
A Case Study in Managing Peri-Implantitis: A 5-Year Follow-Up
This case study explores the management and treatment of peri-implantitis in a 40-year-old patient 5 years post-implant loading. Detailed surgical intervention, including osseous resective surgery and the replacement of an implant abutment and crown, highlights advancements in addressing peri-implant disease and underscores the need for personalized maintenance plans for long-term implant health.
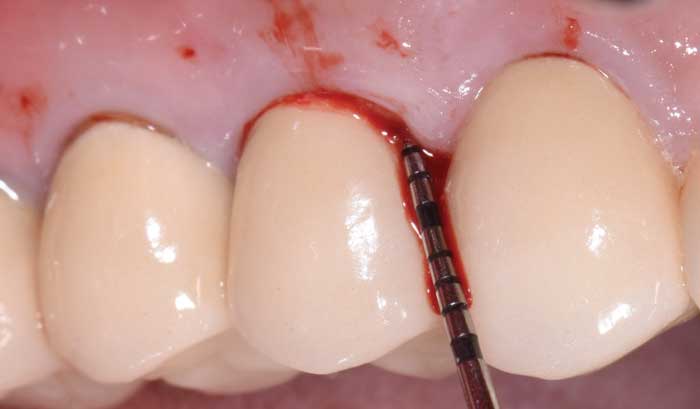
The following case outlines the steps taken to treat peri-implantitis after 5-years post-loading. A 40-year-old woman presented to the graduate periodontics clinic at the University of Texas Health Science Center, San Antonio, School of Dentistry reporting increasing discomfort, bleeding and tenderness around implant #5 (Figure 1 through 8). The patient had a medical history significant for depression and took sertraline. She reported smoking less than 10 cigarettes daily.


The patient’s periodontal tissues were generally pink and healthy, with mild plaque, calculus and debris throughout. The peri-implant tissues around implant #5 were inflamed, with localized vertical intrabony defects. Probing depths ranged from 6 to 8 mm, with moderate bleeding on probing. She reported frequent food impaction between #5 and 6, where an open contact was present. According to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions, she had peri-implantitis.1

After a thorough patient evaluation and review of treatment options, a surgical plan was developed. The procedure would be performed using intravenous conscious sedation. The treatment plan included implant flap debridement, with osseous recontouring or bone grafting. This decision would be made after defect visualization at the time of surgery. The patient was informed that she would need a new crown/abutment at site #5 and/or 6 to close the contact and address any esthetic deficiencies after treatment. Tobacco cessation was also advised.

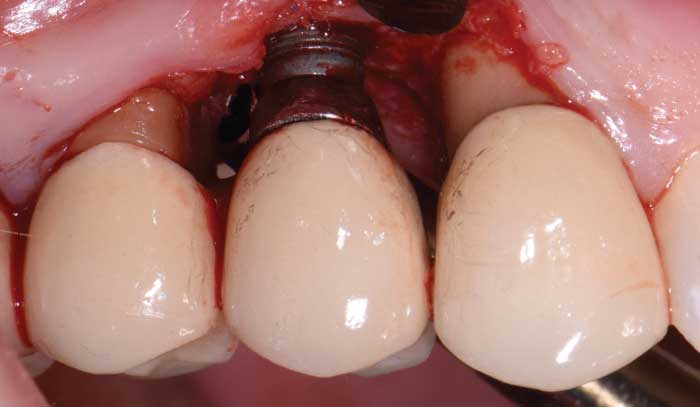
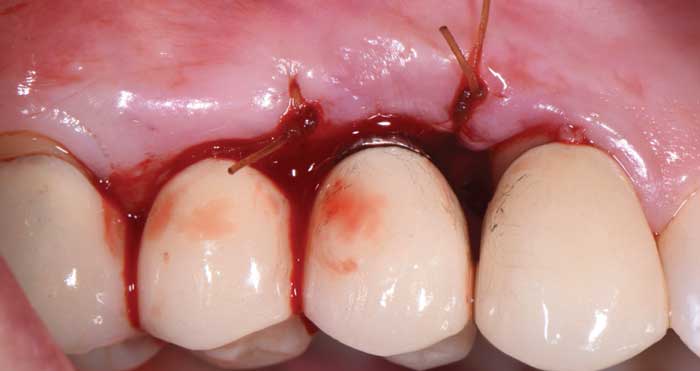
During surgery, full-thickness flaps were elevated to allow for visualization of the intrabony defects. After degranulation with titanium scalers and saline, the defect was not favorable to grafting because it was too broad and shallow. Osseous resective surgery was instead performed to achieve flat, bony architecture around implant #5. Flaps were apically repositioned with resorbable sutures.
After several months of healing, the site was clinically stable, and the patient returned to her restorative dentist for fabrication of a new implant abutment and crown at site #5 and placed on 6-month recare schedule. She was encouraged to use a waterjet around her implant restoration, as there was now a hygienic cleansable space.

Changes in scientific understanding of the pathogenesis of peri-implant disease now dictate how ailing implants should be managed and maintained. It is increasingly important to separate the diagnosis and treatment of periodontal and peri-implant conditions. Current nonsurgical and surgical interventions aim to preserve the titanium dioxide layer using instruments and materials compatible with the implant body, abutment and prosthesis. Maintenance visits and self-care regimens should be customized to meet site-specific and individual needs for long-term health and patient satisfaction.
Reference
- Schwarz F, Derks J, Monje A, Wang H-L. Peri-implantitis. J Clin Periodontol. 2018;45(Suppl 20):S246–S266.
This information originally appeared in Saltz A. Evolving management of peri-implant disease. Decisions in Dentistry. 2021;7(11)16-21.
