
How Dental Teams Can Close the Gap in Transgender Oral Health
As the transgender population grows, oral health professionals play a critical role in reducing disparities by delivering informed, affirming, and clinically responsive care.
This course was published in the July/August 2026 issue and expires August 2029. The author has no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
AGD Subject Code: 750
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Define transgender population terminology.
- Discuss how to provide affirming dental hygiene care.
- Identify strategies to ensuring dental practices are a safe and inclusive environment.
As of February 2025, the transgender population makes up roughly 2.3 million or 1% of the United States population.1 As this population grows, oral health professionals are responsible for fostering respectful, affirming, and culturally competent care, which, ultimately, may lead to higher treatment adherence and overall better oral health outcomes.2,3
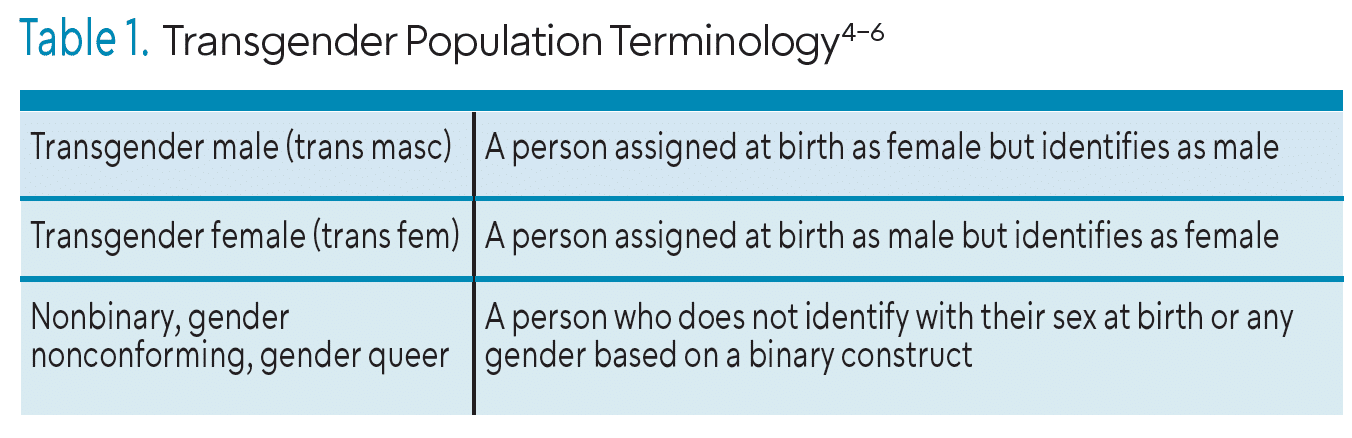
Transgender is an umbrella term for those who do not identify with their sex assigned at birth but rather choose their own gender identity. Gender identity refers to people’s individual feelings of gender and how they choose to identify and/or express those feelings. The transgender community includes trans men, trans women, nonbinary, gender nonconforming, and gender queer. Trans men (or trans masc) refer to those who were assigned as female at birth but identify as male. Trans women (or trans femme) refer to those assigned at birth as male but identify as female.4 Table 1 provides definitions.4-6
 Transitioning can happen at any stage of life but often begins in childhood with feelings of gender dysphoria. The American Psychological Association defines gender dysphoria as the “psychological distress that results from an incongruence between one’s sex assigned at birth and one’s gender identity.”5 Individuals seeking gender affirmation can choose several ways to transition such as social, legal, medical, or surgical.
Transitioning can happen at any stage of life but often begins in childhood with feelings of gender dysphoria. The American Psychological Association defines gender dysphoria as the “psychological distress that results from an incongruence between one’s sex assigned at birth and one’s gender identity.”5 Individuals seeking gender affirmation can choose several ways to transition such as social, legal, medical, or surgical.
Social transitioning may include changing one’s name, pronouns, or the type of clothing/hairstyles they present with.5 For example, changing their name given at birth (dead name) to one that they choose and aligns with their gender identity. Legal transitioning includes changing gender markers on government-issued documents such as a driver’s license or birth certificate.
