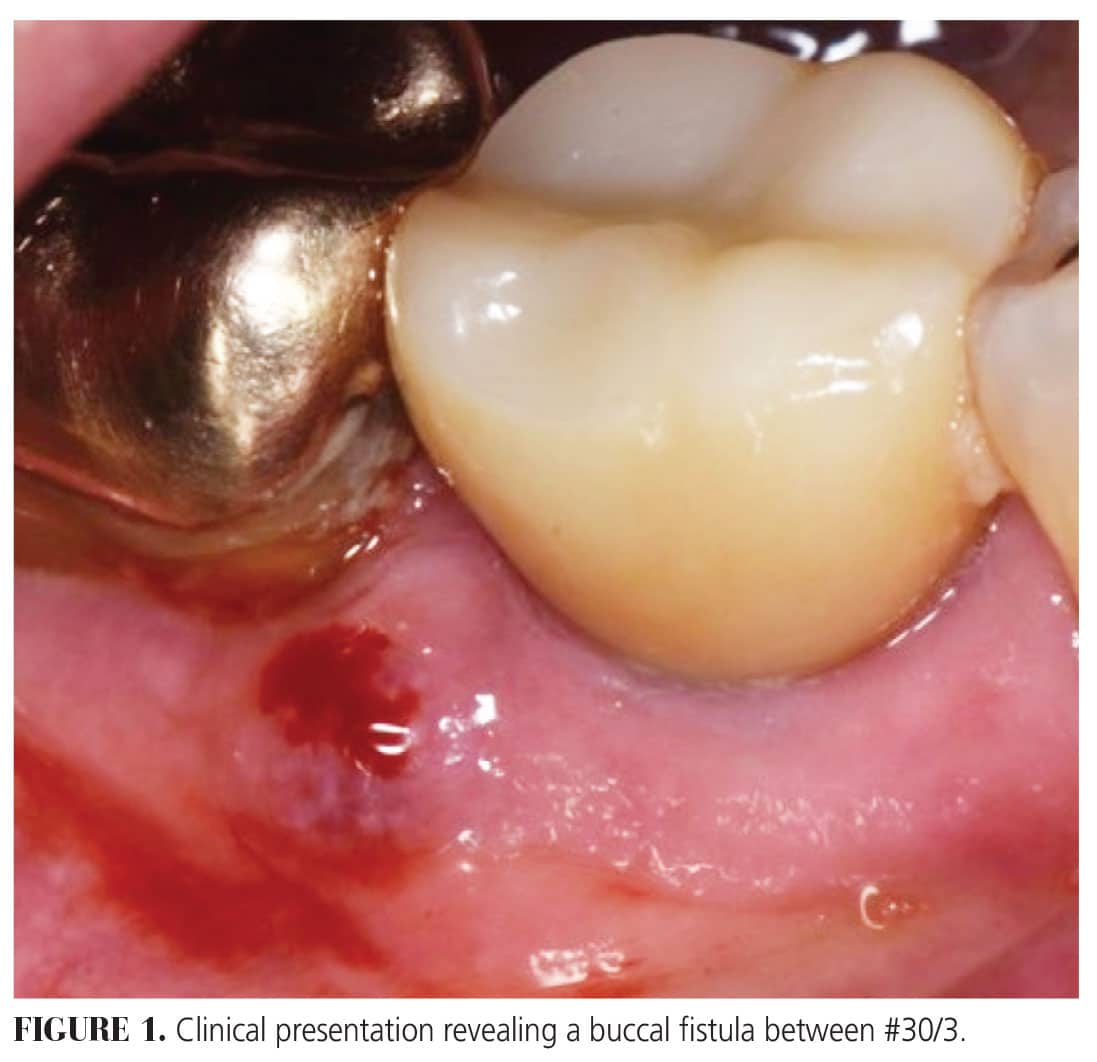
Active lesions require surgical intervention to prevent further osseous breakdown and to mitigate patient symptoms. This can include implant removal and replacement, implant flap debridement, or regenerative therapy using a bone graft, membrane, and/or growth factor. Some protocols also include resection of the implant apex for complete disinfection.8
The use of growth factors has revolutionized oral regeneration around teeth and implants. These natural biological mediators regulate crucial cellular events involved in tissue repair and even enhance the development of lamellar bone in the craniofacial complex.9 One of the best-documented growth factors is recombinant human platelet-derived growth factor (rh-PDGF) and it is derived from human platelet cells following tissue injury.10 Obtained with recombinant DNA processing, rh-PDGF upregulates angiogenesis and promotes guided bone regeneration in large horizontal ridge defects. Its main effect is mitogenesis and chemotaxis for cells of mesenchymal origin, increasing the potential for regeneration.10,11
 In 2005, the United States Food and Drug Administration approved purified rh-PDGF with an osteoconductive matrix, tricalcium phosphate (β-TCP).
