Polishing Esthetic Restorative Materials
The successful maintenance of esthetic restorations.
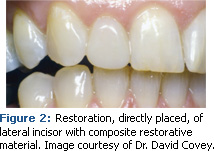
With the explosion of consumer demand for whiter, brighter smiles, dental hygienists need to be well versed in the dental materials used by esthetic dentistry in order to successfully maintain the surface integrity of esthetic restorations. Many esthetic dental materials are so advanced they are almost undetectable clinically (see Figures 1 and 2).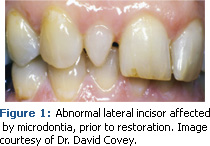
Dental materials undergo polishing procedures on a routine basis in dental hygiene practice, even with the practice of selective polishing.1-4,5 Dental hygienists cannot ignore the unique polishing requirements of esthetic materials and use the same polishing pastes that are used on the teeth, regardless of grit size.1,2,5,6 Unfortunately, esthetic restorative materials are not exempt from the practice of using coarse grit polishing paste to remove heavy stain.5
A basic understanding of the materials used for these artfully created restorations is necessary for their successful maintenance. The three basic materials used for esthetic restorations are porcelain, composites, and glass-ionomer cements.
PORCELAIN
 Porcelain has the most natural appearance of all restorative materials and is used for crowns and veneers. This material has the greatest translucency of all restorative materials because it transmits as much light as enamel. Porcelain is also the hardest esthetic restorative material. However, porcelain has a very brittle nature and is subject to fracture and roughness, which can cause excessive wear on opposing natural tooth structure. When porcelain is used for crowns, it can be applied over metal to increase the strength of the crown but the porcelain fused to the metal can still be subject to fracture. Porcelain can be glazed or polished. Porcelain restorations are glazed in the dental laboratory. Unglazed porcelain is typically found when the restoration has required adjustment during placement. When the occlusal surface or margins require adjustment, the glaze may be unavoidably removed. Unglazed porcelain can be polished and made as smooth as the glazed porcelain to the extent that they are difficult to distinguish from each other. Unglazed porcelain will stain much more readily than glazed or polished porcelain.
Porcelain has the most natural appearance of all restorative materials and is used for crowns and veneers. This material has the greatest translucency of all restorative materials because it transmits as much light as enamel. Porcelain is also the hardest esthetic restorative material. However, porcelain has a very brittle nature and is subject to fracture and roughness, which can cause excessive wear on opposing natural tooth structure. When porcelain is used for crowns, it can be applied over metal to increase the strength of the crown but the porcelain fused to the metal can still be subject to fracture. Porcelain can be glazed or polished. Porcelain restorations are glazed in the dental laboratory. Unglazed porcelain is typically found when the restoration has required adjustment during placement. When the occlusal surface or margins require adjustment, the glaze may be unavoidably removed. Unglazed porcelain can be polished and made as smooth as the glazed porcelain to the extent that they are difficult to distinguish from each other. Unglazed porcelain will stain much more readily than glazed or polished porcelain.
 <H3COMPOSITES
<H3COMPOSITES
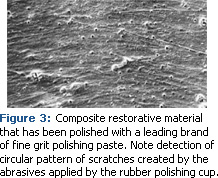
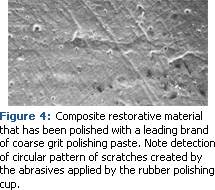
Composites are the most widely used esthetic restorative materials and are made of three structural components: a matrix, which is a plastic resin material (bis-GMA) for binding the filler particles; filler particles, such as glass, silica, quartz, or resin and/or short fibers; and a silane coupling agent that promotes binding of the fillers and the resin matrix. There are several types of composite materials, most of which are classified by the size and/or type of filler particle such as microfilled, hybrid, and macrofilled composites. Table 1 contains the various types of composites and their particle size and hardness number. Most composite restorations have a lower Mohs hardness number than enamel, making them more susceptible to prophylaxis polishing pastes, which can contain abrasives 10 times harder than the composite material.1-3,5 Prophylaxis polishing pastes increase the surface roughness of hybrid, microhybrid, and microfilled resin composite materials to the extent that the rough surface can retain bacteria. Figures 3 and 4 are scanning electron microphotographs that demonstrate the effect of a common commercially prepared prophylaxis polishing paste.7 The scratches of both the fine and coarse grits of this paste are so profound that the circular application with the rubber cup is visible. The roughness created by the paste causes the esthetic restoration to readily retain stain and become severely compromised.