Medical and surgical transitions may include hormone replacement therapy or surgical procedures such as breast augmentation, masculine chest reconstruction, or facial feminization surgery.5 Transitioning is a personal decision and not all transgender individuals will choose to achieve gender affirmation through any of these approaches.5,6
Affirming Dental Hygiene Care
Marginalized groups, such as transgender individuals, often face unique stressors such as discrimination, victimization, harassment, or prejudice outside of and within healthcare settings.7 According to the minority stress theory, these stressors can contribute to poorer physical and mental health outcomes due to financial limitations, barriers to healthcare, fear of seeking care from healthcare professionals who are not culturally competent, and concerns of medical confidentiality.8,9
Based on the United States 2020 Transgender Survey (N=27, 715), 30% of transgender respondents experienced a form of health discrimination or did not seek care due to cost.10 Barriers to accessing healthcare often stem from overall cost and lack of coverage, as well as denial of claims due to being transgender. If legal transitioning has not been completed, this can lead to lack of insurance coverage, especially for specific gender-affirming care. Lack of healthcare coverage can lead to diminished preventive services such as check-ups, health screenings for high blood pressure or diabetes, cancer screenings, immunizations, and dental care.
Even when insurance coverage is available, transgender individuals often delay healthcare simply out of fear of discrimination or substandard care. This fear may be related to lack of knowledge and/or bias from providers related to transgender persons.10,11 Oral health professionals need to be knowledgable about this population to provide more inclusive practice settings and individualized patient-centered care.
Documentation and Communication
Documents within the office, such as medical histories or consent forms, should include affirming language such as space for preferred names and/or preferred pronouns. This can easily be added into existing patient forms, as well as integrated into most electronic health record systems. Most insurance companies will require legal name and legal sex within documentation for filing purposes if legal transition has not occurred.12 However, dental practices can ensure transgender patients that this information is used only for insurance purposes and that the preferred name/pronouns are what will be used in the office.
In addition to documentation, nonoffensive verbal communication can establish a trusting relationship and rapport that may counteract many of the barriers that transgender individuals encounter in healthcare settings. Establishing inclusive documentation and communication practices at the start of the appointment can improve the delivery of culturally competent care for transgender patients.
Oral health disparities within the transgender population include higher rates of dental diseases, increased dental anxiety/fear, and difficulty accessing or affording necessary care.8,13 Due to these disparities, oral health professionals should be prepared to identify risk factors and oral conditions commonly seen in this population as well as provide appropriate treatment strategies.
Risk Assessment and Medical History
A thorough review of the patient’s medical history is critical to determine previous health conditions, current medications, and any surgical history. Specific health conditions commonly seen in the transgender population include mental health issues including anxiety/depression, tobacco/alcohol abuse, increased cancer risk, poor cardiovascular health, and higher incidence of sexually transmitted infections (STIs).14,15 Additionally, common pharmacotherapeutics taken for these conditions, such as anti-anxiety and/or antidepression medications or gender-affirming hormone therapy (GAHT), significantly impact the oral cavity. Anti-anxiety and/or antidepression may raise the risk of xerostomia and caries as well as increase the levels of the periodontal pathogen Porphyromonas gingivalis.16,17
GAHT is one of the most common medical treatments for transgender individuals and may include hormone replacements or hormone blockers.8 For example, a transgender woman may be taking estrogen and anti-androgens to suppress the effects of testosterone and elevate the feminine characteristics provided by the estrogen. These sex hormones have a direct and indirect impact on the periodontium, just like normal hormonal fluctuations can affect patients’ oral health status.18 Dental hygienists should complete a thorough review of health history and medication use in order to properly educate patients about any oral health risks.
Caries Risk and Periodontal Considerations
Xerostomia is one of the most common side effects of anti-anxiety and anti-depression medications, raising the risk of caries and poor periodontal health.13 Treatment considerations for transgender individuals with an increased caries risk include caries risk assessments, in-office fluoride applications, and nutritional counseling. In addition to providing treatment, dental hygienists can educate patients on proper at-home oral health strategies, xylitol use, and product recommendations to reduce xerostomia and caries risk.