In 2005, the United States Food and Drug Administration approved purified rh-PDGF with an osteoconductive matrix, tricalcium phosphate (β-TCP).
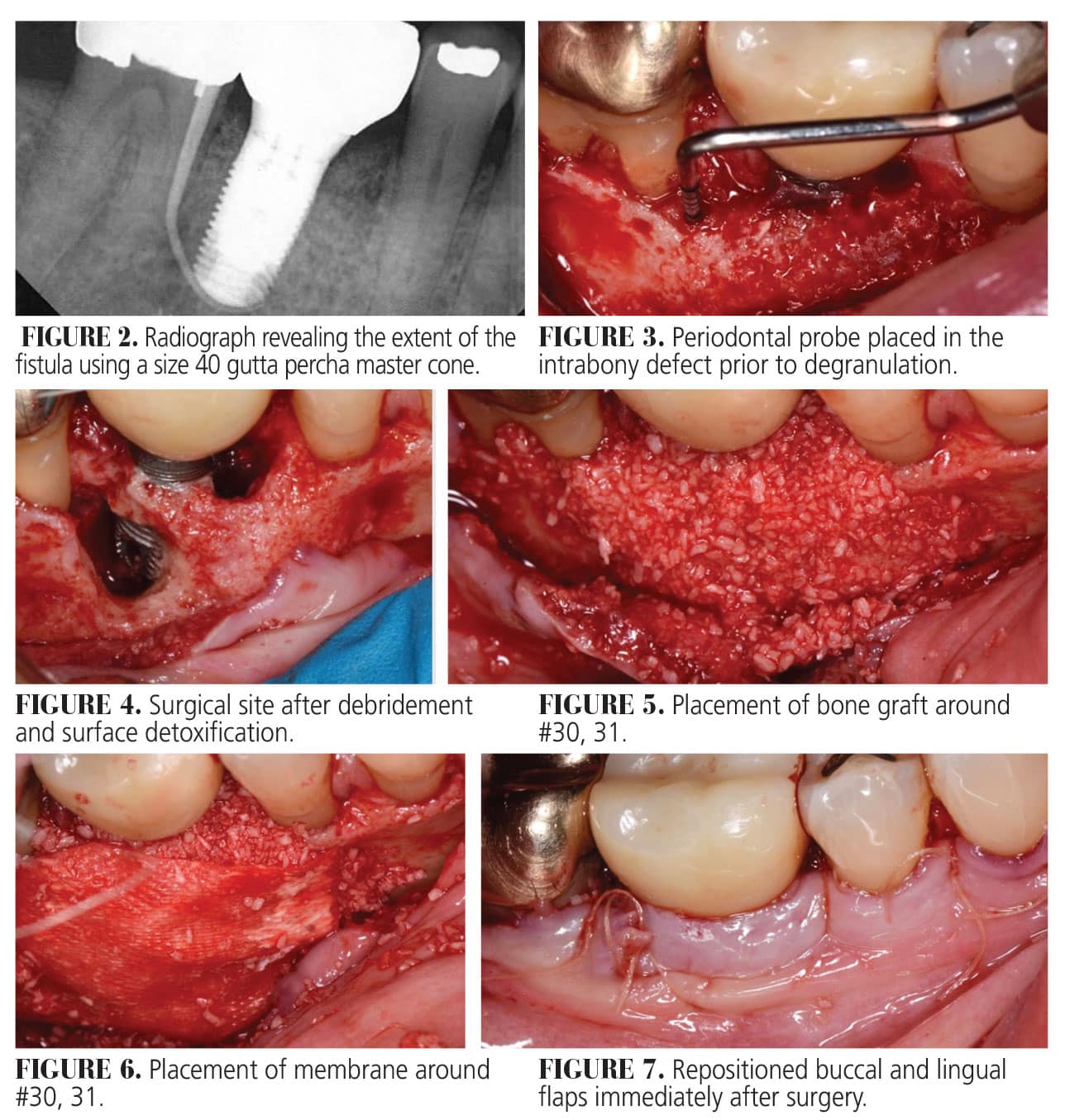
A recent systematic review that assessed the clinical efficacy, benefits, and safety of rh-PDGF in hard and soft tissue regeneration reported that the combined use of bone graft substitutes, namely xenografts and allografts, successfully achieved root coverage, ridge augmentation, and/or ridge preservation.11 Bone substitutes act as an osteoconductive, three-dimensional matrix, or scaffold enhanced by the chemotactic, mitogenic, and angiogenic properties of rh-PDGF, leading to improved wound healing, osteogenesis, and defect resolution.11
References
- Quirynen M, Gijbels F, Jacobs R. An infected jawbone site compromising successful osseointegration. Periodontol 2000. 2003;33:129-144.
- Wiedemann TG. A clinical approach to treatment of retrograde peri-implantitis. Compend Contin Educ Dent. 2021;42:170-175.
- Di Murro B, Canullo L, Pompa G, Di Murro C, Papi P. Prevalence and treatment of retrograde peri-implantitis: A retrospective cohort study covering a 20-year period. Clin Oral Investig. 2021;25:4553-4561.
- Zhou W, Han C, Li D, Li Y, Song Y, Zhao Y. Endodontic treatment of teeth induces retrograde peri-implantitis. Clin Oral Implants Res. 2009;20:1326-1332.