GLASS-IONOMER CEMENTS
Glass-ionomer cements are not as widely used as composites.8 Glass-ionomer cements are tooth-colored so they are more esthetically pleasing than metallic restorations. However, glass-ionomers have few properties in common with composite materials. While both composites and glass-ionomer cements are used for Class V restorations and other anterior and posterior restorations, glass-ionomers do not have comparable shade matching. They also do not have the strength or wear resistance found in composite resins, making the material useful for temporary and intermediate restorations.M9
The glass filler particles in glass-ionomer cements have a Mohs hardness number range of 1-4.5.10 Glass-ionomer cement restorations are more opaque, more brittle, and have a rougher surface than composite resin restorations.11 Glass-ionomer cements are made of a calcium strontium aluminosilicate glass powder (base) combined with a water-soluble polymer (acid).8,9,11 Glass-ionomer cements also contain fluoride ions and can be useful for patients with high caries rates, however, the fluoride levels that are released are not consistent.9 After initial placement of the glass-ionomer cement restoration, there is a large burst of fluoride caused by the high concentration of fluoride ions in the matrix; thereafter, the fluoride is released at a much lower rate.9
FINISHING AND POLISHING
One of the most important aspects of polishing esthetic restorations is to note the distinction between “finishing and polishing” and “polishing.” Finishing and polishing refers to the removal of marginal irregularities, the definition of anatomic contours, and the smoothing away any surface roughness.12 Figure 5 provides examples of the types of finishers and polishers used in the process. The polishing procedure further enhances the restoration by removing scratches from the surface to produce a very smooth, light-reflecting luster. Finishing and polishing procedures are typically performed in three to four distinct steps.12,13 Finishing and polishing are critical to the esthetics of tooth-colored restorations and can have a substantial effect on their biocompatibility with tissues, longevity, and overall long-term clinical success.3,14,15
POLISHING
Polishing refers to the maintenance of the surface characterization of esthetic restorations, recreating a surface luster with smaller and smaller scratches during surface abrasion so that the smallest scratches are smaller than the wavelength of visible light, which is less than 0.5?m.11 The polishing of esthetic restorative materials incorporates both two-body and three-body abrasion.4 In two-body abrasive polishing the bound particles are solidly fixed to a substrate, for example, a rubber finisher embedded with diamond particles. Three-body abrasion, in which loose abrasives (the polishing paste abrasive particles) move in the interface space between the surface being polished and the polishing application device, is used more frequently than two-body abrasion. An example of three-body abrasion is the use of a polishing paste and a rubber polishing cup.
The polishing of esthetic restorative materials encompasses the following considerations:12
1. The structure and mechanical properties of the esthetic restorative material.
2. The hardness of the esthetic restorative material.
3. The hardness of the prophylaxis polishing paste abrasive or other polishing medium.
4. The physical properties of the material used to carry and apply the prophylaxis polishing paste or other polishing medium. This can vary from a paste to an abrasive-embedded prophylaxis cup or an abrasive-embedded polishing disc with various shapes (flame-shaped, conical, round, or diamond finishers).
Polishing esthetic restorative materials should also be based on the patient’s needs just as it is for polishing natural teeth. However, the process should be based on the manufacturers’ recommendations for their particular type and brand of esthetic restorative material. Oral prophylaxis polishing pastes were developed for polishing enamel only.2,4,5
POLISHING PORCELAIN
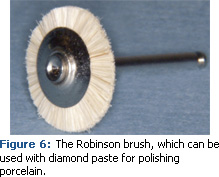 1. Glazed or polished porcelain. Porcelain restorations can stain in the same manner as tooth enamel. However, glazed and polished porcelain are much more stain resistant than unglazed porcelain. Unless given different instructions by the dentist, porcelain can be polished with a diamond paste (the diamond paste should be used dry) with a Robinson brush (see Figure 6).16 Some diamond polishing pastes come in three grit sizes: coarse, medium, and fine. The use of each of these grits should follow the manufacturers’ directions, but if coarse grit is required, it should be followed by the use of medium grit and finished with the fine grit. Each grit should be applied with a separate applicator to achieve the smoothest surface and highest luster. Some rubber polishing instruments will remove stain and create a highly polished surface all in one step. Rubber polishing instruments can also be followed with a diamond paste if necessary. Some rubber polishing finishers and polishers in porcelain polishing kits are embedded with diamond abrasives.16
1. Glazed or polished porcelain. Porcelain restorations can stain in the same manner as tooth enamel. However, glazed and polished porcelain are much more stain resistant than unglazed porcelain. Unless given different instructions by the dentist, porcelain can be polished with a diamond paste (the diamond paste should be used dry) with a Robinson brush (see Figure 6).16 Some diamond polishing pastes come in three grit sizes: coarse, medium, and fine. The use of each of these grits should follow the manufacturers’ directions, but if coarse grit is required, it should be followed by the use of medium grit and finished with the fine grit. Each grit should be applied with a separate applicator to achieve the smoothest surface and highest luster. Some rubber polishing instruments will remove stain and create a highly polished surface all in one step. Rubber polishing instruments can also be followed with a diamond paste if necessary. Some rubber polishing finishers and polishers in porcelain polishing kits are embedded with diamond abrasives.16
2. Unglazed porcelain. If unglazed porcelain is rough when felt with an explorer, it should be smoothed prior to polishing. A smooth, polished surface can be restored to unglazed porcelain with diamond paste (used dry).16 The diamond paste should be applied with a felt wheel or Robinson brush, as a regular rubber polishing cup and diamond paste will not produce the same result.16 However, if only stain is present, a rubber polishing cup and diamond paste can be very effective.