Furthermore, fluctuations in sex hormones, such as estrogen, progesterone, and testosterone, can affect the epithelial tissues’ response to bacterial biofilm and increase vascular proliferation, contributing to heightened gingival inflammation and bleeding, regardless of oral hygiene status.18,19 Many GAHT medications alter sex hormone levels, leading to higher rates of gingivitis and periodontal diseases among the transgender population.18
Dental hygienists play a critical role in prevention and treatment by providing prophylaxes, scaling in the presence of gingivitis, and initial nonsurgical periodontal therapy. Other possible treatments include frequent (every 3 to 4 months) periodontal maintenance visits, laser therapy, and possible referral to a periodontist for further evaluation. Additionally, thorough oral hygiene instruction can reduce the oral effects of these hormone imbalances.20 At-home oral hygiene care instructions may include selective brushing techniques and interproximal care options with recommendations for oral hygiene aids. Ultimately, oral hygiene education should be tailored to these unique risks.
Oral Cancer and Sexually Transmitted Infection Screening
Due to the high incidence of STIs among the transgender population, oral health professionals should be prepared to identify potential intraoral and extraoral lesions.21,22 Human immunodeficiency virus (HIV), syphilis, gonorrhea, and human papillomavirus (HPV) are common STIs seen in the transgender population.8
Dental hygienists can ensure early detection of potential lesions through comprehensive and routine oral cancer screenings and education for self-screening techniques at home in between routine visits. Possible STI lesions found intraorally may appear as red or white discolorations found near the tongue, soft palate, or tonsillar region and could be palpated during an extraoral exam as swollen lymph nodes. Additionally, patients with oral lesions may require referral to an oral surgeon or other specialist, while those who may be unaware of a possible STI should be referred for appropriate medical evaluation.
Tobacco Cessation
In addition to facing an increased risk of STIs, the transgender community is identified by the US Centers for Disease Control and Prevention as a priority population for tobacco cessation interventions.23 Rates of tobacco use are higher in the transgender population and dental hygienists should be prepared to address this during oral health education.
Starting with medical history, oral health professionals should allow for open dialogue with their patients to determine if they are currently smoking or have a past history of smoking. For patients who currently smoke, clinicians should assess the frequency and quantity of tobacco use to support accurate periodontal staging and grading, treatment planning, and individualized oral hygiene education, particularly when periodontal disease is present. Additionally, discussing tobacco use with patients may also provide oral health professionals assistance with a differential diagnosis when examining intraoral and extraoral lesions.13
Practice Environment and Team Training
Within dental practices, oral health professionals can provide a safe and inclusive environment through easy and minor changes. Providing affirming signage within the office such as displaying lesbian, gay, bisexual, transgender, and queer (LGBTQ+) friendly stickers or flags can alert transgender patients of a safe environment.3
In addition, oral health providers should receive cultural competency training and maintain it through ongoing continuing education courses and workshops. The Commission on Dental Accreditation (CODA) requires cultural competence as part of its accreditation standards to ensure oral health professionals are providing safe and inclusive care for diverse populations.24 All providers within the dental office should receive and maintain cultural competency training specific to the transgender population after completion of a CODA-accredited program through continuing education and workshops.25
Oral health professionals can also keep other colleagues within the office accountable by correcting any noninclusive comments or language. The entire office is responsible for providing a safe environment for all patients, therefore maintaining office education is essential for providing care to transgender patients.
Conclusion
In a 2020 survey by the Center for American Progress, 54% of transgender respondents stated being in poor health and 68% of respondents reported experiencing a form of discrimination or mistreatment by healthcare providers.26 To reduce health and dental disparities within the transgender population, oral health professionals should be well informed about providing equitable, patient-centered care through affirming documentation, communication, clinical assessment, treatment planning and practice environment.
References
- USAFacts. What Percentage of the US Population Is Transgender? Feb 2025. Available at https://usafacts.org/articles/what-percentage-of-the-us-population-is-transgender. Accessed June 5, 2026.
- United States Department of Health and Human Services. Healthy People 2030. Available at https://odphp.health.gov/healthypeople. Accessed June 5, 2026.
- Tamrat J. ‘Trans-forming’ dental practice norms: Exploring transgender identity and oral health implications. Can J Dent Hyg. 2022;56:131-139.
- American Psychological Association. Guidelines for psychological practice with transgender and gender nonconforming people. Am Psychol. 2015;70:832-864.