- Temmerman A, Lefever D, Teughels W, Balshi TJ, Balshi SF, Quirynen M. Etiology and treatment of periapical lesions around dental implants. Periodontol 2000. 2014;66:247-254.
- Penarrocha-Oltra D, Blaya-Tarraga JA, Menendez-Nieto I, Penarrocha-Diago M, Penarrocha-Diago M. Factors associated with early apical peri-implantitis: A retrospective study covering a 20-year period. Int J Oral Implantol (Berl). 2020;13:65-73.
- Reiser GM, Nevins M. The implant periapical lesion: etiology, prevention, and treatment. Compend Contin Educ Dent. 1995;16:768–772.
- Burdurlu MC, Dagasan VC, Tunc O, Guler N. Retrograde peri-implantitis: evaluation and treatment protocols of a rare lesion. Quintessence Int. 2021;52:112-121.
- Donos N, Dereka X, Calciolari E. The use of bioactive factors to enhance bone regeneration: A narrative review. J Clin Periodontol. 2019;46 Suppl 21:124-161.
- Yao W, Shah B, Chan HL, Wang HL, Lin GH. Bone quality and quantity alterations after socket augmentation with rhpdgf-bb or bmps: a systematic review. Int J Oral Maxillofac Implants. 2018;33:1255-1265.
- Tavelli L, Ravida A, Barootchi S, Chambrone L, Giannobile WV. Recombinant human platelet-derived growth factor: a systematic review of clinical findings in oral regenerative procedures. JDR Clin Trans Res. 2021;6:161-173.
This information originally appeared in Boeriu S, Hottel TL, Saltz AE, et al. A novel approach to treating retrograde peri-implantitis. Decisions in Dentistry. 2024;10(3):36-1.