3. Porcelain-cement interface. Especially on less than perfect margins of bonded porcelain restorations, the resin cement used for luting (sealing) may become stained. Resin cements used as luting agents readily absorb stain.16 Great attention should be paid to polishing the resin cement interface because it is softer than the porcelain. If too much resin cement is removed during polishing, ditching at the margin can occur, which can leave the patient susceptible to leaking margins, plaque retention, and dental caries. The resin cement should be polished in the same manner as an esthetic composite restoration.16 The resin cement used should be polished with the procedure recommended by the manufacturer of the resin composite. Additionally, several polishing paste products are available that are safe and effective for resin cements. If no stain is present and only plaque needs to be removed, a cleaning agent containing feldspar can be used with a rubber polishing cup.4
POLISHING COMPOSITES
Most composite restorative material manufacturers have a polishing product recommended for use on their composite material. If those are not available, the products manufactured specifically for use on esthetic restorative materials can be used. A cleaning agent will remove dental plaque and not scratch composites, however, it will not polish or remove stain on an esthetic composite restoration.4
Dental hygienists should be able to identify the difference between small particle composites, hybrid composites, and microfilled composites. Small particle composites are fairly obsolete, however, older patients may still have some small particle composites. They are rougher than the hybrid or microfilled composites (when an explorer is drawn across the surface it will create a black line).16 A highly polished surface may not be possible to achieve on a small particle composite, therefore, rubber finishers and rubber polishers can be used, followed by a composite polishing paste.
Microfilled composites can be polished very quickly with a rubber polisher. Again, this can be followed by the use of a composite polishing paste, either the type recommended by the manufacturer of the composite or the type specifically manufactured for dental hygienists. Hybrid composites are harder to polish than microfilled composites. Hybrid composites should be polished with an aluminum oxide polishing paste recommended for composite restorations. The aluminum oxide paste should be applied with a rubber polishing cup that has been filled with water. If the restoration becomes dry during the procedure, water should be used to remoisten it.16 An extra-fine aluminum oxide paste should be used as the final polish for a hybrid composite. Finally, a cleaning agent can be used on any type of esthetic composite restorative material since it cleans but does not scratch.4
POLISHING GLASS-IONOMERS
Glass-ionomers typically have a rougher surface than esthetic composite materials, however, they should be polished using a light pressure and a slow speed.16 If a polishing product indicated for use on glass-ionomers does not remove stain, a fine finishing disc or rubber polisher can be used. Glass-ionomer restorations desiccate, which can lead to cracking and premature deterioration of the restoration, and should be lubricated with a petroleum jelly or water prior to polishing.16 Glass-ionomers will never have the shiny, smooth nondetectable surface than can be achieved with a polished esthetic composite restoration.
ADDITIONAL CONSIDERATIONS
Both manual and powered instrumentation around restorations should help produce and preserve the surface characterization of all restorations. The goal is to create the smoothest surfaces possible for teeth and restorative materials without inflicting damage or jeopardizing the marginal integrity of cemented castings. In particular, powered instrumentation with ultrasonic scalers can damage composite restorations (hybrid and microfilled), glass ionomers, laminate veneers, and titanium implant abutments. Ultrasonic instrumentation can also alter the margins of amalgam restorations and fracture porcelain.17 The tips of scalers should never be directed into the spaces where enamel and the restorative material abut.
Patients must also be provided with oral selfcare instructions.5 Patients must be instructed to use the least abrasive toothpaste because individual esthetic materials will respond uniquely to the abrasive particles in toothpaste.18 The hardness of esthetic restorative materials rivals the hardness of cementum and dentin, not enamel.4 On the other hand, the hardness of abrasive agents used in toothpastes are hundreds of times harder than natural tooth structures4 and even more so than esthetic restorative materials.
SUMMARY
When esthetic dental restorations are encountered during charting, they should be included in the treatment plan for the specific polishing procedures that are required. If the brand and type of esthetic restoration are known through the patient chart, the polishing procedures and products used should be those recommended by the manufacturer. If not possible, alternative polishing procedures should be used. A cleaning agent containing feldspar and rubber polishing cup can be used on all esthetic restorative materials with no chance of damage to the surface characterization.