- American Psychiatric Association. What Is Gender Dysphoria? Available at psychiatry.org/patients-families/gender-dysphoria/what-is-gender-dysphoria. Accessed June 5, 2026.
- American Psychological Association. Understanding Transgender People, Gender Identity, and Gender Expression. Available at apa.org/topics/lgbtq/transgender-people-gender-identity-gender-expression. Accessed June 5, 2026.
- Falck F, Branstrom R. The significance of structural stigma towards transgender people in health care encounters across Europe: Health care access, gender identity disclosure, and discrimination in health care as a function of national legislation and public attitudes. BMC Pub Health. 2023;23: 1-15.
- Macri D, Wolfe K. My preferred pronoun is she: Understanding transgender identity and oral health care needs. Can J Dent Hyg. 2019;53:110-117.
- Frost D, Meyer I. Minority stress theory: Application, critique, and continued relevance. Cur Opinion in Psy. 2023;51: 1-6.
- Kachen A, Pharr J. Health care access and utilization by transgender populations: A United States transgender survey study. Transgend Health. 2020;5:141-148.
- Macdonald DW, Grossoehme DH, Mazzola A, Pestian T, Schwartz SB. Oral health care experiences of transgender adolescents and young adults. J Am Dent Assoc. 2019;150:748-754.
- National LGBT Health Education Center Fenway Institute. Providing Inclusive Services and Care for LGBT People: A Guide for Health Care Staff. Available at lgbtqiahealtheducation.org/wp-content/uploads/Providing-Inclusive-Services-and-Care-for-LGBT-People.pdf. Accessed June 5, 2026.
- Discepolo K, Aquino N. Considerations for transgender patients requiring dental rehabilitation. J Dent Children. 2022;89:46-51.
- Manpreet K, Ajmal MB, Raheel SA. Oral health status among transgender young adults: a cross-sectional study. BMC Oral Health. 2021;21: 1-6.
- Azagba S, de Silva G, Ebling T. Examining general, physical, and mental health disparities between transgender and cisgender adults in the US. Int J Equity in Health. 2025;24: 1-11.
- Kisely S. No mental health without oral health. Canad J Psych. 2016;61:277-282.
- Alcazar-Hernandez J, Pecci-Loret MR, Guerrero-Girones J. Oral manifestations in patients in treatment with antidepressants: A systematic review. J Clin Med. 2024;13: 1-15.
- Patil SN, Kalburgi NB, Koregol AC, et al. Female sex hormones and periodontal health-awareness among gynecologists – a questionnaire survey. Saudi Dent J. 2012;24:99-104
- Markou E, Eleana B, Lazaros T, et al. The influence of sex steroid hormones on gingiva of women. Open Dent J. 2009;9:146-156.
- Sathish AK, Varghese J, Fernandes AJ. The impact of sex hormones on the periodontium during a woman’s lifetime: A concise-review update. Current Oral Health Reports. 2022;9:146-156.
- McNulty A and Bourne C. Transgender HIV and sexually transmissible infections. Sex Health. 2017;14:451-455.
- Samuel SR, Muragaboopathy V, Patil S. Transgender HIV status, self perceived dental care barriers, and residents’ stigma, willingness to treat them in a community dental outreach program: Cross-sectional study. Spec Care Dent. 2018;38:307-312.
- Jamal A, Philips E, Gentzke AS, et al. Current cigarette smoking among adults – United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67:53-59.
- Commission on Dental Accreditation (CODA.) Dental Hygiene Standards. Available at https://coda.ada.org/-/media/project/ada-organization/ada/coda/files/dental_hygiene_standards.pdf?rev=796e0c03f5ee4abca777ac02f9ee83ae&hash=EF22294B07B4E03B065210C5A68D459A. Accessed June 5, 2026.
- Ludwig DC, Morrison SD. Should dental care make a transition? J Am Dent Assoc. 2018;149:79-80.
- Center for American Progress. Discrimination and Experiences of LGBTQ People in the US: 2020 Survey Results. Available at americanprogress.org/article/discrimination-experiences-among-lgbtq-people-us-2020-survey-results. Accessed June 5, 2026.
From Dimensions of Dental Hygiene. July/August 2026; 24(4):40-45
