The Critical Connection Between Endodontic and Periodontal Pathology
There’s growing agreement that endodontic infections can lead to periodontal issues, especially when abscess pressures create sinus tracts into the periodontal ligament. However, periodontal diseases rarely cause pulpal necrosis unless the pocket reaches the apex, creating a pathway for bacterial invasion.
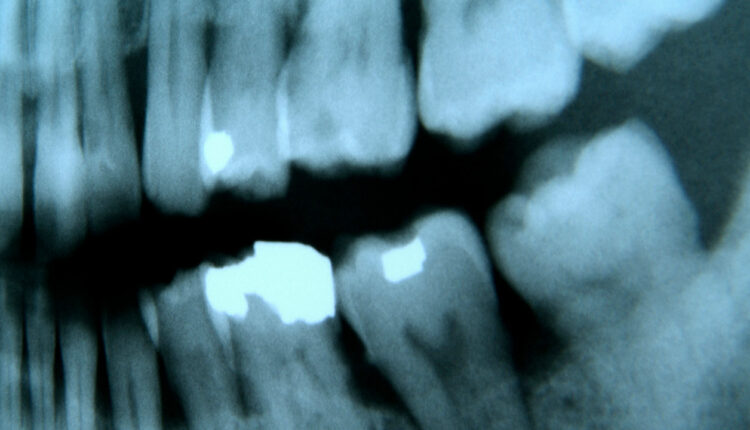
There is agreement between endodontists and periodontists that endodontic pathology can cause periodontal pathology. When the pressures from a dental abscess increase, the purulent exudate will follow the path of least resistance. If this path is through the periodontal ligament, a sinus tract can develop through the sulcus, resulting in a deep periodontal pocket. Pockets arising from pulpal disease should be expected to heal without the need for periodontal treatment (Figures 1A through 1C).1 However, studies indicate that a history of smoking, as well as extensive clinical attachment loss, deep probing depths, and severity of full-mouth periodontitis, are associated with a guarded prognosis for some endodontic-periodontal lesions.2

There is conflicting evidence as to whether periodontal disease can cause pulpal disease. Some investigators have reported pulpal changes, such as inflammation and pulp stones, next to lateral and accessory canals,3,4 whereas other investigators have found no correlation between periodontal disease and pulp histology.5,6 One investigator studied 414 advanced periodontally involved teeth, of which only 3% required root canal treatment.7 From a clinical standpoint, it can therefore be concluded that periodontal disease rarely causes pulpal necrosis due to the exposure of lateral and/or accessory canals.

On the other hand, endodontists and periodontists agree that if a periodontal pocket reaches the apical foramen, the pulp can become necrotic.8 Recent histological evidence has shown that when the periodontal pocket reaches the apex, the blood flow of the apical vessels can become compromised. In turn, bacteria can invade these compromised vessels and serve as avenues for the bacteria to enter the pulp.9

REFERENCES
- Rotstein I, Simon JH. The endo-perio lesion: a critical appraisal of the disease condition. Endod Topics. 2006;13:34–56.
- Fan X, Yu X, Yu S, et al. Prognostic factors of grade 2–3 endo-periodontal lesions treated nonsurgically in patients with periodontitis: A retrospective case-control study. BioMed Res. Int. 2020;2020:1–9.
- Seltzer S, Bender IB, Ziontz M. The interrelationship of pulp and periodontal disease. Oral Surg Oral Med Oral Pathol. 1963;16:1474–1490.
- Rubach WC, Mitchell DF. Periodontal disease, accessory canals and pulp pathosis. J Periodontol. 1965;36:34–38.
- Torabinejad M, Kiger RD. Histologic evaluation of dental pulp tissue of a patient with periodontal disease. Oral Surg Oral Med Oral Pathol. 1985;59:198–200.
- Mazur B, Massler M. Influence of periodontal disease on the dental pulp. Oral Surg Oral Med Oral Pathol. 1964;17:592–603.
- Bergenholtz G, Nyman S. Endodontic complications following periodontal and prosthetic treatment of patients with advanced periodontal disease. J Periodontol. 1984;55:63–68.
- Langeland K, Rodrigues H, Dowden W. Periodontal disease, bacteria, and pulpal histopathology. Oral Surg Oral Med Oral Pathol. 1974;37:257–270.
- Ricucci D, Siqueira JF, Rocas IN. Pulp response to periodontal disease: Novel observations help clarify the process of tissue breakdown and infection. J Endod. 2021;47:740–754.
This information originally appeared in Dunlap CA, Lundergan WP, Dunlap BC. Diagnosis of endodontic-periodontal lesions. Decisions in Dentistry. 2023;9(2):42-45.