The principles for polishing esthetic restorations are the same as for natural teeth. If the polishing agent used has more than one size grit polish the coarsest grit polish should be used first, followed by each successively smaller grit polish. During polishing, mixing larger abrasive particles with smaller particles will not produce the desired shiny surface because the particle sizes will mix. Each size grit must be applied separately. Therefore, to prevent each grit size from being contaminated with the previous size grit, the rubber cup or applicator must be replaced between applications. During the polishing procedure, the polishing paste should be frequently renewed in the polishing cup because the paste may dry as the binders are expressed during use, which will make the paste more abrasive.
Keeping esthetic restorative materials looking like they were just placed is a service highly valued by patients and is another reason to emphasize why dental hygiene appointments are so important.
REFERENCES
- Neme AL, Wagner WC, Pink FE, Frazier KB. The effect of prophylactic polishing pastes and toothbrushing on the surface roughness of resin composite materials in vitro. Oper Dent. 2003;28:808-815.
- Barnes, CM, Covey DA, Walker MP, Johnson WW. Essential selective polishing: the maintenance of aesthetic restorations. Journal of Practical Hygiene. 2003;12:18-24.
- Neme AL, Frazier KB, Roeder LB, Debner TL. Effect of prophylactic polishing protocols on the surface roughness of esthetic restorative materials. Oper Dent. 2002;27:50-58.
- Barnes CM. The science of polishing. Dimensions of Dental Hygiene. 2009; 7(11):18-22.
- Barnes CM. Care and maintenance of esthetic restorations. Journal of Practical Hygiene. 2004;14:19-22.
- Barbakow F, Lutz F, Imfeld T. Relative dentin abrasion by dentifrices and prophylaxis pastes: implications for clinicians, manufacturers and patients. Quintessence Int. 1987;18:29-34.
- Strategic Data Marketing. Available at: www.sdmdata.com. Accessed October 21, 2009.
- Saito S, Tosaki S, Hirota K. Characteristic of glass-ionomer cements. In: Davidson CL, Mjör IA. Advances in Glass-Ionomer Cements. Chicago: Quintessence Publishing Co Inc; 1999:15.
- Roberson TH, Heymann HO, Swift EJ. Sturdevant’s Art and Science of Operative Dentistry. St. Louis: Mosby; 2003:218-219, 502-593.
- United States Patent Number 4,695,251. Orthodontic bracket adhesive and abrasive for removal thereof. Available at: www.freepatentsonline.com. Accessed December 1, 2009.
- Gladwin M, Bagby M. Clinical Aspects of Dental Materials, Theory, Practice and Cases. Baltimore: Lippincott, Williams & Wilkins; 2004:65-77, 209, 268.
- Jeffries SR. Abrasive finishing and polishing in restorative dentistry: a state-of-the-art review. Dent Clin N Am. 2007;51:379-397.
- Yap AU, Lye KW, Sau CW. Surface characteristics of tooth-colored restoratives polished utilizing different polishing systems. Oper Dent. 1997;22:260-265.
- Goldstein RE. Finishing of composites and laminates. Dent Clin N Am. 1989;33:305-318.
- Goldstein RE, Garber DA. Maintaining esthetic restorations—a shared responsibility. J Esth Dent. 1995;7:187.
- Miller MB, ed. REALITY The Techniques, Volume I. Houston, Tex: REALITY Publishing Co; 2003:604-605.
- Hodsdon KA. Postoperative care for esthetic restorations: a challenge to dental hygienists. Journal of Practical Hygiene. 1998;7:19-24.
- Tanoue N, Matsumura H, Atsuta M. Wear and surface roughness of current prosthetic composites after toothbrush/dentifrice abrasion. J Prosthetic Dent. 2000;84:93-97.
- O’Brien WJ. Dental Materials and Their Selection, 3rd ed., 2002, pp. 113-116, Chicago, Quintessence Publishing Co.
- Sarrett DC, K.-J.M. Soderholm K-J.M. , Batich CD. Water and Abrasive Effects on Three-body Wear of Composites. J Dent Res 70(7):1074-1081, July, 1991.
- Al-Haik Marwan S, Trinkle S,Yang F. Investigation of the nonmechanical and tri biological properties of dental materials. Int J Theoretical and Applied Multiscale Mechanics, 2009 1(1) 1-15.
- Farracane JL. Materials in Dentistry Principles and Applications. 2nd ed., 2001, p.88-110; 293-308, Baltimore, Lippincott, Williams & Wilkins.
From Dimensions of Dental Hygiene. January 2010; 8(1): 24, 26-28.
