The Impact of Burnished Calculus on Periodontal Health
Burnished calculus poses a significant risk to periodontal health by creating a breeding ground for inflammation and infection.
Removal of burnished calculus is challenging yet extremely important to create root surfaces that are biologically compatible with the periodontium and to reduce inflammation. Endoscopy has shown that calculus is strongly associated with inflammation in the pocket wall.1,2 Subsequently, the incomplete removal of calculus leaves a niche for irritants to promote inflammation, contributing to reinfection and disease recurrence.3 Burnished calculus is the smoothing of deposits by instrumentation, creating a hard and dense structure. Burnishing is inadvertent and results from inadequate instrumentation due to technique and time.
Assessment
Bleeding on probing is a key indicator of burnished calculus.4 Inflammation adjacent to burnished deposits is not easily determined. In fact, gingiva often appears pink, taut, and fibrotic. Therefore, the gingiva should be assessed with periodontal probing for bleeding points, pocket depth, and clinical attachment level. Radiographs are important also to evaluate root topography and bone loss.
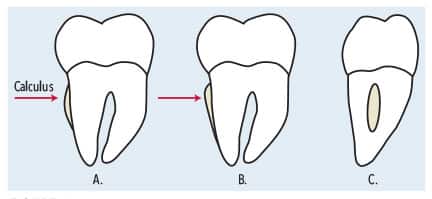
Exploring the root surface and not feeling normal root anatomy nor an apical and coronal border of a deposit are other ways to identify burnished calculus (Figure 1). Compressed air aids in detection by evaluating root surfaces near the cementoenamel junction and in the periodontal pocket, should the gingiva be inflamed.
References
- Wilson TG, Carnio J, Schenk R, Myers G. Absence of histologic signs of chronic inflammation following closed subgingival scaling and root planing using the dental endoscope: human biopsies — a pilot study. J Periodontol. 2008;79:2036-2041.
- Wilson TG, Harrel SK, Nunn ME, Francis B, Webb K. The relationship between the presence of tooth-borne subgingival deposits and inflammation found with a dental endoscope. J Periodontol. 2008;79:2029–35.
- Cobb CM, Sottosanti JS. A reevaluation of scaling and root planing. J Periodontol. 2021:92:1370-1378.
- Checchi L, Montvecchi M, Checchi V, Zappulla F. The relationship between bleeding on probing and subgingival deposits. an endoscopical evaluation. Open Dent J. 2009;3:154-160.
This information originally appeared in Hodges KO. Removing burnished calculus. Dimensions of Dental Hygiene. 2023;21(8):18-21.
